You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Nissan Note E-Power 2022 Quick Guide ENDocument57 pagesNissan Note E-Power 2022 Quick Guide ENSarita EmmanuelNo ratings yet
- Probability Theory - VaradhanDocument6 pagesProbability Theory - VaradhanTom HenNo ratings yet
- Lesson Exemplar Math 7Document6 pagesLesson Exemplar Math 7Pablo Jimenea100% (2)
- Akut AbdomenDocument24 pagesAkut AbdomenEka100% (1)
- Money Order Sauce.Document2 pagesMoney Order Sauce.randomNo ratings yet
- Genotype - Accupower Jak2Document34 pagesGenotype - Accupower Jak2Elvan Dwi WidyadiNo ratings yet
- (Concentration: 30ng/ul Purity A260/280: 1.7) : Sample: Blood EDTA PCR PreparationDocument2 pages(Concentration: 30ng/ul Purity A260/280: 1.7) : Sample: Blood EDTA PCR PreparationElvan Dwi WidyadiNo ratings yet
- (Concentration: 30ng/ul Purity A260/280: 1.7) : Sample: Blood EDTA PCR PreparationDocument2 pages(Concentration: 30ng/ul Purity A260/280: 1.7) : Sample: Blood EDTA PCR PreparationElvan Dwi WidyadiNo ratings yet
- BV Blue TestDocument4 pagesBV Blue TestElvan Dwi WidyadiNo ratings yet
- QC Levey-Jenning WestgurdDocument8 pagesQC Levey-Jenning WestgurdElvan Dwi WidyadiNo ratings yet
- Menejeman LabDocument3 pagesMenejeman LabElvan Dwi WidyadiNo ratings yet
- LaboratoryQualityStandardsandtheirImplementation 9C27 PDFDocument74 pagesLaboratoryQualityStandardsandtheirImplementation 9C27 PDFElvan Dwi WidyadiNo ratings yet
- Pgl1 Penanda Lepra: Elvan, DR/ DR - Puspa Wardani,. Dr. SP - PKDocument8 pagesPgl1 Penanda Lepra: Elvan, DR/ DR - Puspa Wardani,. Dr. SP - PKElvan Dwi WidyadiNo ratings yet
- Rencana Pelaksanaan PembelajaranDocument5 pagesRencana Pelaksanaan PembelajaranElvan Dwi WidyadiNo ratings yet
- Performance of Bvblue Rapid Test in Detecting Bacterial Vaginosis Among Women in Mysore, IndiaDocument1 pagePerformance of Bvblue Rapid Test in Detecting Bacterial Vaginosis Among Women in Mysore, IndiaElvan Dwi Widyadi100% (1)
- Hem Lab6 RBC Morph Incl F12Document7 pagesHem Lab6 RBC Morph Incl F12Elvan Dwi WidyadiNo ratings yet
- Glycatedalbumin (GA)Document22 pagesGlycatedalbumin (GA)Elvan Dwi WidyadiNo ratings yet
- Wesgardrules & MultirulesDocument18 pagesWesgardrules & MultirulesElvan Dwi WidyadiNo ratings yet
- From The Sample To The Reading, Indirect ELISA Protocol: Buffer PreparationDocument2 pagesFrom The Sample To The Reading, Indirect ELISA Protocol: Buffer PreparationElvan Dwi WidyadiNo ratings yet
- Opini: Everybody in This World Has Dream. Whoever They Are, Wherever They Are FromDocument3 pagesOpini: Everybody in This World Has Dream. Whoever They Are, Wherever They Are FromElvan Dwi WidyadiNo ratings yet
- Phosphate BishopDocument3 pagesPhosphate BishopElvan Dwi WidyadiNo ratings yet
- Sysmex Ca 600Document4 pagesSysmex Ca 600Elvan Dwi WidyadiNo ratings yet
- UrinalysisDocument10 pagesUrinalysisElvan Dwi WidyadiNo ratings yet
- Test Detail: Tes Tariff Registration Date Test Start Date Start Time Finish TimeDocument1 pageTest Detail: Tes Tariff Registration Date Test Start Date Start Time Finish TimeElvan Dwi WidyadiNo ratings yet
- Head & Brain Trauma: EMS Professions Temple CollegeDocument77 pagesHead & Brain Trauma: EMS Professions Temple CollegeElvan Dwi WidyadiNo ratings yet
- Medrano, Rene LynnDocument2 pagesMedrano, Rene LynnRene Lynn Labing-isa Malik-MedranoNo ratings yet
- Chapter Two: General Design ConsiderationsDocument27 pagesChapter Two: General Design ConsiderationsTeddy Ekubay GNo ratings yet
- Performance Comparison of VxWorks Linux RTAI and Xenomai in A Hard Real-Time ApplicationDocument5 pagesPerformance Comparison of VxWorks Linux RTAI and Xenomai in A Hard Real-Time ApplicationsatyanaryanakNo ratings yet
- Mba633 Road To Hell Case AnalysisDocument3 pagesMba633 Road To Hell Case AnalysisAditi VarshneyNo ratings yet
- 22 Thành NG Quen Thu C Trên Ielts - FirefighterDocument2 pages22 Thành NG Quen Thu C Trên Ielts - FirefighterNinh NguyễnNo ratings yet
- Plastic Hinge Length and Depth For Piles in Marine Oil Terminals Including Nonlinear Soil PropertiesDocument10 pagesPlastic Hinge Length and Depth For Piles in Marine Oil Terminals Including Nonlinear Soil PropertiesGopu RNo ratings yet
- Pascal Die Casting Machine SystemDocument20 pagesPascal Die Casting Machine Systemenascimento32No ratings yet
- Scan WV1DB12H4B8018760 20210927 1800Document6 pagesScan WV1DB12H4B8018760 20210927 1800Sergio AlvarezNo ratings yet
- Evidence MODULE 1 Evidence DefinitionDocument8 pagesEvidence MODULE 1 Evidence Definitiondave BarretoNo ratings yet
- Empowerment Technology Lesson 4 PDFDocument18 pagesEmpowerment Technology Lesson 4 PDFqueenless eightyoneNo ratings yet
- Manitou 1350RDocument4 pagesManitou 1350RcandlaganNo ratings yet
- n4 HandoutDocument2 pagesn4 HandoutFizzerNo ratings yet
- HP Scanjet Pro 2500 F1 Flatbed Scanner: Boost Productivity With Fast, Versatile ScanningDocument2 pagesHP Scanjet Pro 2500 F1 Flatbed Scanner: Boost Productivity With Fast, Versatile ScanningParesh BabariaNo ratings yet
- Calculation ReportDocument157 pagesCalculation Reportisaacjoe77100% (3)
- Hume 100 ReviewerDocument7 pagesHume 100 ReviewerShai GaviñoNo ratings yet
- Unit 3Document5 pagesUnit 3Narasimman DonNo ratings yet
- Measures of Indicator 1Document2 pagesMeasures of Indicator 1ROMMEL BALAN CELSONo ratings yet
- SemDocument583 pagesSemMaria SantosNo ratings yet
- Credit Card Authorization Form WoffordDocument1 pageCredit Card Authorization Form WoffordRaúl Enmanuel Capellan PeñaNo ratings yet
- CS3501 Compiler Design Lab ManualDocument43 pagesCS3501 Compiler Design Lab ManualMANIMEKALAINo ratings yet
- Toftejorg TZ-75 Rotary Jet Head - Portable: Fast, Effective Impact CleaningDocument3 pagesToftejorg TZ-75 Rotary Jet Head - Portable: Fast, Effective Impact CleaningSamo SpontanostNo ratings yet
- UntitledDocument5 pagesUntitledapril montejoNo ratings yet
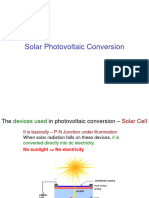
- Slide 7 PV NewDocument74 pagesSlide 7 PV NewPriyanshu AgrawalNo ratings yet
- Effect of Minor and Trace Elements in Cast IronDocument2 pagesEffect of Minor and Trace Elements in Cast IronsachinguptachdNo ratings yet
- Application Letter For Promotion T2 T3Document24 pagesApplication Letter For Promotion T2 T3FGacadSabadoNo ratings yet
- Topic 3 Intellectual RevolutionDocument20 pagesTopic 3 Intellectual RevolutionOlive April TampipiNo ratings yet