You might also like
- Baptism EventDocument37 pagesBaptism Eventsharmaine ella guittap68% (19)
- Sleep ApneaDocument23 pagesSleep Apneahams100% (1)
- Acupuncture Treatment For Sleep ApneaDocument11 pagesAcupuncture Treatment For Sleep Apneataoacu2000100% (1)
- TMJ Ankylosis Case PresentationDocument60 pagesTMJ Ankylosis Case PresentationbasharakmNo ratings yet
- Sleep Apnea JournalDocument4 pagesSleep Apnea JournalShamini ShanmugalingamNo ratings yet
- Obstructive Sleep Apnoea Sept 2014Document4 pagesObstructive Sleep Apnoea Sept 2014Desak PratiwiNo ratings yet
- Information Supplement: Obstructive Sleep ApnoeaDocument4 pagesInformation Supplement: Obstructive Sleep ApnoeaNgaire TaylorNo ratings yet
- Sleep Medicine: Devi Farida UtamiDocument105 pagesSleep Medicine: Devi Farida UtamimufiNo ratings yet
- ResearchDocument3 pagesResearchapi-380517264No ratings yet
- Patient Information Brochure: What Is Obstructive Sleep Apnea?Document2 pagesPatient Information Brochure: What Is Obstructive Sleep Apnea?Muhammad SyammNo ratings yet
- Name: Ericka Vanessa MoránDocument6 pagesName: Ericka Vanessa MoránLitopez YepezNo ratings yet
- Sleep Disorders (Diasomnia) : Diasomnia - Difficulties Falling Asleep or WakingDocument11 pagesSleep Disorders (Diasomnia) : Diasomnia - Difficulties Falling Asleep or Wakingfunny-arianNo ratings yet
- The Facts On Sleep Apnea SecretsDocument63 pagesThe Facts On Sleep Apnea SecretsClariceikoNo ratings yet
- Sleep Apnoea - Prof - DR K.K.PDocument44 pagesSleep Apnoea - Prof - DR K.K.PjialeongNo ratings yet
- Obstructive Sleep Apnea SyndromeDocument44 pagesObstructive Sleep Apnea SyndromeSantiNo ratings yet
- Sleep Apnea - Could It Be Robbing You of Rest?Document4 pagesSleep Apnea - Could It Be Robbing You of Rest?Saya MenangNo ratings yet
- Sleep ApnoeaDocument2 pagesSleep Apnoeaapi-338840258No ratings yet
- Obstructive Sleep Apnoea SyndromeDocument72 pagesObstructive Sleep Apnoea SyndromeArjun SainiNo ratings yet
- Obstructive Sleep Apnea and Analgesia - SJH PowerpointDocument29 pagesObstructive Sleep Apnea and Analgesia - SJH PowerpointAbd ZouhierNo ratings yet
- Case Study 20Document5 pagesCase Study 20yjones39100% (3)
- Sleep Apnea: Name - Bharvi Yadav Roll No. - 200BSCCP015Document8 pagesSleep Apnea: Name - Bharvi Yadav Roll No. - 200BSCCP015Bharvi YadavNo ratings yet
- Sleep Apnea Syndrome &Document28 pagesSleep Apnea Syndrome &Sumit PuloriaNo ratings yet
- Management of Obstructive Sleep Apnea: A Dental Perspective: Eview RticleDocument9 pagesManagement of Obstructive Sleep Apnea: A Dental Perspective: Eview RticleFourthMolar.comNo ratings yet
- Obstructive Sleep Apnea in AdultsDocument2 pagesObstructive Sleep Apnea in AdultsElaine CristinaNo ratings yet
- Nasal Obstruction and Obstruction During Sleep - Pausanos and GoDocument10 pagesNasal Obstruction and Obstruction During Sleep - Pausanos and GoPowell TabogocNo ratings yet
- Obstructive Sleep ApnoeaDocument69 pagesObstructive Sleep ApnoeaPrasanna Datta100% (1)
- OSCE Sleep ApneaDocument2 pagesOSCE Sleep ApneaNadia AlmahalawiNo ratings yet
- Obstructive Sleep ApneaDocument15 pagesObstructive Sleep ApneaMushee01No ratings yet
- SnoringDocument12 pagesSnoringa3llamNo ratings yet
- Adenoids and TonsilsDocument12 pagesAdenoids and TonsilsUsama FadhulNo ratings yet
- Sleep Disordered Breathing (Part 4) : Obstructive Sleep Apnea in ChildrenDocument5 pagesSleep Disordered Breathing (Part 4) : Obstructive Sleep Apnea in ChildrenSuprit SnNo ratings yet
- Sleep Disordered Breathing/ Obstructive Sleep Apnea: Jhansi Nalamati MDDocument53 pagesSleep Disordered Breathing/ Obstructive Sleep Apnea: Jhansi Nalamati MDRabie MeramNo ratings yet
- Leep Pnea: Reporters: Desdechado, Niellan Ferrer, Jessa Magkilat, Hanzarri Palmes, Kamillah Sabat, ChristianDocument27 pagesLeep Pnea: Reporters: Desdechado, Niellan Ferrer, Jessa Magkilat, Hanzarri Palmes, Kamillah Sabat, ChristianEira LopezNo ratings yet
- Sleep Apnea Term PaperDocument8 pagesSleep Apnea Term Paperf1gisofykyt3100% (1)
- 152 Obstructive Sleep Apnoea and Anaesthesia 1Document6 pages152 Obstructive Sleep Apnoea and Anaesthesia 1Echo WahyudiNo ratings yet
- Cure Sleep ApneaDocument5 pagesCure Sleep ApneaAdelyn Bebz AchiengNo ratings yet
- Sleep Apnea and Sleep-Disordered BreathingDocument64 pagesSleep Apnea and Sleep-Disordered Breathing李丞永No ratings yet
- Snoring, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandSnoring, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Obstructive Sleep Apnea - Dr.M.M.varadharaja / Orthodontic Courses by Indian Dental AcademyDocument168 pagesObstructive Sleep Apnea - Dr.M.M.varadharaja / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Apnea Obstructiva Del SueñoDocument22 pagesApnea Obstructiva Del SueñoRaul SotoNo ratings yet
- Obstructive Sleep ApnoeaDocument43 pagesObstructive Sleep Apnoeachunshienwc6833100% (3)
- Obstructive Sleep ApneaDocument80 pagesObstructive Sleep ApneaAamir Yousuf100% (2)
- ANESTHESIA For OTLARYNGOLOGIC SurgeryDocument64 pagesANESTHESIA For OTLARYNGOLOGIC SurgeryKelvin TuazonNo ratings yet
- Obesity and Obstructive Sleep ApnoeaDocument26 pagesObesity and Obstructive Sleep ApnoeaMagdi PienaarNo ratings yet
- LaryngitisDocument9 pagesLaryngitisjonna casumpangNo ratings yet
- Adult and Pediatric Obstructive Sleep ApneaDocument44 pagesAdult and Pediatric Obstructive Sleep ApneaSwastik SatpathyNo ratings yet
- PrintDocument65 pagesPrintLý TưởngNo ratings yet
- Sleep ApneuDocument22 pagesSleep ApneuAnonymous 8Jlc7aTs90No ratings yet
- Nclex (1301) (1) (1315)Document43 pagesNclex (1301) (1) (1315)Elizabeth SharmaNo ratings yet
- 2 Respiratory ObstructionDocument8 pages2 Respiratory ObstructionLulu MushiNo ratings yet
- RPS - BLS (Dr. Bindo)Document38 pagesRPS - BLS (Dr. Bindo)Krmilla KumillNo ratings yet
- Cure Sleep Apnea: Everything About Sleep Apnea And Sleep Apnea TreatmentFrom EverandCure Sleep Apnea: Everything About Sleep Apnea And Sleep Apnea TreatmentRating: 3.5 out of 5 stars3.5/5 (3)
- OSA Obstructive Sleep Apnea Fact SheetDocument4 pagesOSA Obstructive Sleep Apnea Fact SheetChoche Luis Jodon100% (1)
- Sleep Disorders Presented by Group 4Document30 pagesSleep Disorders Presented by Group 4Praise ToluwalaseNo ratings yet
- 18sleep Apnea and Sleep DisordersDocument23 pages18sleep Apnea and Sleep Disordersnikita ester100% (1)
- LaryngospasmDocument3 pagesLaryngospasmbalab2311No ratings yet
- Obstructive Sleep Apnea, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandObstructive Sleep Apnea, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 3 out of 5 stars3/5 (2)
- Obstructive Sleep Apnea: SS Visser Lung Unit Pah and UpDocument23 pagesObstructive Sleep Apnea: SS Visser Lung Unit Pah and UpMuhammad NuruddinNo ratings yet
- Sleep Disorders Treatment GuideDocument16 pagesSleep Disorders Treatment GuideNestor BalboaNo ratings yet
- OSA UpdatesDocument64 pagesOSA UpdatesRosmadi IsmailNo ratings yet
- Treating Obstructive Sleep Apnea Improves Essential Hypertension and Quality of LifeDocument8 pagesTreating Obstructive Sleep Apnea Improves Essential Hypertension and Quality of Life'ArifahAhmadNo ratings yet
- Samsung Scholarship Application 2013Document8 pagesSamsung Scholarship Application 2013Alex CarricoNo ratings yet
- Bukh DV 36 SmeDocument5 pagesBukh DV 36 SmeTullio OpattiNo ratings yet
- NCEPOD / CEPOD National Confidential Enquiry Into Post Operative DeathsDocument23 pagesNCEPOD / CEPOD National Confidential Enquiry Into Post Operative DeathsdrschethanNo ratings yet
- Event Report Insights Into HackathonDocument7 pagesEvent Report Insights Into HackathonSujoy SarkarNo ratings yet
- Knit Free by JojiDocument8 pagesKnit Free by JojipaulaNo ratings yet
- Universal Preschool Is No Golden Ticket: Why Government Should Not Enter The Preschool Business, Cato Policy Analysis No. 333Document31 pagesUniversal Preschool Is No Golden Ticket: Why Government Should Not Enter The Preschool Business, Cato Policy Analysis No. 333Cato InstituteNo ratings yet
- AbductedDocument160 pagesAbductedSoni Mishra TiwariNo ratings yet
- Bridge 3 Deck DesignDocument16 pagesBridge 3 Deck DesignMd MamroseNo ratings yet
- Bab 2Document13 pagesBab 2Teguh Novri YansyahNo ratings yet
- PLC Timers and CountersDocument16 pagesPLC Timers and CountersTristan Jeff BautistaNo ratings yet
- NCM 210 RLE - 10 Herbal Plants Approved by DOHDocument6 pagesNCM 210 RLE - 10 Herbal Plants Approved by DOHLYRIZZA LEA BHEA DESIATANo ratings yet
- Trumpet Auditions Spring 2023Document7 pagesTrumpet Auditions Spring 2023JeffNo ratings yet
- MIT 103 Assignment-1Document9 pagesMIT 103 Assignment-1Rachna BhatnagarNo ratings yet
- No Homework Policy Counter ArgumentDocument2 pagesNo Homework Policy Counter ArgumentRafael Silva Medina100% (1)
- Questioner For The Long Quiz (Grade 8)Document3 pagesQuestioner For The Long Quiz (Grade 8)Novie Mae ReambonanzaNo ratings yet
- BGM User ManualDocument48 pagesBGM User ManualAlgebra92No ratings yet
- Verification and Validation in CFD and Heat Transfer: ANSYS Practice and The New ASME StandardDocument22 pagesVerification and Validation in CFD and Heat Transfer: ANSYS Practice and The New ASME StandardMaxim100% (1)
- Ccna Interview Ques-2Document11 pagesCcna Interview Ques-2Sarath Chandra GupthaNo ratings yet
- Nursing Dissertation SmokingDocument8 pagesNursing Dissertation SmokingCustomPapersOnlineSingapore100% (1)
- 6.2.3.7 Packet Tracer - Configuring Multiarea OSPFv3 Instructions IGDocument3 pages6.2.3.7 Packet Tracer - Configuring Multiarea OSPFv3 Instructions IGana100% (1)
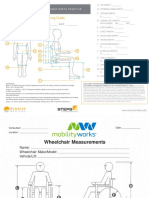
- Attachemnt A - Body and Wheelchair MeasurementDocument2 pagesAttachemnt A - Body and Wheelchair MeasurementNur Adila MokhtarNo ratings yet
- AICTE 360 Degree Feedback Implementation Manual 20210123Document31 pagesAICTE 360 Degree Feedback Implementation Manual 20210123pradeephmkumarNo ratings yet
- Therapist Driven ProtocolsDocument3 pagesTherapist Driven ProtocolsPaoly PalmaNo ratings yet
- Action of Catalase On Hydrogen PeroxideDocument4 pagesAction of Catalase On Hydrogen PeroxideRuchie Ann Pono BaraquilNo ratings yet
- Nanoscience and Nanotechnology in ArgentinaDocument84 pagesNanoscience and Nanotechnology in ArgentinaMaterials Research InstituteNo ratings yet
- MOS Structure Lifting PlanDocument15 pagesMOS Structure Lifting Planmuiqbal.workNo ratings yet
- Grand Case Study V7 Final 030310Document49 pagesGrand Case Study V7 Final 030310Jemimah Ruth Madayag ValenzuelaNo ratings yet
- Big Dams, Development Aid and World BankDocument24 pagesBig Dams, Development Aid and World BankMushtaq GaadiNo ratings yet
- Activity Based CostingDocument26 pagesActivity Based CostingVishal BabuNo ratings yet