You might also like
- Timeline Cardiac Surgery - enDocument10 pagesTimeline Cardiac Surgery - enMaría Félix Ovalle de NavarroNo ratings yet
- Shinmaywa CR PDFDocument8 pagesShinmaywa CR PDFanggera91No ratings yet
- FinlandaDocument76 pagesFinlandaMarius AlexandruNo ratings yet
- Toxoplasma GondiiDocument29 pagesToxoplasma GondiiNagalingaNo ratings yet
- FPD 1361 Ea4Document12 pagesFPD 1361 Ea4Moe LattNo ratings yet
- What Is in Vitro Fertilization (IVF) and Its ProcessDocument4 pagesWhat Is in Vitro Fertilization (IVF) and Its ProcessPlanet womenNo ratings yet
- Workbook For Designing, Implementing, and Evaluating A Sharps Injury Prevention ProgramDocument168 pagesWorkbook For Designing, Implementing, and Evaluating A Sharps Injury Prevention ProgramBheki TshimedziNo ratings yet
- Horn SystemsDocument4 pagesHorn SystemsArt DoeNo ratings yet
- Sludge Pump - WASTE WATER1 PDFDocument6 pagesSludge Pump - WASTE WATER1 PDFAvijitSinharoyNo ratings yet
- Lawrence Pumps VPL3600: Vertical Lineshaft, Slurry PumpDocument8 pagesLawrence Pumps VPL3600: Vertical Lineshaft, Slurry PumpjnNo ratings yet
- Baby Vaccination ChartDocument2 pagesBaby Vaccination Chartsujit21inNo ratings yet
- Materials Management: Interview Questions & AnswersDocument114 pagesMaterials Management: Interview Questions & AnswersAnirban BaralNo ratings yet
- Pumps Motors and Diesel Engine - Compliance by Wilo PDFDocument6 pagesPumps Motors and Diesel Engine - Compliance by Wilo PDFDurgawati MishraNo ratings yet
- Chapter 5 Application of Insulating MaterialDocument21 pagesChapter 5 Application of Insulating MaterialAmir nawazNo ratings yet
- MUST To KNOW in Blood Banking 1Document19 pagesMUST To KNOW in Blood Banking 1Aya Virtucio100% (1)
- Management of Third and Fourth Degree TearsDocument4 pagesManagement of Third and Fourth Degree TearsYwagar YwagarNo ratings yet
- Pathophysiology of CHOLELITHIASISDocument2 pagesPathophysiology of CHOLELITHIASISLiza Marie Cayetano Adarne57% (7)
- Pathophysiology of CHOLELITHIASISDocument2 pagesPathophysiology of CHOLELITHIASISLiza Marie Cayetano Adarne57% (7)
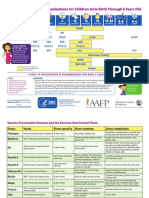
- Parent Ver SCH 0 6yrs AafpDocument2 pagesParent Ver SCH 0 6yrs AafpcicitNo ratings yet
- Human Anatomy RespiratoryDocument36 pagesHuman Anatomy RespiratoryHafid JuniorNo ratings yet
- HMIS 322 Final ExamDocument10 pagesHMIS 322 Final Examkalasa royd100% (2)
- Summary of Key Points: Tetanus Vaccines: WHO Position Paper - February 2017Document19 pagesSummary of Key Points: Tetanus Vaccines: WHO Position Paper - February 2017rendha sasongkoNo ratings yet
- Tour PlanDocument31 pagesTour Planrah98No ratings yet
- History of CancerDocument17 pagesHistory of CancercheaussieNo ratings yet
- Top 52 Structural Engineer Interview Questions With Answers: Free EbookDocument77 pagesTop 52 Structural Engineer Interview Questions With Answers: Free Ebooknaga lakshmiNo ratings yet
- Anatomy and Physiology of Respiratory SystemDocument9 pagesAnatomy and Physiology of Respiratory SystemLiza Marie Cayetano AdarneNo ratings yet
- Nebulization TherapyDocument24 pagesNebulization TherapyMark Francis S. RajasNo ratings yet
- Expanded Program ImmunizationDocument4 pagesExpanded Program ImmunizationLheiDanielMariellMonteroNo ratings yet
- NCP Impaired Skin IntegrityDocument2 pagesNCP Impaired Skin IntegrityLiza Marie Cayetano Adarne93% (14)
- What Is CancerDocument126 pagesWhat Is Cancernodyrose2000100% (2)
- RH Incompatibility: Go ToDocument4 pagesRH Incompatibility: Go ToFadhila AnasNo ratings yet
- A Report On Raising of BroilersDocument9 pagesA Report On Raising of BroilersBabu Ram Panthi69% (13)
- ItalyTourItinerary 03Document6 pagesItalyTourItinerary 03Inge VkoNo ratings yet
- Oncology: Origin of The Word CancerDocument18 pagesOncology: Origin of The Word CancerShahab SaqibNo ratings yet
- NCP Ineffective Tissue PerfusionDocument2 pagesNCP Ineffective Tissue PerfusionLiza Marie Cayetano Adarne71% (17)
- l8 Management of Perianal Pain and ConditionsDocument51 pagesl8 Management of Perianal Pain and ConditionsMohd Johari Mohd ShafuwanNo ratings yet
- When Not To Do IVFDocument19 pagesWhen Not To Do IVFAnoushka PalNo ratings yet
- Intractable, Refractory Cough - Jindal IVF ChandigarhDocument9 pagesIntractable, Refractory Cough - Jindal IVF ChandigarhJindal Chest ClinicNo ratings yet
- IuiDocument34 pagesIuiDenis100% (1)
- Cheapofareus-Tips To Book Cheap FlightDocument4 pagesCheapofareus-Tips To Book Cheap FlightcheapofareusNo ratings yet
- Rensa FittingsDocument9 pagesRensa Fittingsjpsingh75No ratings yet
- VLOOKUP and Hlookup FunctionsDocument13 pagesVLOOKUP and Hlookup FunctionsVaibhav DwivediNo ratings yet
- Final Prenatal Fact SheetDocument3 pagesFinal Prenatal Fact Sheetapi-469724337No ratings yet
- Boletin Non ClogDocument12 pagesBoletin Non ClogulisesgeNo ratings yet
- Diabetes and You: Your Guide To Better Living With DiabetesDocument51 pagesDiabetes and You: Your Guide To Better Living With DiabetesdrjperumalNo ratings yet
- Health Benifits of FishDocument10 pagesHealth Benifits of Fishsrinivasnfdb7291No ratings yet
- Arthritis Joint Pain ReliefDocument14 pagesArthritis Joint Pain ReliefSam CookNo ratings yet
- TGM Metallurgy 010910 NK PDFDocument335 pagesTGM Metallurgy 010910 NK PDFSiti Rabiatul AdawiyahNo ratings yet
- ? Excel VLOOKUP - Massive Guide With 8 ExamplesDocument19 pages? Excel VLOOKUP - Massive Guide With 8 Examplessunil unnithanNo ratings yet
- RUH Umpen: Ruhrpumpen GMBHDocument40 pagesRUH Umpen: Ruhrpumpen GMBHjacobo nasimbaNo ratings yet
- Best 61 Travel TipsDocument12 pagesBest 61 Travel TipsKaran Arora ChandigarhNo ratings yet
- H and P Unit I II III MQCDocument36 pagesH and P Unit I II III MQCSuryakant LadNo ratings yet
- 4 H Surgical Instruments and TerminologyDocument17 pages4 H Surgical Instruments and TerminologyMahmoud Hussien100% (1)
- Rheumatoid ArthritisDocument38 pagesRheumatoid ArthritisOlga GoryachevaNo ratings yet
- Diseases of The Respiratory SystemDocument44 pagesDiseases of The Respiratory SystemEugenia Ceban100% (2)
- TGM - Synthetic Organic Chemicals - 010910 - NK PDFDocument290 pagesTGM - Synthetic Organic Chemicals - 010910 - NK PDFsanthoshneo02@gmail.comNo ratings yet
- Fully Disposable Auto Injector For Drugs in VialsDocument2 pagesFully Disposable Auto Injector For Drugs in VialsIsrael ExporterNo ratings yet
- CancerDocument60 pagesCancerAnonymous JCUVTVoNo ratings yet
- ENTOMOLOGYDocument3 pagesENTOMOLOGYMayowa OgunmolaNo ratings yet
- The History of CancerDocument34 pagesThe History of CancerGermánNo ratings yet
- Skin CancerDocument26 pagesSkin CancerSrinivasa Rao ChintapatlaNo ratings yet
- The History of CancerDocument35 pagesThe History of CancerAnjum RizviNo ratings yet
- 16 1 Stone PDFDocument29 pages16 1 Stone PDFVel MuruganNo ratings yet
- An Insight Into Cancer and Anticancer Drugs: Acta Scientific Medical Sciences (Issn: 2582-0931)Document12 pagesAn Insight Into Cancer and Anticancer Drugs: Acta Scientific Medical Sciences (Issn: 2582-0931)Awais Arain AhmadNo ratings yet
- Disease ReportDocument9 pagesDisease ReportDamir WhiteNo ratings yet
- Speaker:: University of Birmingham - 2 - 3 - What - Is - Cancer - HD - 1080pDocument2 pagesSpeaker:: University of Birmingham - 2 - 3 - What - Is - Cancer - HD - 1080pdrmadankumarbnysNo ratings yet
- The History of Cancer Research: Introducing An AACR Centennial SeriesDocument2 pagesThe History of Cancer Research: Introducing An AACR Centennial SeriesNiswatul InayahNo ratings yet
- History of OncologyDocument2 pagesHistory of OncologyMilagros GarcíaNo ratings yet
- NIH Public Access: Author ManuscriptDocument7 pagesNIH Public Access: Author ManuscriptAnaNo ratings yet
- The Evolution of Mastectomy Surgical Technique - From Mutilation To MedicineDocument8 pagesThe Evolution of Mastectomy Surgical Technique - From Mutilation To MedicineAnonymous LnWIBo1GNo ratings yet
- Ijc 29134Document15 pagesIjc 29134AnaNo ratings yet
- NCP N.D.Document3 pagesNCP N.D.Liza Marie Cayetano AdarneNo ratings yet
- Articiafical Airways Mechanical Ventilator - MachineDocument1 pageArticiafical Airways Mechanical Ventilator - MachineLiza Marie Cayetano AdarneNo ratings yet
- Breast CancerDocument2 pagesBreast CancerLiza Marie Cayetano AdarneNo ratings yet
- Cover and Table of ContentsDocument4 pagesCover and Table of ContentsLiza Marie Cayetano AdarneNo ratings yet
- Reflection Paper On Cases 3 and 4Document1 pageReflection Paper On Cases 3 and 4Liza Marie Cayetano AdarneNo ratings yet
- Acknowledgement and AbstractDocument2 pagesAcknowledgement and AbstractLiza Marie Cayetano AdarneNo ratings yet
- Rev - PROPOSAL Template June 2011 For MIX METHODS Quali & Quanti RESEARCH CorrectedDocument17 pagesRev - PROPOSAL Template June 2011 For MIX METHODS Quali & Quanti RESEARCH CorrectedLiza Marie Cayetano AdarneNo ratings yet
- Letter of AssentDocument2 pagesLetter of AssentLiza Marie Cayetano AdarneNo ratings yet
- Review of SystemsDocument3 pagesReview of SystemsLiza Marie Cayetano AdarneNo ratings yet
- Online Teaching Strategies To Improve Collaboration Among Nursing StudentsDocument8 pagesOnline Teaching Strategies To Improve Collaboration Among Nursing StudentsLiza Marie Cayetano AdarneNo ratings yet
- Definitions of Branches of FeminisnDocument3 pagesDefinitions of Branches of FeminisnJennilyn TugelidaNo ratings yet
- AnalysisDocument9 pagesAnalysisLiza Marie Cayetano AdarneNo ratings yet
- Junichiro Tanizaki TheTattooerDocument9 pagesJunichiro Tanizaki TheTattooerLiza Marie Cayetano AdarneNo ratings yet
- Viral CarcinogenesisDocument18 pagesViral CarcinogenesisTowardsLightNo ratings yet
- Asepsis - MedicalDocument6 pagesAsepsis - MedicalChetan KumarNo ratings yet
- Infection Controle Nursing ManagementDocument22 pagesInfection Controle Nursing ManagementUday KumarNo ratings yet
- Reflection On Biorisk ManagementDocument2 pagesReflection On Biorisk ManagementqueenNo ratings yet
- April 30, 2021 Strathmore TimesDocument16 pagesApril 30, 2021 Strathmore TimesStrathmore TimesNo ratings yet
- Daily Express-23Apr 2Document43 pagesDaily Express-23Apr 2vnaliniNo ratings yet
- Immunoglobulins: Structure and Function Immunoglobulins (Ig) - Glycoprotein Molecules Which Are Produced by Plasma Cells inDocument14 pagesImmunoglobulins: Structure and Function Immunoglobulins (Ig) - Glycoprotein Molecules Which Are Produced by Plasma Cells inCristina GeorgianaNo ratings yet
- Bacterial Histidine Kinases As Novel Antibacterial Drug TargetsDocument12 pagesBacterial Histidine Kinases As Novel Antibacterial Drug TargetsSritapa Basu MallickNo ratings yet
- COVID-19 Cases and Hospitalizations by COVID-19 Vaccination Status and Previous COVID-19 Diagnosis - California and New York, May-November 2021Document7 pagesCOVID-19 Cases and Hospitalizations by COVID-19 Vaccination Status and Previous COVID-19 Diagnosis - California and New York, May-November 2021News10NBCNo ratings yet
- Routine Immunization Schedule ToolDocument2 pagesRoutine Immunization Schedule ToolJack MillerNo ratings yet
- New Variants of CovidDocument2 pagesNew Variants of CovidAdrian Jay BeloyNo ratings yet
- Pakistan Statistical Year Book, 2016Document514 pagesPakistan Statistical Year Book, 2016Eman WahidNo ratings yet
- Nursing AssessmentDocument8 pagesNursing AssessmentDien NingsihbaliNo ratings yet
- WDP PathologyTube Chart and Order of Draw v2 0Document1 pageWDP PathologyTube Chart and Order of Draw v2 0KABAL SINGH GILL100% (1)
- CertificatDocument2 pagesCertificatIulia LupeiNo ratings yet
- MCN Drill 1Document23 pagesMCN Drill 1Cai Velasco DecenaNo ratings yet
- Application Status Granted Visa Conditions: Maritime Crew (Subclass 988)Document4 pagesApplication Status Granted Visa Conditions: Maritime Crew (Subclass 988)ren rosallosaNo ratings yet
- Try Out Un Gunadarma 2018 Paket ADocument17 pagesTry Out Un Gunadarma 2018 Paket ADwinta100% (1)
- 45 Common Veterinary VaccinesDocument26 pages45 Common Veterinary Vaccinesjackpotjonathan0No ratings yet
- "Ebola" The Worst Virus From AfricaDocument3 pages"Ebola" The Worst Virus From AfricaCamilo CanoNo ratings yet
- Vaccine Cold Chain in General Practices: A Prospective Study in 75 Refrigerators (Keep Cool Study)Document13 pagesVaccine Cold Chain in General Practices: A Prospective Study in 75 Refrigerators (Keep Cool Study)Cherry LwinNo ratings yet
- Antivenom - How It's Made and Why It's So PreciousDocument6 pagesAntivenom - How It's Made and Why It's So PreciousnetriderNo ratings yet
- Oak Hill SH PDFDocument29 pagesOak Hill SH PDFLanie MarcosNo ratings yet
- Data CTRI DataDocument5 pagesData CTRI DataDonvgmailNo ratings yet