You might also like
- Critical Care Review: Airway Management of The Critically Ill PatientDocument16 pagesCritical Care Review: Airway Management of The Critically Ill PatientNikita ShakyaNo ratings yet
- Secuencia de Intubación RápidaDocument16 pagesSecuencia de Intubación Rápidaalis_maNo ratings yet
- Rapid Sequence Intubation and Cricoid PressureDocument16 pagesRapid Sequence Intubation and Cricoid PressureErlin IrawatiNo ratings yet
- 1 s2.0 S0733862722000384 MainDocument13 pages1 s2.0 S0733862722000384 Maincoca12451No ratings yet
- 4.-Rapid Sequence Intubation in Adults - Uptodate PDFDocument14 pages4.-Rapid Sequence Intubation in Adults - Uptodate PDFkendramura100% (1)
- Obesity and Anticipated Difficult Airway - A Comprehensive Approach With Videolaryngoscopy, Ramp Position, Sevoflurane and Opioid Free AnaesthesiaDocument8 pagesObesity and Anticipated Difficult Airway - A Comprehensive Approach With Videolaryngoscopy, Ramp Position, Sevoflurane and Opioid Free AnaesthesiaIJAR JOURNALNo ratings yet
- 2022 Preoperative Assessment Premedication Perioperative DocumentationDocument38 pages2022 Preoperative Assessment Premedication Perioperative DocumentationMohmmed Mousa100% (1)
- AARC Clinical Practice GuidelineDocument7 pagesAARC Clinical Practice GuidelineXime GonzálezNo ratings yet
- Ventilatorweaningand Extubation: Karen E.A. Burns,, Bram Rochwerg, Andrew J.E. SeelyDocument18 pagesVentilatorweaningand Extubation: Karen E.A. Burns,, Bram Rochwerg, Andrew J.E. Seelyأركان هيلث Arkan healthNo ratings yet
- Essentials in Lung TransplantationFrom EverandEssentials in Lung TransplantationAllan R. GlanvilleNo ratings yet
- Smith 2001Document19 pagesSmith 2001PaulHerreraNo ratings yet
- Freid 2005Document14 pagesFreid 2005PaulHerreraNo ratings yet
- Airway Management in The Obese Patient: William A. LoderDocument6 pagesAirway Management in The Obese Patient: William A. LoderTapas Kumar SahooNo ratings yet
- Rapid Sequence Intubation For Adults Outside The Operating RoomDocument12 pagesRapid Sequence Intubation For Adults Outside The Operating Roomjohnsam93No ratings yet
- Evid TT 2200305Document4 pagesEvid TT 2200305Muthia Farah AshmaNo ratings yet
- Anesthesia in Prehospital Emergencies and in The Emergency DepartmentDocument7 pagesAnesthesia in Prehospital Emergencies and in The Emergency DepartmentIvan TapiaNo ratings yet
- Practice Guidelines For Preoperative FastingDocument18 pagesPractice Guidelines For Preoperative FastingTaufik RachmanNo ratings yet
- Physiotherapy in The ICUDocument10 pagesPhysiotherapy in The ICUakheel ahammedNo ratings yet
- Effect of Smoking On Intraoperative Sputum and Postoperative Pulmonary Complication in Minor Surgical PatientsDocument7 pagesEffect of Smoking On Intraoperative Sputum and Postoperative Pulmonary Complication in Minor Surgical PatientsfellaniellaNo ratings yet
- Pediatric Rapid Sequence Intubation - An In-Depth ReviewDocument12 pagesPediatric Rapid Sequence Intubation - An In-Depth ReviewDiego LatorreNo ratings yet
- Rapid Sequence Intubation in Adults For Emergency Medicine and Critical Care - UpToDateDocument41 pagesRapid Sequence Intubation in Adults For Emergency Medicine and Critical Care - UpToDateFabio FreitasNo ratings yet
- 2015 LeeuwenbergDocument10 pages2015 LeeuwenbergPaulHerreraNo ratings yet
- Maximizing Success With Rapid Sequence IntubationsDocument11 pagesMaximizing Success With Rapid Sequence IntubationsRaymond RosarioNo ratings yet
- Prehospital Rsi ManualDocument20 pagesPrehospital Rsi ManualMiguel XanaduNo ratings yet
- Articulo de Indice de SecrecionesDocument7 pagesArticulo de Indice de Secrecionesmariam.husseinjNo ratings yet
- The Physiologically Difficult Airway: Eview RticleDocument9 pagesThe Physiologically Difficult Airway: Eview RticleEdson Llerena SalvoNo ratings yet
- Farmacologia en SIRDocument19 pagesFarmacologia en SIRFranklin Correa PrietoNo ratings yet
- Greater Sydney Area Hems Prehospital Rsi Manual: Version 2.1 Oct 2012Document20 pagesGreater Sydney Area Hems Prehospital Rsi Manual: Version 2.1 Oct 2012Juan Antonio GarcíaNo ratings yet
- Enhancing Pulmonary Function and Arterial Blood GaDocument12 pagesEnhancing Pulmonary Function and Arterial Blood Gaاحمد العايديNo ratings yet
- Module 1 Case StudyDocument7 pagesModule 1 Case StudyDivine ParagasNo ratings yet
- Secuencia Rapida GuiasDocument29 pagesSecuencia Rapida GuiasToñoGomezNo ratings yet
- Anesthesia For Bariatric Surgery Practice Guideline - Approved 4 - 9 - 2018 - KAPC - PDF PDFDocument4 pagesAnesthesia For Bariatric Surgery Practice Guideline - Approved 4 - 9 - 2018 - KAPC - PDF PDFHIRANGERNo ratings yet
- Myasthenia Gravis Multiple Sclerosis Case FileDocument3 pagesMyasthenia Gravis Multiple Sclerosis Case Filehttps://medical-phd.blogspot.comNo ratings yet
- Atracurio Vs CisatracurioDocument6 pagesAtracurio Vs CisatracurioEdisonANo ratings yet
- Trends in Anasthesia and Critical CareDocument6 pagesTrends in Anasthesia and Critical CareNurLatifah Chairil AnwarNo ratings yet
- Acute Life-Threatening Hypoxemia During Mechanical VentilationDocument8 pagesAcute Life-Threatening Hypoxemia During Mechanical VentilationCesar Rivas CamposNo ratings yet
- Rapid Sequence Intubation: BackgroundDocument8 pagesRapid Sequence Intubation: Backgroundmarsh86No ratings yet
- RCT of Aprv Vs LPV in Ards PtsDocument11 pagesRCT of Aprv Vs LPV in Ards PtsOldriana Prawiro HapsariNo ratings yet
- Airway Covid - 19Document37 pagesAirway Covid - 19Monica Herdiati Rukmana NaibahoNo ratings yet
- Oral and Maxillofacial Surgery Clinics of North America Office Based Anesthesia 45 57Document13 pagesOral and Maxillofacial Surgery Clinics of North America Office Based Anesthesia 45 57Max FaxNo ratings yet
- Symposium Papers: Emergency Airway ManagementDocument10 pagesSymposium Papers: Emergency Airway Managementdewin21No ratings yet
- 37 Iajps37112017 PDFDocument4 pages37 Iajps37112017 PDFBaru Chandrasekhar RaoNo ratings yet
- Kali Bichromicum 30C For COPD 2005Document8 pagesKali Bichromicum 30C For COPD 2005Dr. Nancy MalikNo ratings yet
- Mechanical Ventilator Discontinuation Process: Lingye Chen,, Daniel Gilstrap,, Christopher E. CoxDocument7 pagesMechanical Ventilator Discontinuation Process: Lingye Chen,, Daniel Gilstrap,, Christopher E. CoxGhost11mNo ratings yet
- Determinants of Time-To-Weaning in A Specialized Respiratory Care UnitDocument10 pagesDeterminants of Time-To-Weaning in A Specialized Respiratory Care UnitClaudia IsabelNo ratings yet
- Determinants of Time-To-Weaning in A Specialized Respiratory Care UnitDocument10 pagesDeterminants of Time-To-Weaning in A Specialized Respiratory Care UnitClaudia IsabelNo ratings yet
- Comparative Study of Breathing Techniques After Coronary Artery by Pass GraftingDocument12 pagesComparative Study of Breathing Techniques After Coronary Artery by Pass GraftingJulenda CintarinovaNo ratings yet
- 2 DiaphragmaticExcursionDocument5 pages2 DiaphragmaticExcursionTiago XavierNo ratings yet
- Masoomeh Adib, Atefeh Ghanbari, Cyrus Emir Alavi and Ehsan Kazemnezhad LeyliDocument9 pagesMasoomeh Adib, Atefeh Ghanbari, Cyrus Emir Alavi and Ehsan Kazemnezhad LeyliBoy MadNo ratings yet
- Should Patients Be Able To Follow Commands Prior To IonDocument10 pagesShould Patients Be Able To Follow Commands Prior To IonjuliasimonassiNo ratings yet
- Extubation With or Without Spontaneous Breathing TrialDocument9 pagesExtubation With or Without Spontaneous Breathing TrialPAULA SORAIA CHENNo ratings yet
- Maggiore 2013Document10 pagesMaggiore 2013oman hendiNo ratings yet
- NCM 112 (FINALS) Chap 1Document2 pagesNCM 112 (FINALS) Chap 1MikasaNo ratings yet
- ERAS Protocols in TB EmpyemaDocument6 pagesERAS Protocols in TB EmpyemaMohan VenkateshNo ratings yet
- Ards Prone PositionDocument9 pagesArds Prone PositionAnonymous XHK6FgHUNo ratings yet
- Jerath2020 Article InhalationalVolatile-basedSedaDocument4 pagesJerath2020 Article InhalationalVolatile-basedSedasncr.gnyNo ratings yet
- Webinar Kuliah Umum Anestesi Joglo Semar 17 Juni 2020Document95 pagesWebinar Kuliah Umum Anestesi Joglo Semar 17 Juni 2020izaNo ratings yet
- Terapia Adjunta en SdraDocument23 pagesTerapia Adjunta en SdraMarcoNo ratings yet
- RSI - Children 2 PDFDocument6 pagesRSI - Children 2 PDFAbdul RachmanNo ratings yet
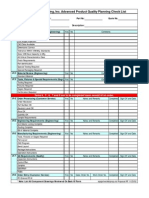
- Voisard Manufacturing, Inc. Advanced Product Quality Planning Check ListDocument1 pageVoisard Manufacturing, Inc. Advanced Product Quality Planning Check ListzaheermechNo ratings yet
- Total Quality Management Must Know" Concepts For EngineersDocument28 pagesTotal Quality Management Must Know" Concepts For EngineerszaheermechNo ratings yet
- Training Schedule PWIDocument1 pageTraining Schedule PWIzaheermechNo ratings yet
- Cswip 3.1 Welding Inspector - Multiple Choice Question, Dec 7, 2007Document43 pagesCswip 3.1 Welding Inspector - Multiple Choice Question, Dec 7, 2007claytoninf87% (30)
- CSWIP Plate Tr5. WPK Rev2Document4 pagesCSWIP Plate Tr5. WPK Rev2razormeback100% (1)
- Physical Configuration Audit (PCA) ChecklistDocument2 pagesPhysical Configuration Audit (PCA) ChecklistzaheermechNo ratings yet
- Preventive Maintenance of MachinesDocument6 pagesPreventive Maintenance of MachineszaheermechNo ratings yet
- ISO Standards Collection - CranesDocument4 pagesISO Standards Collection - CranesJosé Rezende0% (1)
- Functional Configuration Audit (FCA) Checklist: RequirementsDocument2 pagesFunctional Configuration Audit (FCA) Checklist: RequirementszaheermechNo ratings yet
- Passive and Low Frequency RadarDocument11 pagesPassive and Low Frequency RadarzaheermechNo ratings yet
- Pca Checklist: RestrictedDocument3 pagesPca Checklist: RestrictedzaheermechNo ratings yet
- FCA Checklist (NASA)Document2 pagesFCA Checklist (NASA)zaheermechNo ratings yet
- Guide To Insulation Product Specifications: ASTM Guides, Practices and Test MethodsDocument24 pagesGuide To Insulation Product Specifications: ASTM Guides, Practices and Test MethodszaheermechNo ratings yet
- A Powerpoint Training Presentation: by Keith H. CooperDocument38 pagesA Powerpoint Training Presentation: by Keith H. CooperzaheermechNo ratings yet
- ACCP Professional Level III Initial Qualification RequirementsDocument1 pageACCP Professional Level III Initial Qualification RequirementszaheermechNo ratings yet
- EXAMPLE CalculationsDocument4 pagesEXAMPLE CalculationszaheermechNo ratings yet
- Gant ChartDocument2 pagesGant ChartzaheermechNo ratings yet
- Denso HP4Document87 pagesDenso HP4Abraham Janco Janco100% (2)
- Thesis TopicsDocument9 pagesThesis TopicsInayath AliNo ratings yet
- dnd3 Character Sheet STD 105cDocument2 pagesdnd3 Character Sheet STD 105cGerry MaloneyNo ratings yet
- PRP RationaleDocument12 pagesPRP Rationalemarquezjayson548No ratings yet
- ReflectionDocument2 pagesReflectionBảo HàNo ratings yet
- A Crude Awakening Video NotesDocument3 pagesA Crude Awakening Video NotesTai NguyenNo ratings yet
- Individual Ability in SoftwareDocument9 pagesIndividual Ability in Softwaredhana0809100% (4)
- CREW Whitaker Recusal Letter DOJ 11-8-2018Document9 pagesCREW Whitaker Recusal Letter DOJ 11-8-2018Beverly TranNo ratings yet
- Airplus CDF3 Technical SpecsDocument38 pagesAirplus CDF3 Technical Specssadik FreelancerNo ratings yet
- Distortion of The Ecclesiological Views of Metropolitan Chrysostomos of PhlorinaDocument11 pagesDistortion of The Ecclesiological Views of Metropolitan Chrysostomos of PhlorinaHibernoSlavNo ratings yet
- Name: - Date: - Week/s: - 2 - Topic: Examining Trends and FadsDocument3 pagesName: - Date: - Week/s: - 2 - Topic: Examining Trends and FadsRojelyn Conturno100% (1)
- Kindergarten ArchitectureDocument65 pagesKindergarten ArchitectureAnushka Khatri83% (6)
- Report End of Chapter 1Document4 pagesReport End of Chapter 1Amellia MaizanNo ratings yet
- Proofreading: Basic Guide (Research)Document34 pagesProofreading: Basic Guide (Research)Mary Christelle100% (1)
- Biologic and Biophysical Technologies. FINALDocument28 pagesBiologic and Biophysical Technologies. FINALRafael Miguel MallillinNo ratings yet
- SwahiliDocument7 pagesSwahiliMohammedNo ratings yet
- Content Kartilya NG Katipunan: Kataastaasan, Kagalanggalangang Katipunan NG Mga Anak NG Bayan)Document6 pagesContent Kartilya NG Katipunan: Kataastaasan, Kagalanggalangang Katipunan NG Mga Anak NG Bayan)AngelaNo ratings yet
- CPP CheatsheetDocument10 pagesCPP CheatsheetPrakash GavelNo ratings yet
- RagragsakanDocument6 pagesRagragsakanRazel Hijastro86% (7)
- Implementasi Fault Management (Manajemen Kesalahan) Pada Network Management System (NMS) Berbasis SNMPDocument11 pagesImplementasi Fault Management (Manajemen Kesalahan) Pada Network Management System (NMS) Berbasis SNMPIwoncl AsranNo ratings yet
- Natural Gas DistributionDocument46 pagesNatural Gas DistributionscribdmisraNo ratings yet
- The Spokesman Weekly Vol. 32 No. 39 May 30, 1983Document12 pagesThe Spokesman Weekly Vol. 32 No. 39 May 30, 1983SikhDigitalLibraryNo ratings yet
- Small Incision Cataract SurgeryDocument249 pagesSmall Incision Cataract SurgeryAillen YovitaNo ratings yet
- My Kindergarten BookDocument48 pagesMy Kindergarten BookfranciscoNo ratings yet
- Detergent For Auto DishWashing Machine EDocument5 pagesDetergent For Auto DishWashing Machine EkaltoumNo ratings yet
- Pale ExamDocument4 pagesPale ExamPatrick Tan100% (1)
- Material Safety Data Sheet: Manufacturer Pt. Bital AsiaDocument3 pagesMaterial Safety Data Sheet: Manufacturer Pt. Bital AsiaediNo ratings yet
- E9d30c8 4837smartDocument1 pageE9d30c8 4837smartSantoshNo ratings yet
- Exercise No. 2 (DCC First and Second Summary)Document3 pagesExercise No. 2 (DCC First and Second Summary)Lalin-Mema LRNo ratings yet
- Literature ReviewDocument7 pagesLiterature Reviewapi-353923446No ratings yet