You might also like
- Comparative Analysis - History of Architecture, China, Japan, KoreaDocument14 pagesComparative Analysis - History of Architecture, China, Japan, KoreaMillenia domingoNo ratings yet
- Euphoria 2021 F K Anyone Whos Not A Sea Blob Part 2 Jules Script Teleplay Written by Sam Levinson and Hunter SchaferDocument40 pagesEuphoria 2021 F K Anyone Whos Not A Sea Blob Part 2 Jules Script Teleplay Written by Sam Levinson and Hunter SchaferMadalena Duarte7No ratings yet
- (R) Choep: IndicationDocument5 pages(R) Choep: IndicationAlina CrissNo ratings yet
- Incidence of Alveoloplasty PDFDocument4 pagesIncidence of Alveoloplasty PDFaleeza sanaNo ratings yet
- Arts - 9 - Quarter 3 Module 1Document4 pagesArts - 9 - Quarter 3 Module 1John Mark Prestoza100% (3)
- Keto LogDocument7 pagesKeto LogKim Justin InfantadoNo ratings yet
- Anticoagulant Pocket GuideDocument8 pagesAnticoagulant Pocket GuideDrew John Minardi100% (2)
- The Greenock HangingsDocument5 pagesThe Greenock HangingsInverclyde Community Development Trust100% (2)
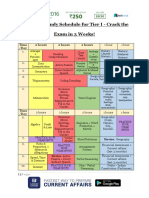
- SSC CHSL Study Schedule For Tier I - Crack The Exam in 3 Weeks!Document3 pagesSSC CHSL Study Schedule For Tier I - Crack The Exam in 3 Weeks!Tushita80% (15)
- Business Law Syllabus (BLT)Document4 pagesBusiness Law Syllabus (BLT)Glene NallaNo ratings yet
- Aminoglycoside & VancomycinDocument10 pagesAminoglycoside & VancomycinKhor Chin PooNo ratings yet
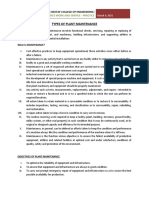
- Types of Plant MaintenanceDocument7 pagesTypes of Plant MaintenanceTHEOPHILUS ATO FLETCHERNo ratings yet
- Ix-karmapa-The Chariot For Traveling The Supreme PathDocument54 pagesIx-karmapa-The Chariot For Traveling The Supreme Pathssm100% (1)
- Flag V7 3.15Document2 pagesFlag V7 3.15GabrielNo ratings yet
- Nilotinib V4 4.13Document2 pagesNilotinib V4 4.13GabrielNo ratings yet
- L 51 R Hypercvad R MaDocument7 pagesL 51 R Hypercvad R MaMohamed MahmoudNo ratings yet
- Abvd V6 6.14Document2 pagesAbvd V6 6.14GabrielNo ratings yet
- Pentostatin V4 6.14Document2 pagesPentostatin V4 6.14GabrielNo ratings yet
- Lamivudine: in Vitro Studies Indicate That Zidovudine-Resistant Virus Isolates Can Become ZidovudineDocument7 pagesLamivudine: in Vitro Studies Indicate That Zidovudine-Resistant Virus Isolates Can Become ZidovudineKirtikrushna Suresh Prasad OjhaNo ratings yet
- Cyclosporine PDFDocument6 pagesCyclosporine PDFFazdrah AssyuaraNo ratings yet
- Annex I Summary of Product CharacteristicsDocument30 pagesAnnex I Summary of Product CharacteristicsPharmaEducationNo ratings yet
- Drug Monograph: Generic Name: Trade Name: Drug Class: IndicationsDocument10 pagesDrug Monograph: Generic Name: Trade Name: Drug Class: IndicationsRawan AlmutairiNo ratings yet
- L 13 High Dose Methotrexate High Grade NHL Cns ProphylaxisDocument6 pagesL 13 High Dose Methotrexate High Grade NHL Cns ProphylaxisHanin MaharNo ratings yet
- Aida Protocol For Apl: InductionDocument4 pagesAida Protocol For Apl: InductionGabrielNo ratings yet
- Apixaban Eliquis MonographDocument14 pagesApixaban Eliquis MonographTran Minh NgocNo ratings yet
- Rebozet Tykerb PDFDocument33 pagesRebozet Tykerb PDFWinda AgustinaNo ratings yet
- Docetaxel Carboplatin Trastuzumab T Carbo H Breast Cancer Adjuvant ProtocolDocument14 pagesDocetaxel Carboplatin Trastuzumab T Carbo H Breast Cancer Adjuvant ProtocolsmokkerNo ratings yet
- Nursing ResponsibilitiesDocument4 pagesNursing ResponsibilitiesMaureen Joy Cascayan EspirituNo ratings yet
- Management of Severe Ulcerative Colitis: DR - Siddharth SinghDocument21 pagesManagement of Severe Ulcerative Colitis: DR - Siddharth SinghLohith VakacherlaNo ratings yet
- Summary of Product Characteristics: For A Full List of Excipients, See Section 6.1Document17 pagesSummary of Product Characteristics: For A Full List of Excipients, See Section 6.1umarn1582No ratings yet
- Chemotherapy Protocol: RegimenDocument6 pagesChemotherapy Protocol: RegimenAlexandra AndronescuNo ratings yet
- Olaparib BRCA Mutated HER2 Negative Early Breast CancerDocument8 pagesOlaparib BRCA Mutated HER2 Negative Early Breast CancersmokkerNo ratings yet
- ClarithromycinDocument4 pagesClarithromycinGAYATHIRINo ratings yet
- Tishk International University: ApixabanDocument4 pagesTishk International University: ApixabanDyar MzafarNo ratings yet
- DI Query - 3Document5 pagesDI Query - 3uneesolutionsNo ratings yet
- Cablivi Epar Product Information - enDocument39 pagesCablivi Epar Product Information - enSuh TeixeiraNo ratings yet
- Group 3 5acl CML Core Prime FarmDocument29 pagesGroup 3 5acl CML Core Prime FarmAubey TanNo ratings yet
- Pembrolizumab With Carboplatin Paclitaxel and EC Neoadjuvant Breast Cancer Regimen Followed by Adjuvant PembrolizumabDocument17 pagesPembrolizumab With Carboplatin Paclitaxel and EC Neoadjuvant Breast Cancer Regimen Followed by Adjuvant PembrolizumabsmokkerNo ratings yet
- Azacitidine V2 4.14Document3 pagesAzacitidine V2 4.14GabrielNo ratings yet
- Heparin Dose Adjustment in The Prescence of Renal ImpairmentDocument5 pagesHeparin Dose Adjustment in The Prescence of Renal ImpairmentRPR KSVNo ratings yet
- ABVDDocument3 pagesABVDEsther WanguiNo ratings yet
- Endometrial Cancer - Pharmacologic Management - Cancer Therapy AdvisorDocument18 pagesEndometrial Cancer - Pharmacologic Management - Cancer Therapy AdvisorIrfan FathurrahmanNo ratings yet
- 1.13 Hyper-CVAD-MA Version 2.1Document5 pages1.13 Hyper-CVAD-MA Version 2.1Alina CrissNo ratings yet
- Avelumab 800 MGDocument9 pagesAvelumab 800 MGVlad CroitoruNo ratings yet
- Oseltamivir Indication, Dosage, Side Effect, Precaution MIMS IndonesiaDocument1 pageOseltamivir Indication, Dosage, Side Effect, Precaution MIMS Indonesiaintan alvinnNo ratings yet
- Accofil Epar Product Information enDocument155 pagesAccofil Epar Product Information endora192424No ratings yet
- Cytarabine Subcut V4 4.14Document1 pageCytarabine Subcut V4 4.14GabrielNo ratings yet
- Plazomicin - Drug Information - UpToDateDocument13 pagesPlazomicin - Drug Information - UpToDateMarius PapuricaNo ratings yet
- CMSCN RCHOP HighDocument3 pagesCMSCN RCHOP HighsatishNo ratings yet
- Hemostan, Methergine CA Gluconate2Document4 pagesHemostan, Methergine CA Gluconate2Stacy MC PelitoNo ratings yet
- Receiving Concurrent Moderate CYP3A4 Inhibitors (Erythromycin, Saquinavir, Verapamil, Fluconazole) - 25 MG Once Daily InitiallyDocument272 pagesReceiving Concurrent Moderate CYP3A4 Inhibitors (Erythromycin, Saquinavir, Verapamil, Fluconazole) - 25 MG Once Daily InitiallyFatima Doran PandaogNo ratings yet
- Pyra TBDocument6 pagesPyra TBRaya Ibarra LumogdangNo ratings yet
- New Zealand Data Sheet: 1. Product NameDocument22 pagesNew Zealand Data Sheet: 1. Product NamexoloNo ratings yet
- R GCVP V2 2.15Document3 pagesR GCVP V2 2.15GabrielNo ratings yet
- Cyclosporin Final (1) - 1-EditDocument32 pagesCyclosporin Final (1) - 1-Editsky.blueNo ratings yet
- Perindopril ErbumineDocument8 pagesPerindopril ErbumineYanna Habib-MangotaraNo ratings yet
- REBOZETDocument28 pagesREBOZETAndronikus DharmawanNo ratings yet
- Ribociclib: Protocol Ref: Mpharibobr (Version No: 1.1)Document10 pagesRibociclib: Protocol Ref: Mpharibobr (Version No: 1.1)Joana JohnNo ratings yet
- Class Indications: GentamicinDocument3 pagesClass Indications: GentamicinBer Anne Jaropojop TahilNo ratings yet
- Aus Pi TargocidDocument5 pagesAus Pi TargocidAsto Ata InteristiNo ratings yet
- Neratinib Adjuvant Treatment Breast Cancer Protocol V1.1Document6 pagesNeratinib Adjuvant Treatment Breast Cancer Protocol V1.1smokkerNo ratings yet
- Brajcefg Protocol 1feb2014Document4 pagesBrajcefg Protocol 1feb2014Rasha EmadNo ratings yet
- LUAVAFAT ProtocolDocument6 pagesLUAVAFAT Protocolthanh ngôNo ratings yet
- Vesanoid (Tretinoin) Capsules R Only Warnings 1. Experienced Physician and InstitutionDocument14 pagesVesanoid (Tretinoin) Capsules R Only Warnings 1. Experienced Physician and InstitutionArun GargNo ratings yet
- Capecitabine 14 DayDocument6 pagesCapecitabine 14 DaybrystyyNo ratings yet
- OB, Lactation, Pedi:: Route Onset Peak DurationDocument2 pagesOB, Lactation, Pedi:: Route Onset Peak Durationfryeabel1No ratings yet
- Tretinoin (All Trans Retinoic Acid)Document2 pagesTretinoin (All Trans Retinoic Acid)GabrielNo ratings yet
- R Bendamustine 90 For Low Grade NHL V2 2.15Document2 pagesR Bendamustine 90 For Low Grade NHL V2 2.15GabrielNo ratings yet
- R GCVP V2 2.15Document3 pagesR GCVP V2 2.15GabrielNo ratings yet
- Pentostatin V4 6.14Document2 pagesPentostatin V4 6.14GabrielNo ratings yet
- Melphalan Oral V3 7.11Document2 pagesMelphalan Oral V3 7.11GabrielNo ratings yet
- Intravenous Mel Dex July 08 Checked in Date Oct 2011Document2 pagesIntravenous Mel Dex July 08 Checked in Date Oct 2011GabrielNo ratings yet
- ISC EconomicsDocument49 pagesISC Economicskrittika190% (1)
- Latihan Soal Dan Evaluasi Materi ComplimentDocument6 pagesLatihan Soal Dan Evaluasi Materi ComplimentAvildaAfrinAmmaraNo ratings yet
- Refrigeration Technology: SymbolsDocument44 pagesRefrigeration Technology: SymbolsGaluh AjengNo ratings yet
- Humanities SculptureDocument15 pagesHumanities SculpturehungrynomadphNo ratings yet
- GoKReport1819Final 23091uDocument28 pagesGoKReport1819Final 23091uGurukrupa DasNo ratings yet
- 312 Listening List III FinalDocument2 pages312 Listening List III FinalJakeNo ratings yet
- Nine Competencies For HR Excellence Cheat Sheet: by ViaDocument1 pageNine Competencies For HR Excellence Cheat Sheet: by ViaRavi KumarNo ratings yet
- Deutscher National-KatechismusDocument3 pagesDeutscher National-KatechismusitsgabbywanNo ratings yet
- Vibration Control Technology Industry (Freudenberg Schwab)Document111 pagesVibration Control Technology Industry (Freudenberg Schwab)ismailNo ratings yet
- 120 Ways To Get Leads: Chuck HolmesDocument7 pages120 Ways To Get Leads: Chuck HolmesfirasdaherNo ratings yet
- Week 1Document15 pagesWeek 1Jamaica AlejoNo ratings yet
- CH 1 Cases - Mcqs CH 1 Cases - McqsDocument55 pagesCH 1 Cases - Mcqs CH 1 Cases - McqsChaudhary AdeelNo ratings yet
- The Role of Customer Knowledge Management (CKM) in Improving Organization-Customer RelationshipDocument7 pagesThe Role of Customer Knowledge Management (CKM) in Improving Organization-Customer RelationshipAbdul LathifNo ratings yet
- Book Review - 1: Reviewer: Devajyoti BiswasDocument3 pagesBook Review - 1: Reviewer: Devajyoti BiswassaemoonNo ratings yet
- Tan Shuy v. MaulawinDocument10 pagesTan Shuy v. MaulawinheyoooNo ratings yet
- Job Offer Electrical EngineerDocument3 pagesJob Offer Electrical EngineerAbner ZaldivarNo ratings yet
- Clam Antivirus 0.100.0 User ManualDocument34 pagesClam Antivirus 0.100.0 User ManualJacobus SulastriNo ratings yet
- Timeline of My Exposure To Traditional and New Media - Justine Sheen Gay-12 ABM-BDocument16 pagesTimeline of My Exposure To Traditional and New Media - Justine Sheen Gay-12 ABM-Bapi-389627320No ratings yet
- Dead Poets SocietyDocument1 pageDead Poets SocietyNagy ZenteNo ratings yet
- Global Forecasts DiscussionDocument10 pagesGlobal Forecasts DiscussionkareemarfaNo ratings yet
- 5990200Document551 pages5990200Basit Ahmad bhat0% (1)