You might also like
- Alcohol, Drugs, Genes and the Clinical Laboratory: An Overview for Healthcare and Safety ProfessionalsFrom EverandAlcohol, Drugs, Genes and the Clinical Laboratory: An Overview for Healthcare and Safety ProfessionalsRating: 5 out of 5 stars5/5 (1)
- Competing Thru The New Marketing MixDocument6 pagesCompeting Thru The New Marketing MixRM ValenciaNo ratings yet
- Activity 4 - LeucovorinDocument1 pageActivity 4 - LeucovorinMelissa Fatima Laurente DosdosNo ratings yet
- Performance Enhancing Drug AbuDocument7 pagesPerformance Enhancing Drug AbuUAE TECHNo ratings yet
- Doping in Sport: Side Effects of DopingDocument4 pagesDoping in Sport: Side Effects of Dopingiilm002No ratings yet
- Enha Ncement Drugs Andtheathlete: Francesco Botr E, Antonio PavanDocument16 pagesEnha Ncement Drugs Andtheathlete: Francesco Botr E, Antonio PavanDanijel DamnjanovicNo ratings yet
- BR J Sports Med 1975 Articles 58 9Document3 pagesBR J Sports Med 1975 Articles 58 9samawayNo ratings yet
- Doping in SportsDocument3 pagesDoping in SportsDanica Marie RegaladoNo ratings yet
- DinaDocument19 pagesDinaelizabetaNo ratings yet
- Legal Aspects of Drug Testing in Sports LawDocument6 pagesLegal Aspects of Drug Testing in Sports Lawmansi rathiNo ratings yet
- WADA Presentation FinalDocument30 pagesWADA Presentation Finalcooladeel233100% (1)
- Wada Prohibited List: Bull'S Eye On DopingDocument3 pagesWada Prohibited List: Bull'S Eye On DopingDong Hao SimNo ratings yet
- Doping Short VersionDocument3 pagesDoping Short VersionSaber NouiraNo ratings yet
- The Role of The Pharmacist in The Fight Against Doping in SportDocument4 pagesThe Role of The Pharmacist in The Fight Against Doping in SportVanessa SoaresNo ratings yet
- Uso de Farmacos en Los Deportistas y Riesgos de DopajeDocument28 pagesUso de Farmacos en Los Deportistas y Riesgos de DopajeMarta AntunezNo ratings yet
- DopingDocument5 pagesDopingTamara ArsicNo ratings yet
- Summary of Major Modifications and Explanatory Notes: Prohibited SubstancesDocument10 pagesSummary of Major Modifications and Explanatory Notes: Prohibited SubstancesEngie GamezNo ratings yet
- The Sports Doping ShenaniganDocument5 pagesThe Sports Doping ShenaniganYash BhatnagarNo ratings yet
- Drugs and Doping in SportDocument39 pagesDrugs and Doping in SportAbhijit Sharma100% (1)
- Type of Probihited Drugs in Sports Based On WadaDocument14 pagesType of Probihited Drugs in Sports Based On WadaunknownmeNo ratings yet
- The IAAF Anti-Doping Athlete's Guide PDFDocument21 pagesThe IAAF Anti-Doping Athlete's Guide PDFΣΤΕΦΑΝΟΣ ΜΑΤΑΚΗΣNo ratings yet
- Unit - 2 - Dope TestingDocument25 pagesUnit - 2 - Dope TestingMuskaan BindalNo ratings yet
- Debate Is Drugs Testing in Athletes JustifiedDocument2 pagesDebate Is Drugs Testing in Athletes JustifiedCristianNo ratings yet
- A Comprehensive Review On Current Analytical Approaches Used For TheDocument18 pagesA Comprehensive Review On Current Analytical Approaches Used For Thekassim AliNo ratings yet
- Drugs in SportDocument6 pagesDrugs in SportAbdul Razak MansorNo ratings yet
- Sports Corruption: The History and Challenges of Anti-Doping Regimes in The U.S. and AbroadDocument4 pagesSports Corruption: The History and Challenges of Anti-Doping Regimes in The U.S. and AbroadCenter for the Advancement of Public IntegrityNo ratings yet
- Torts Project MasudaDocument18 pagesTorts Project MasudaPratham MohantyNo ratings yet
- People.: HN Aal NDDocument4 pagesPeople.: HN Aal NDkugaugafNo ratings yet
- 11.play Fair NDPSDocument3 pages11.play Fair NDPSTshewang DemaNo ratings yet
- 3.1.2. The Prohibited List and Monitored SubstancesDocument2 pages3.1.2. The Prohibited List and Monitored SubstancesUpadhayayAnkurNo ratings yet
- Doping in SportsDocument9 pagesDoping in Sportsursvenki4ever3793No ratings yet
- Doping in Sports: Current Review: April 2013Document5 pagesDoping in Sports: Current Review: April 2013RITESH MADRECHANo ratings yet
- 16complete Penokok DietDocument96 pages16complete Penokok DietJAKLIN EMPOLNo ratings yet
- Doping in SportsDocument11 pagesDoping in SportsRITESH MADRECHANo ratings yet
- Annual Banned-Substance ReviewDocument20 pagesAnnual Banned-Substance ReviewRuben_Monroy_ClaudioNo ratings yet
- This House Would Permit The Use of Performance Enhancing Drugs in Professional SportsDocument7 pagesThis House Would Permit The Use of Performance Enhancing Drugs in Professional Sportssamimi binti abdul rahmanNo ratings yet
- 10.1007@s40618 019 01145 ZDocument11 pages10.1007@s40618 019 01145 ZVale GrudNo ratings yet
- The World Anti-Doping Code in Olympic and International SportDocument2 pagesThe World Anti-Doping Code in Olympic and International SportUpadhayayAnkurNo ratings yet
- Ifbb Education Ebook The Anti-Doping in Sport DDocument82 pagesIfbb Education Ebook The Anti-Doping in Sport Djose valdiviaNo ratings yet
- 10 DopinginsportsIJCRRDocument5 pages10 DopinginsportsIJCRRZunaira YasinNo ratings yet
- Foods 09 01012Document21 pagesFoods 09 01012chmontero21No ratings yet
- Research Paper Sports Law Tia SachdevaDocument8 pagesResearch Paper Sports Law Tia SachdevaTia SachdevaNo ratings yet
- 2006 Steroids Report: Prepared by The Steroids Working Group United States Sentencing CommissionDocument32 pages2006 Steroids Report: Prepared by The Steroids Working Group United States Sentencing CommissionlosangelesNo ratings yet
- Performance-Enhancing Drugs in Sports: How Chemists Catch UsersDocument2 pagesPerformance-Enhancing Drugs in Sports: How Chemists Catch UsersJuan Daniel EriraNo ratings yet
- Assignment: Name - Aisha Fatima Course - Physiotherapy Year-4th YearDocument2 pagesAssignment: Name - Aisha Fatima Course - Physiotherapy Year-4th YearMuhammad ZaibNo ratings yet
- AdamasDocument46 pagesAdamasMuhammad AriffuddinNo ratings yet
- Pharmacy: Exploring Knowledge, Attitudes and Abuse Concerning Doping in Sport Among Syrian Pharmacy StudentsDocument13 pagesPharmacy: Exploring Knowledge, Attitudes and Abuse Concerning Doping in Sport Among Syrian Pharmacy Studentssome buddyyNo ratings yet
- Research Paper Drug Abuse in AthletesDocument17 pagesResearch Paper Drug Abuse in Athletesnjerunick3060No ratings yet
- DOPNIGDocument10 pagesDOPNIGShashi Bhan tiwariNo ratings yet
- The Regulation of Doping in U.S. and International Sports Introduction: Doping in SportDocument3 pagesThe Regulation of Doping in U.S. and International Sports Introduction: Doping in SportUpadhayayAnkurNo ratings yet
- HEOC - Performance Enhancing Drugs and Risk Decision MakingDocument42 pagesHEOC - Performance Enhancing Drugs and Risk Decision MakingPurdieparkerNo ratings yet
- Draft Notice Comments Guidance Doc Supplements Sportspersons 16-03-2018Document27 pagesDraft Notice Comments Guidance Doc Supplements Sportspersons 16-03-2018Kavita YadavNo ratings yet
- Validation of A LC-MS-MS Method For Anabolic Steroids in Nutritional SupplementsDocument20 pagesValidation of A LC-MS-MS Method For Anabolic Steroids in Nutritional SupplementsnamiraNo ratings yet
- Anti-Doping Presentation: A Resource For Cgas To Present To Athletes and Team OfficialsDocument20 pagesAnti-Doping Presentation: A Resource For Cgas To Present To Athletes and Team OfficialsAjay Pal NattNo ratings yet
- Anabolic Steroids-BDocument5 pagesAnabolic Steroids-BGideon MurathaNo ratings yet
- Jurnal Nutrition BaruDocument11 pagesJurnal Nutrition BaruNursahanizaNo ratings yet
- The Athlete Biological Passport: An Integral Element of Innovative Strategies in AntidopingDocument4 pagesThe Athlete Biological Passport: An Integral Element of Innovative Strategies in AntidopingCitra AntonNo ratings yet
- About Anti-Doping Lab QatarDocument10 pagesAbout Anti-Doping Lab QatarAnti-Doping Lab QatarNo ratings yet
- Foundation Level - Anti DopingDocument9 pagesFoundation Level - Anti DopingAbhishek RawatNo ratings yet
- A Brief Review of Higher Dietary Protein Diets in Weight Loss - A Focus On AthletesDocument9 pagesA Brief Review of Higher Dietary Protein Diets in Weight Loss - A Focus On AthletesDenis LordanNo ratings yet
- Samvel 2019 A Review of Eu Regulation of Sports Nutrition Same Game Different RulesDocument24 pagesSamvel 2019 A Review of Eu Regulation of Sports Nutrition Same Game Different Ruleskristina sutevskaNo ratings yet
- The Use and Misuse of Performance-Enhancing Substances in SportDocument5 pagesThe Use and Misuse of Performance-Enhancing Substances in SportAbhishek JainNo ratings yet
- Basic Concepts in Toxicology - FDocument90 pagesBasic Concepts in Toxicology - FKhokonNo ratings yet
- Attock Demand Week 4Document26 pagesAttock Demand Week 4Salman PervaizNo ratings yet
- 83-Article Text-253-1-10-20151213Document9 pages83-Article Text-253-1-10-20151213KumarNo ratings yet
- 4344 8343 2 PBDocument7 pages4344 8343 2 PBI'm DekuuNo ratings yet
- List of Books - Pharmacology: Authorname Book Title Publisher EditionDocument2 pagesList of Books - Pharmacology: Authorname Book Title Publisher EditionAsiya ZaidiNo ratings yet
- DivalproexDocument2 pagesDivalproexeefrheelNo ratings yet
- Top 200 Pharmaceuticals 2021V2Document1 pageTop 200 Pharmaceuticals 2021V2Amin AminiradNo ratings yet
- Factors Affecting Inter Individual Variations in Drug ResponseDocument10 pagesFactors Affecting Inter Individual Variations in Drug Responsehumera50% (4)
- Invoice Example For CompanyDocument6 pagesInvoice Example For CompanyectoclinicNo ratings yet
- CPhI Japan InformationDocument22 pagesCPhI Japan InformationctyvteNo ratings yet
- LearnEnglish Letter ComplaintDocument4 pagesLearnEnglish Letter ComplaintYosef AhmdNo ratings yet
- (Journal) Clinical Pharmacology Therapeutics Journal. Volume 85. Issue 5 (2009) PDFDocument111 pages(Journal) Clinical Pharmacology Therapeutics Journal. Volume 85. Issue 5 (2009) PDFRicovially DavyaNo ratings yet
- Introduction To Drug Utilization ResearchDocument48 pagesIntroduction To Drug Utilization ResearchTummieNo ratings yet
- MR 27 Juli 2021Document21 pagesMR 27 Juli 2021kumoro panjiNo ratings yet
- Journal Titles and AbbreviationsDocument29 pagesJournal Titles and Abbreviationsbalaicar2012No ratings yet
- Guideline On Good Pharmacovigilance Practices (GVP) Module VII - Periodic Safety Update Report (Rev 1)Document68 pagesGuideline On Good Pharmacovigilance Practices (GVP) Module VII - Periodic Safety Update Report (Rev 1)Salló TivadarNo ratings yet
- Cri 192Document5 pagesCri 192Reyn CagmatNo ratings yet
- Organic Chemistry of Natural ProductsDocument29 pagesOrganic Chemistry of Natural ProductsHai-Tung ToNo ratings yet
- NomenclaturafarmacosDocument178 pagesNomenclaturafarmacosAtena Sinahi Romero CervantesNo ratings yet
- Aripiprazole (Generic) ABILIFY (BRAND)Document3 pagesAripiprazole (Generic) ABILIFY (BRAND)missayayaya100% (1)
- Phenobarbital Elixir BP - Electronic Medicines Compendium (eMC) - Print FriendlyDocument5 pagesPhenobarbital Elixir BP - Electronic Medicines Compendium (eMC) - Print FriendlyBrian HarrisNo ratings yet
- Cannabis SativaDocument9 pagesCannabis SativaghitadlamareNo ratings yet
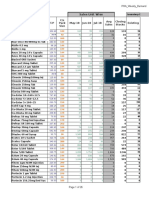
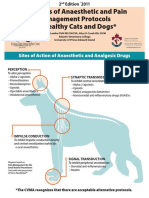
- Examples of Anaesthetic and Pain Management Protocols For Healthy Cats and DogsDocument3 pagesExamples of Anaesthetic and Pain Management Protocols For Healthy Cats and DogsEka FirmanNo ratings yet
- 07 Bibliography FormatDocument14 pages07 Bibliography FormatArjun KafleNo ratings yet
- Week 2 (Revised Sept 2023) Student Non Parenteral MedicationDocument20 pagesWeek 2 (Revised Sept 2023) Student Non Parenteral MedicationsaemhatdsbNo ratings yet
- Evaluation of Paracetamol TabletsDocument12 pagesEvaluation of Paracetamol TabletsYeong Jane LynNo ratings yet
- Match Words 1 - 10 To The Pictures A - J!Document5 pagesMatch Words 1 - 10 To The Pictures A - J!Wendi WahyudiNo ratings yet
- Drug StudyDocument8 pagesDrug StudyJade R. GoNo ratings yet