You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Solution Manual For High Acuity Nursing 7th Edition WagnerDocument25 pagesSolution Manual For High Acuity Nursing 7th Edition WagnerJamesThomasngec97% (35)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- (XXX Echocardiography Facility) : 2-D & M-Mode Echocardiogram Report Color Flow Doppler ReportDocument1 page(XXX Echocardiography Facility) : 2-D & M-Mode Echocardiogram Report Color Flow Doppler ReportArijitArikNath100% (1)
- Edexcel As Biology Revision Guide PDF FreeDocument108 pagesEdexcel As Biology Revision Guide PDF Freebody fayez100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- A Clinician's Guide To Nuclear MedicineDocument409 pagesA Clinician's Guide To Nuclear Medicineayodeji7886% (7)
- Pharmacology Chapter 42 p-2Document11 pagesPharmacology Chapter 42 p-2sho bartNo ratings yet
- LaminectomyDocument6 pagesLaminectomyPerrilyn Perey100% (1)
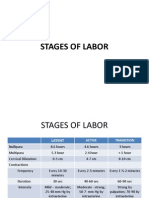
- Stages of LaborDocument30 pagesStages of LaborPerrilyn Perey100% (1)
- Excess Fluid Volume PPT (Case Press)Document10 pagesExcess Fluid Volume PPT (Case Press)Perrilyn PereyNo ratings yet
- Acute Renal FailureDocument4 pagesAcute Renal FailurePerrilyn PereyNo ratings yet
- Bubbles HeDocument39 pagesBubbles HePerrilyn PereyNo ratings yet
- 5 P - S of LaborDocument19 pages5 P - S of LaborPerrilyn PereyNo ratings yet
- Hematologic DiseasesDocument11 pagesHematologic DiseasesPerrilyn Perey100% (2)
- Nihms281140.pdf BibliographyDocument13 pagesNihms281140.pdf BibliographyPerrilyn PereyNo ratings yet
- Arrest of DescentDocument5 pagesArrest of DescentPerrilyn PereyNo ratings yet
- Critcare PDFDocument20 pagesCritcare PDFPerrilyn PereyNo ratings yet
- Leg or Foot Amputation Pref CardDocument2 pagesLeg or Foot Amputation Pref CardPerrilyn PereyNo ratings yet
- Anxiety Related 2010Document17 pagesAnxiety Related 2010Perrilyn PereyNo ratings yet
- Drug NameDocument1 pageDrug NamePerrilyn PereyNo ratings yet
- OR TermsDocument1 pageOR TermsPerrilyn PereyNo ratings yet
- MenstruationDocument1 pageMenstruationPerrilyn PereyNo ratings yet
- Health Assessment Form Scribd.Document1 pageHealth Assessment Form Scribd.Perrilyn PereyNo ratings yet
- HUMAN ANATOMY AND PHYSIOLOGY LABORATORY Cardiovascular SystemDocument12 pagesHUMAN ANATOMY AND PHYSIOLOGY LABORATORY Cardiovascular SystemZaira MangalimanNo ratings yet
- Fisiologi Sistem KardiovaskularDocument28 pagesFisiologi Sistem Kardiovaskularpriesha aprilia03No ratings yet
- Atif Afzal Quick HintsDocument54 pagesAtif Afzal Quick Hintssara khanNo ratings yet
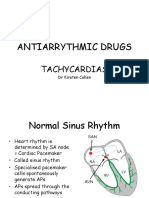
- Antiarrythmic Drugs: TachycardiasDocument36 pagesAntiarrythmic Drugs: TachycardiasDrDeepak PawarNo ratings yet
- Cardiac Cycle: Mechanical Event and Their Electrical and Clinical CorrelationDocument28 pagesCardiac Cycle: Mechanical Event and Their Electrical and Clinical Correlationhawas muhammed100% (1)
- Door To Unload: A New Paradigm For The Management of Cardiogenic ShockDocument8 pagesDoor To Unload: A New Paradigm For The Management of Cardiogenic ShockAttilio Del RossoNo ratings yet
- Animal Science 121 Principles To Animal Science Compiled by Dr. Erwin L. IcallaDocument19 pagesAnimal Science 121 Principles To Animal Science Compiled by Dr. Erwin L. IcallaJamielyne Rizza AtienzaNo ratings yet
- Edexcel Biology A2 2006 June Ms AllDocument88 pagesEdexcel Biology A2 2006 June Ms AllSachitra Wijethunga100% (2)
- Ketogenic Diets Inhibit Mitochondrial Biogenesis and Induce Cardiac FibrosisDocument13 pagesKetogenic Diets Inhibit Mitochondrial Biogenesis and Induce Cardiac FibrosisUriel MoralexNo ratings yet
- Lie Detection TechniquesDocument260 pagesLie Detection Techniquesnavarrodan0823No ratings yet
- Biology Unit 1 Repeat Questions PDFDocument12 pagesBiology Unit 1 Repeat Questions PDFFarah100% (1)
- Biology Notes Form Two: Transport in Plants and AnimalsDocument49 pagesBiology Notes Form Two: Transport in Plants and AnimalsPeter Osundwa Kiteki100% (3)
- The Heart of The MatterDocument33 pagesThe Heart of The MatterhuangsoulNo ratings yet
- Case Presentation On Coronary Artery Disease - 090908Document54 pagesCase Presentation On Coronary Artery Disease - 090908Parth Vasave100% (3)
- Targeted Neonatal Echocardiography Teaching Manual-New EditionDocument80 pagesTargeted Neonatal Echocardiography Teaching Manual-New EditionAbraham Vallejos100% (1)
- Anatomy & Physiology of The Cardiovascular SystemDocument3 pagesAnatomy & Physiology of The Cardiovascular SystemluaNo ratings yet
- Jurnal Pakai 2 (Diagnosis, Tatalaksana) Efusi PerikardiumDocument9 pagesJurnal Pakai 2 (Diagnosis, Tatalaksana) Efusi PerikardiumSatrya DitaNo ratings yet
- Jugular Venous Pulse: Madras Medical MissionDocument53 pagesJugular Venous Pulse: Madras Medical MissionJoshua JayakaranNo ratings yet
- Hemodynamic Monitoring Riding The Waves in California Renee SmithDocument30 pagesHemodynamic Monitoring Riding The Waves in California Renee SmithSanaz NikiNo ratings yet
- Buret TerbaruDocument33 pagesBuret TerbaruEka Rahayu UtamiNo ratings yet
- Intracardiac PressuresDocument41 pagesIntracardiac Pressureswaleed315No ratings yet
- Heart Failure - Practice Essentials, Background, PathophysiologyDocument17 pagesHeart Failure - Practice Essentials, Background, PathophysiologyAshutosh SinghNo ratings yet
- Chapter 6 The Circulatory System of MammalsDocument30 pagesChapter 6 The Circulatory System of MammalsRethenaNo ratings yet
- Modern Management of Systolic Anterior Motion of The Mitral ValveDocument11 pagesModern Management of Systolic Anterior Motion of The Mitral ValveRodri EspinNo ratings yet
- CardiomegalyDocument91 pagesCardiomegalyMariquita Buenafe100% (1)