You might also like
- Intracranial HemorrhageDocument41 pagesIntracranial Hemorrhagedoctormussieaberra100% (1)
- Hypertension PathoDocument2 pagesHypertension Pathojake90210100% (1)
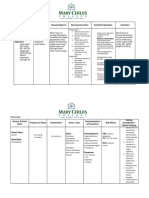
- Assessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationDocument10 pagesAssessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationJobelle AcenaNo ratings yet
- Nursing Care Plan Renal FailureDocument18 pagesNursing Care Plan Renal FailureKundan KumarNo ratings yet
- CHF Cardiomegaly Volume OverloadDocument1 pageCHF Cardiomegaly Volume Overloadnursing concept mapsNo ratings yet
- Novilyn C. Pataray BSN - Ii Hemophilia: St. Paul College of Ilocos SurDocument1 pageNovilyn C. Pataray BSN - Ii Hemophilia: St. Paul College of Ilocos SurCharina AubreyNo ratings yet
- Generic Name & Brand Name Mechanism of Action Indications and Drug Rationale Contraindications Common Side Effects Nursing ConsiderationsDocument2 pagesGeneric Name & Brand Name Mechanism of Action Indications and Drug Rationale Contraindications Common Side Effects Nursing ConsiderationsMary Shine GonidaNo ratings yet
- Healthcare - Nursing Care Plan - Excess Fluid VolumeDocument4 pagesHealthcare - Nursing Care Plan - Excess Fluid VolumeBenjamin CañalitaNo ratings yet
- Concept Map Pleural EffusionDocument1 pageConcept Map Pleural Effusionapi-341263362No ratings yet
- Drug StudyDocument5 pagesDrug StudyDick Morgan FerrerNo ratings yet
- Drug Study Augmentin-KidapawanDocument2 pagesDrug Study Augmentin-KidapawanCherubim Lei DC FloresNo ratings yet
- Drug Study (Calcium Gluconate)Document2 pagesDrug Study (Calcium Gluconate)Andrea Albester GarinoNo ratings yet
- Small Bowel Obstruction Concept MapDocument1 pageSmall Bowel Obstruction Concept MapTessa Claire JaranowskiNo ratings yet
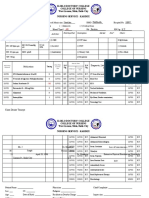
- Iloilo Doctors' College College of Nursing West Avenue, Molo, Iloilo City Nursing Service - KardexDocument4 pagesIloilo Doctors' College College of Nursing West Avenue, Molo, Iloilo City Nursing Service - KardexKiara Denise TamayoNo ratings yet
- Nursing Care Plan. HypertensionDocument2 pagesNursing Care Plan. HypertensionKiara Shanelle Posadas AbrioNo ratings yet
- Angina Pectoris PathophysiologyDocument2 pagesAngina Pectoris PathophysiologyALIANA KIMBERLY MALQUESTONo ratings yet
- Ards Concept MapDocument1 pageArds Concept Mapchristine louise bernardo100% (1)
- Impaired Gas ExchangeDocument1 pageImpaired Gas Exchangeruggero07No ratings yet
- Nursing Care Plan Impaired Gas ExchangeDocument1 pageNursing Care Plan Impaired Gas ExchangeKarylle PetilNo ratings yet
- Student Nurses' Community: NURSING CARE PLAN Functional Urinary IncontinenceDocument4 pagesStudent Nurses' Community: NURSING CARE PLAN Functional Urinary IncontinenceJez RarangNo ratings yet
- Case CHFDocument10 pagesCase CHFAgnes Erlita Distriani Patade50% (2)
- NCP Fluid Vol Excess AgnDocument3 pagesNCP Fluid Vol Excess AgnArbie JacintoNo ratings yet
- Nursing Care Plan: Subjective DataDocument4 pagesNursing Care Plan: Subjective DataAbdallah AlasalNo ratings yet
- Care Plan For Excess Fluid Volume ExampleDocument3 pagesCare Plan For Excess Fluid Volume ExampleVette Angelikka Dela CruzNo ratings yet
- Concept Map Finished 2Document6 pagesConcept Map Finished 2api-352785497100% (1)
- HyperparathyroidismDocument16 pagesHyperparathyroidismkint manlangitNo ratings yet
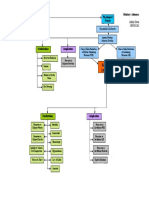
- B. Create Your Concept Map of The Disorder. Use A Separate Paper For This. Use Short Coupon Bond and Draw Your Concept Map Using This FormatDocument5 pagesB. Create Your Concept Map of The Disorder. Use A Separate Paper For This. Use Short Coupon Bond and Draw Your Concept Map Using This FormatPatricia Jean FaeldoneaNo ratings yet
- Cues Nursing Diagnosis Analysis Goals & Objectives Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Analysis Goals & Objectives Intervention Rationale EvaluationMiggy SikatNo ratings yet
- Vitamin KDocument2 pagesVitamin KMuvs RazonNo ratings yet
- Clinical Log Term II PDFDocument9 pagesClinical Log Term II PDFPriscilla S100% (1)
- Drug StudyDocument17 pagesDrug StudyTherese ArellanoNo ratings yet
- Case Study Final PortraitDocument11 pagesCase Study Final PortraitZhy CaluzaNo ratings yet
- NCC-SickleCellAnemiaManagement ConceptMap InteractivePDFDocument2 pagesNCC-SickleCellAnemiaManagement ConceptMap InteractivePDFLoggerz Arck100% (1)
- NCP DM and HCVDDocument3 pagesNCP DM and HCVDMAYBELINE OBAOB100% (1)
- Hypertension Concept MapDocument3 pagesHypertension Concept Map'SheenMarkReal'No ratings yet
- Case Study RespiDocument3 pagesCase Study RespiMark Jheran AlvarezNo ratings yet
- ACS PathophysiologyDocument2 pagesACS PathophysiologyFerliza OblenaNo ratings yet
- Subjective: "Sumikip Ang Dibdib Ko at Hindi Ako Makahinga NG Maayos" As IndependentDocument2 pagesSubjective: "Sumikip Ang Dibdib Ko at Hindi Ako Makahinga NG Maayos" As IndependentCorinneNo ratings yet
- NCP - Activity Intolerance & Excess Fluid VolumeDocument2 pagesNCP - Activity Intolerance & Excess Fluid VolumeCindy MariscotesNo ratings yet
- Nursing Care Plan Date Assessed: December 11, 2017 Nursing Diagnosis Nursing Objective Nursing Intervention Scientific Explanation EvaluationDocument2 pagesNursing Care Plan Date Assessed: December 11, 2017 Nursing Diagnosis Nursing Objective Nursing Intervention Scientific Explanation EvaluationCelyn Nicole Fernandez RollanNo ratings yet
- Health Management of The Patient With Diabetes Mellitus Type 2Document1 pageHealth Management of The Patient With Diabetes Mellitus Type 2Sev Kuzmenko0% (1)
- Propranolol 1 PresentationDocument17 pagesPropranolol 1 Presentationapi-284092317100% (1)
- Risk For Falls Aeb Loss of BalanceDocument4 pagesRisk For Falls Aeb Loss of BalanceAlexandrea MayNo ratings yet
- Renal Failure NCPDocument3 pagesRenal Failure NCPjsksNo ratings yet
- Decrease Cardiac OutputDocument6 pagesDecrease Cardiac OutputGerardeanne ReposarNo ratings yet
- Hemophilia N C P BY BHERU LALDocument1 pageHemophilia N C P BY BHERU LALBheru LalNo ratings yet
- Urinary EliminationDocument5 pagesUrinary EliminationClarence ViboraNo ratings yet
- NCP MRMDocument2 pagesNCP MRMKhloe Cristel Llanes Torres100% (1)
- Drugs - Icu (Group)Document7 pagesDrugs - Icu (Group)Patricia LuceroNo ratings yet
- Caso Clinico Electivas 3Document9 pagesCaso Clinico Electivas 3MARIANGEL LAFONTNo ratings yet
- Nursing AssessmentDocument4 pagesNursing AssessmentFlor SabaysabayNo ratings yet
- Presented by Asmaa Abdelhameed AhmedDocument24 pagesPresented by Asmaa Abdelhameed AhmedSoma Al-mutairiNo ratings yet
- Concept Map 3 MM (Abdominal Pain)Document2 pagesConcept Map 3 MM (Abdominal Pain)Matt McKinleyNo ratings yet
- Drug Study GuideDocument2 pagesDrug Study GuideAubrey Sunga100% (1)
- Case Study Heart Attack PDFDocument30 pagesCase Study Heart Attack PDFtkgoon634950% (2)
- Nursing Care Plan: Fluid Volume Deficit R/T Active Fluid Loss (Increased Urine Output)Document9 pagesNursing Care Plan: Fluid Volume Deficit R/T Active Fluid Loss (Increased Urine Output)Gayu Patel0% (1)
- Disorders of Sodium: Presenter: DR Bharath Kumar P Moderator: DR Ramesh K NDocument41 pagesDisorders of Sodium: Presenter: DR Bharath Kumar P Moderator: DR Ramesh K NBharath Kumar PamulapatiNo ratings yet
- De Methaq L2 HyponatreamiaDocument11 pagesDe Methaq L2 Hyponatreamiaزين العابدين محمد عويش مشريNo ratings yet
- Concept Map TemplateDocument1 pageConcept Map Templatenursing concept mapsNo ratings yet
- Diagnostics: Disorder & Basic Patho/Etiology: Clinical ManifestationsDocument1 pageDiagnostics: Disorder & Basic Patho/Etiology: Clinical Manifestationsnursing concept mapsNo ratings yet
- Bronchial Asthma in Acute Exacerbation BAIAE Pathophysiology Schematic DiagramDocument3 pagesBronchial Asthma in Acute Exacerbation BAIAE Pathophysiology Schematic DiagramVictor Angelo VeraNo ratings yet
- Pathophysiology EmphysemaDocument1 pagePathophysiology EmphysemaGil AswiguiNo ratings yet
- Bipolar Concept MapDocument3 pagesBipolar Concept Mapnursing concept maps100% (2)
- Concept Map BlankDocument2 pagesConcept Map Blanknursing concept mapsNo ratings yet
- Mental Health Concept MapDocument2 pagesMental Health Concept Mapnursing concept mapsNo ratings yet
- ESRD PathophysiologyDocument2 pagesESRD Pathophysiologynursing concept mapsNo ratings yet
- PathoPhysiology of Renal Failure OverviewDocument7 pagesPathoPhysiology of Renal Failure Overviewnursing concept maps100% (1)
- Physiological ChangesDocument1 pagePhysiological ChangesJilian McGuganNo ratings yet
- Concept MapDocument1 pageConcept Mapnursing concept mapsNo ratings yet
- Hip FractureDocument3 pagesHip Fracturenursing concept mapsNo ratings yet
- Diabetes Mellitus Type 2 Schematic DiagramDocument1 pageDiabetes Mellitus Type 2 Schematic DiagramJhe Lyn82% (11)
- Pituitary Adenoma Concept MapDocument1 pagePituitary Adenoma Concept Mapnursing concept mapsNo ratings yet
- Sleep Apnea Concept MapDocument1 pageSleep Apnea Concept Mapashleydean100% (2)
- Degenerative Disc Disease Concept MapDocument1 pageDegenerative Disc Disease Concept Mapnursing concept mapsNo ratings yet
- ARF PathophysiologyDocument2 pagesARF Pathophysiologykathy100% (9)
- Critical Care Concept MapDocument1 pageCritical Care Concept Mapkonniep69100% (1)
- Bipolar Disorder Concept MapDocument1 pageBipolar Disorder Concept Mapnursing concept maps100% (1)
- Infertility Concept MapDocument1 pageInfertility Concept Mapnursing concept maps50% (2)
- Age Greater Than 60 Y/o Hereditary Precipitating Factors: Hypertension Increase Protein and Fat IntakeDocument3 pagesAge Greater Than 60 Y/o Hereditary Precipitating Factors: Hypertension Increase Protein and Fat Intakenursing concept mapsNo ratings yet
- Nursing Management Concept MapDocument1 pageNursing Management Concept MapXy-Za Roy Marie100% (1)
- Hypertension Concept MapDocument1 pageHypertension Concept Mapnursing concept maps100% (1)
- Coronary Artery Bypass Graph Concept MapDocument5 pagesCoronary Artery Bypass Graph Concept Mapnursing concept maps100% (1)
- Osteoarthritis Concept MapDocument1 pageOsteoarthritis Concept Mapnursing concept maps0% (1)
- Cholecystitis Concept MapDocument4 pagesCholecystitis Concept Mapnursing concept maps100% (7)
- Reason For Needing Health Care: Key Problem / ND: Noncompliance Key Problem / NDDocument6 pagesReason For Needing Health Care: Key Problem / ND: Noncompliance Key Problem / NDnursing concept mapsNo ratings yet
- Fluids and Electrolytes IV FluidsDocument1 pageFluids and Electrolytes IV Fluidsnursing concept mapsNo ratings yet
- Schizophrenia Mood Disorders Grief Loss MENTAL HEALTH NURSING PDFDocument19 pagesSchizophrenia Mood Disorders Grief Loss MENTAL HEALTH NURSING PDFnursing concept mapsNo ratings yet
- Chronic Bronchitis and EmphesemaDocument2 pagesChronic Bronchitis and Emphesemanursing concept maps100% (2)
- Spanish Web PDFDocument36 pagesSpanish Web PDFSergio SayagoNo ratings yet
- "The Grace Period Has Ended": An Approach To Operationalize GDPR RequirementsDocument11 pages"The Grace Period Has Ended": An Approach To Operationalize GDPR RequirementsDriff SedikNo ratings yet
- Approaching Checklist Final PDFDocument15 pagesApproaching Checklist Final PDFCohort Partnerships100% (1)
- Ms5 Stress 1Document26 pagesMs5 Stress 1NicolasNo ratings yet
- The "Write" Way: A Judicial Clerk's Guide To Writing For The CourtDocument92 pagesThe "Write" Way: A Judicial Clerk's Guide To Writing For The Courtunknown07blackstarNo ratings yet
- InTech-Project Costs and Risks Estimation Regarding Quality Management System ImplementationDocument28 pagesInTech-Project Costs and Risks Estimation Regarding Quality Management System ImplementationMohamed ArzathNo ratings yet
- Chapter02 AnglesDocument40 pagesChapter02 Angleslen16328100% (1)
- Slides - Simple Linear RegressionDocument35 pagesSlides - Simple Linear RegressionJarir AhmedNo ratings yet
- Oc ch17Document34 pagesOc ch17xavier8491No ratings yet
- Brenda Alderman v. The Philadelphia Housing Authority, 496 F.2d 164, 3rd Cir. (1974)Document16 pagesBrenda Alderman v. The Philadelphia Housing Authority, 496 F.2d 164, 3rd Cir. (1974)Scribd Government DocsNo ratings yet
- SDS SheetDocument8 pagesSDS SheetΠΑΝΑΓΙΩΤΗΣΠΑΝΑΓΟΣNo ratings yet
- Introduction To Financial Management: Topic 1Document85 pagesIntroduction To Financial Management: Topic 1靳雪娇No ratings yet
- CMAR Vs DBBDocument3 pagesCMAR Vs DBBIbrahim BashaNo ratings yet
- A Vagabond SongDocument4 pagesA Vagabond SongLiLiana DewiNo ratings yet
- Concept Paper For Business ResearchDocument4 pagesConcept Paper For Business ResearchRobertchristian RagaNo ratings yet
- Who Di 31-4 Atc-DddDocument6 pagesWho Di 31-4 Atc-DddHenderika Lado MauNo ratings yet
- Muzakarah Jawatankuasa Fatwa Majlis Kebangsaan Bagi Hal Ehwal Ugama Islam Malaysia Kali KeDocument7 pagesMuzakarah Jawatankuasa Fatwa Majlis Kebangsaan Bagi Hal Ehwal Ugama Islam Malaysia Kali KeSiti Zubaidah ZulkhairieNo ratings yet
- Autoregressive-Moving Average (ARMA) ModelsDocument34 pagesAutoregressive-Moving Average (ARMA) Modelsflaviorochaavila100% (1)
- Heat Transfer OperationsDocument10 pagesHeat Transfer OperationsShafique AhmedNo ratings yet
- Jurnal Q1 PDFDocument29 pagesJurnal Q1 PDFSepti DamayantiNo ratings yet
- The Example of Text That Contains Present Perfect TenseDocument2 pagesThe Example of Text That Contains Present Perfect TenseRahmiSyariif100% (1)
- Unit 9:: What Did You See at The Zoo?Document11 pagesUnit 9:: What Did You See at The Zoo?ARiFin MoHaMedNo ratings yet
- Elitmus PapersDocument21 pagesElitmus Papersanon_879320987No ratings yet
- ESSAYDocument1 pageESSAYJunalie GregoreNo ratings yet
- Vocabulary ListDocument2 pagesVocabulary List謝明浩No ratings yet
- Myriam Met. CBLDocument25 pagesMyriam Met. CBLCamila EscobarNo ratings yet
- Ujt and PutDocument35 pagesUjt and Putisraeljumbo100% (1)
- Coursera Qs-Ans For Financial AidDocument2 pagesCoursera Qs-Ans For Financial AidMarno03No ratings yet
- 2007 - Q1 NewsletterDocument20 pages2007 - Q1 NewsletterKisara YatiyawelaNo ratings yet
- DaybreaksDocument14 pagesDaybreaksKYLE FRANCIS EVANo ratings yet