You might also like
- 2555 การผลิตและประกันคุณภาพเภสัชตำรับโรงพยาDocument176 pages2555 การผลิตและประกันคุณภาพเภสัชตำรับโรงพยาJeng PharmNo ratings yet
- แนวทางเวชปฏิบัติสำหรับการดูแลผู้ป่วยที่มีอาการแพ้ชนิดรุนแรง พ.ศ.2560Document34 pagesแนวทางเวชปฏิบัติสำหรับการดูแลผู้ป่วยที่มีอาการแพ้ชนิดรุนแรง พ.ศ.2560เด็กชายสมันตภัทร แฟนคลับอาจารย์กวง100% (1)
- คู่มือการใช้ยาอย่างสมเหตุสมผล ทางวิสัญญีและการระงับปวดDocument82 pagesคู่มือการใช้ยาอย่างสมเหตุสมผล ทางวิสัญญีและการระงับปวดStaporn KasemsripitakNo ratings yet
- ความคงสภาพของยาเตรียมเฉพาะคราวในรูปแบบต่างๆDocument22 pagesความคงสภาพของยาเตรียมเฉพาะคราวในรูปแบบต่างๆKani Rapee0% (1)
- WI-PHA-45 - การบริหารจัดการความสอดคล้องต่อเนื่องของยา (medicatio reconciliation) ผู้ป่วยนอกDocument13 pagesWI-PHA-45 - การบริหารจัดการความสอดคล้องต่อเนื่องของยา (medicatio reconciliation) ผู้ป่วยนอกWannaporn SangwarnNo ratings yet
- คู่มือการปรุงยาเฉพาะรายตำรับยากัญชา (ส่วนที่ไม่เป็นยาเสพติดให้โทษ) v.1Document82 pagesคู่มือการปรุงยาเฉพาะรายตำรับยากัญชา (ส่วนที่ไม่เป็นยาเสพติดให้โทษ) v.1sc425000No ratings yet
- 03 36 363 Had 17052560Document167 pages03 36 363 Had 17052560Rungtip Ruangnaparat100% (1)
- MCQ 1-2555 Day 2Document26 pagesMCQ 1-2555 Day 2Covermark Thailand60% (5)
- CQIห้องยา 1Document7 pagesCQIห้องยา 1jirat_iyarapongNo ratings yet
- Scope Ospe Pt1Document1 pageScope Ospe Pt1TiNTiNNo ratings yet
- รวมข้อสอบ MCQ ใบประกอบวิชาชีพเภสัชกรรมDocument29 pagesรวมข้อสอบ MCQ ใบประกอบวิชาชีพเภสัชกรรมCheNo ratings yet
- Daily Log 1 5Document18 pagesDaily Log 1 5Manuschanok SutthipongNo ratings yet
- 1 รูปแบบคลินิกกัญชาทางการแพทย์Document58 pages1 รูปแบบคลินิกกัญชาทางการแพทย์jirat_iyarapongNo ratings yet
- 6. หลักการใช้กัญชาทางการแพทย์แผนไทย PDFDocument243 pages6. หลักการใช้กัญชาทางการแพทย์แผนไทย PDFWaterfall ShapelessNo ratings yet
- CPG CancerDocument570 pagesCPG Cancerba5_numNo ratings yet
- คู่มือคลินิกกัญชาทางการแพทย์แผนไทยฉบับวันที่ ๑๖ - ๑๗ กันยายน ๒๕๖๒Document66 pagesคู่มือคลินิกกัญชาทางการแพทย์แผนไทยฉบับวันที่ ๑๖ - ๑๗ กันยายน ๒๕๖๒Jagravudh PuagkongNo ratings yet
- Drug Interaction Ha61 PDFDocument66 pagesDrug Interaction Ha61 PDFbuaby005No ratings yet
- 02 Muscle RelaxantsDocument12 pages02 Muscle RelaxantsVathSanNo ratings yet
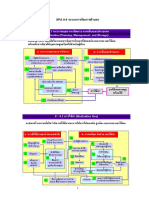
- SPA Part II CH 6 Medication Management SyDocument26 pagesSPA Part II CH 6 Medication Management SyNanthicha MkplNo ratings yet
- คำแนะนำการใช้กัญชาทางการแพทย์Document18 pagesคำแนะนำการใช้กัญชาทางการแพทย์ศาสตรา คำมุลตรีNo ratings yet
- II6 Sar2022 - Draft1Document65 pagesII6 Sar2022 - Draft1Nattapatt LimloustrakulNo ratings yet
- Slide Antimicrobial Stewardship ProgramDocument20 pagesSlide Antimicrobial Stewardship ProgramWeerapat SriraksaNo ratings yet
- AC Chemotherapy HADDocument16 pagesAC Chemotherapy HADNeenuch Maneenuch100% (1)
- กลไกการส่งเสริมการใช้สมุนไพรไทยDocument10 pagesกลไกการส่งเสริมการใช้สมุนไพรไทยThawatchai NajaikongNo ratings yet
- tbps2012 1 23-40Document18 pagestbps2012 1 23-40bangbon drugstoreNo ratings yet
- Soap TBDocument12 pagesSoap TBวิภาวนันท์ จรลีNo ratings yet
- Sar Med 2565Document18 pagesSar Med 2565Nattapatt LimloustrakulNo ratings yet
- Concurrent TriggerDocument25 pagesConcurrent Triggerjya promNo ratings yet
- แนวทางการป้องกันความคลาดเคลื่อนทางยารพ สต 2567Document6 pagesแนวทางการป้องกันความคลาดเคลื่อนทางยารพ สต 2567saisuda.sr.pharmacyNo ratings yet
- UntitledDocument35 pagesUntitledchainat hospitolNo ratings yet
- 6 Drugs Used in OphthalmologyDocument16 pages6 Drugs Used in OphthalmologyKittipong PoolketkitNo ratings yet
- Thai P Harm Health Sciences 2012Document7 pagesThai P Harm Health Sciences 2012Ashok SinhaNo ratings yet
- pc4 โรงพยาบาล HADDocument67 pagespc4 โรงพยาบาล HADbuaby005No ratings yet
- แนวทางเวชปฏิบัติของแพทย์ทั่วไปสำหรับการรักษาผู้ป่วยโรคจิตDocument69 pagesแนวทางเวชปฏิบัติของแพทย์ทั่วไปสำหรับการรักษาผู้ป่วยโรคจิตsomsur2001No ratings yet
- 2914-Article Text-8485-9369-10-20121227Document5 pages2914-Article Text-8485-9369-10-20121227Taory AnisNo ratings yet
- e Rdu-รพ.โนนสูง ภญ.สุทธินีDocument75 pagese Rdu-รพ.โนนสูง ภญ.สุทธินีSurasit SukseeluangNo ratings yet
- การดูแลผู้ป่วยปวดท้องเฉียบพลันDocument23 pagesการดูแลผู้ป่วยปวดท้องเฉียบพลันSawanyaPrammanakulNo ratings yet
- เเนวทางควคุมวัณโรค PDFDocument177 pagesเเนวทางควคุมวัณโรค PDFMui Weawpunyasin RxSuNo ratings yet
- Document 2Document19 pagesDocument 2นันทสิทธิ์ ศิริวิชญ์ไมตรีNo ratings yet
- Ospe 2558 PDFDocument1 pageOspe 2558 PDF037 Onpreeya LansaiNo ratings yet
- Injectable 64Document46 pagesInjectable 64Kanyawee LerNo ratings yet
- 2725-Article Text-8019-8854-10-20121001Document8 pages2725-Article Text-8019-8854-10-20121001นุสรา วราวุฒิNo ratings yet
- 9968 - File - CPG RDUDocument2 pages9968 - File - CPG RDUปกรณ์ธรรม เพชรแสนค่าNo ratings yet
- คู่มือการป้องกันการติดเชื้อในโรงพยาบาลDocument122 pagesคู่มือการป้องกันการติดเชื้อในโรงพยาบาลNj Nursing NursingNo ratings yet
- รายงานตอบคำถาม 2Document15 pagesรายงานตอบคำถาม 2Nathakorn RodklongtanNo ratings yet
- หมวดที่ 4 ข้อ 4.6 การจัดบริการเภสัชกรรม RDU และ คDocument51 pagesหมวดที่ 4 ข้อ 4.6 การจัดบริการเภสัชกรรม RDU และ คNattamon KosajanNo ratings yet
- sharefilefile 3224.ภาคผนวก๒เปรียบเทียบสมรรถนะร่วมและสมรรถนะสาขาบริบาลเภสัชกรรม PDFDocument3 pagessharefilefile 3224.ภาคผนวก๒เปรียบเทียบสมรรถนะร่วมและสมรรถนะสาขาบริบาลเภสัชกรรม PDFjya promNo ratings yet
- Drug - eruption สมาคมโรดผิวหนังDocument6 pagesDrug - eruption สมาคมโรดผิวหนังUdsanee SukpimonphanNo ratings yet
- AC ambu ผลัด 2 เสร็จ PDFDocument24 pagesAC ambu ผลัด 2 เสร็จ PDFBeau PhatruetaiNo ratings yet
- รายงานการศิกษาประสิทธิผลรักษาและความปลอดภัยของยายับยั้งการหลั่งกรด PPIDocument130 pagesรายงานการศิกษาประสิทธิผลรักษาและความปลอดภัยของยายับยั้งการหลั่งกรด PPIvilaNo ratings yet
- การทบทวนคำสั่งใช้ยา-เภสัชกร - 14032563Document24 pagesการทบทวนคำสั่งใช้ยา-เภสัชกร - 14032563Atawit SomsiriNo ratings yet
- 2012-01-20acute Care Manual 2011, LPHDocument136 pages2012-01-20acute Care Manual 2011, LPHBongkotchakorn Mind PhonchaiNo ratings yet
- กรณีศึกษาDocument18 pagesกรณีศึกษาGoy BubbiesNo ratings yet
- ปรับปรุง 2567Document10 pagesปรับปรุง 2567roongtippNo ratings yet
- MedicainalCannabisBook v4-1Document60 pagesMedicainalCannabisBook v4-1sc425000No ratings yet
- บทความงานวิจัยDocument12 pagesบทความงานวิจัยKanyawee LerNo ratings yet