You might also like
- Dengue FeverDocument7 pagesDengue FeverAmber Hope PonsicaNo ratings yet
- The Story of GregorioDocument2 pagesThe Story of GregorioKelly LegaspiNo ratings yet
- Nursing Management of CVA and NIDDMDocument12 pagesNursing Management of CVA and NIDDMKaloy KamaoNo ratings yet
- NCP Dengue CabadingDocument3 pagesNCP Dengue CabadingHannah Angelu CabadingNo ratings yet
- Activity Gene TherapyDocument3 pagesActivity Gene TherapyKent Gabriel YangaoNo ratings yet
- Dengue FeverDocument27 pagesDengue FeverHari Mukti100% (4)
- Impaired SwallowingDocument2 pagesImpaired SwallowingfaizaNo ratings yet
- Sit AnDocument6 pagesSit AnbabiNo ratings yet
- Nursing Interview Guide - HA - VIOSDocument9 pagesNursing Interview Guide - HA - VIOSIra Velle ViosNo ratings yet
- NCP UtiDocument1 pageNCP UtiAgentpiinkkNo ratings yet
- Ecologic ModelDocument2 pagesEcologic Modelchardy101No ratings yet
- A Case Study On DengueDocument11 pagesA Case Study On DengueYetTamparong100% (1)
- Ecologic ModelDocument2 pagesEcologic Modelluis_chubeeNo ratings yet
- Measles Final Vishal Brochure PDFDocument2 pagesMeasles Final Vishal Brochure PDFVishal Kunnathur SenthilkumarNo ratings yet
- Assignment For Oxy. Online BasedDocument5 pagesAssignment For Oxy. Online BasedNurhassem Nor AkangNo ratings yet
- NCP For Bronchopneumonia With 7 Nursing DiagnosisDocument4 pagesNCP For Bronchopneumonia With 7 Nursing DiagnosisBeng AlontoNo ratings yet
- Koizer DDocument2 pagesKoizer DkoizerNo ratings yet
- NCP On DyspneaDocument5 pagesNCP On DyspneaDizzy BualanNo ratings yet
- Influenza PATHOPHYSIOLOGYDocument3 pagesInfluenza PATHOPHYSIOLOGYElle RosalesNo ratings yet
- BFCDocument8 pagesBFCIrene GunongNo ratings yet
- Adult 3 FinalDocument29 pagesAdult 3 Finalأبوأحمد الحكيم100% (1)
- NCP AppendectomyDocument10 pagesNCP Appendectomy100lNo ratings yet
- MODULE-9-Biotechnology, Genetically Modified Organisms, and Gene TherapyDocument5 pagesMODULE-9-Biotechnology, Genetically Modified Organisms, and Gene TherapyKerry NuñezNo ratings yet
- Pg36 37 of Pneumothorax Case StudyDocument2 pagesPg36 37 of Pneumothorax Case StudyCharles Dean Ugalde100% (2)
- Hyperventilation Syndrome 2021Document4 pagesHyperventilation Syndrome 2021tenri ashariNo ratings yet
- ChickenpoxDocument16 pagesChickenpoxJeet ThuraiNo ratings yet
- Anatomy and Physiology of The LungsDocument3 pagesAnatomy and Physiology of The LungsMayownski TejeroNo ratings yet
- Cyanobacteria: Figure 1. Microscopic Illustration of CyanobacteriaDocument7 pagesCyanobacteria: Figure 1. Microscopic Illustration of CyanobacteriaMichelle HutamaresNo ratings yet
- Community Service ReflectionDocument2 pagesCommunity Service Reflectionapi-236349398No ratings yet
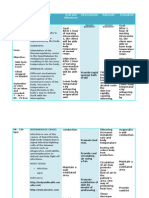
- Nursing Care Plan: Nursing Diagnosis Nursing Goals Nursing OutcomeDocument3 pagesNursing Care Plan: Nursing Diagnosis Nursing Goals Nursing OutcomemerryNo ratings yet
- Workshop 5 - Sampling DesignsDocument1 pageWorkshop 5 - Sampling DesignsJohn Victor B. FelixNo ratings yet
- Nursing Care Plan # 1:: Assessment Diagnosis Scientific Basis Planning Nursing Interventions Rationale EvaluationDocument11 pagesNursing Care Plan # 1:: Assessment Diagnosis Scientific Basis Planning Nursing Interventions Rationale EvaluationGj PaguidianNo ratings yet
- Acute Bronchitis Care Study 202Document25 pagesAcute Bronchitis Care Study 202Kara Kathrina Fuentes100% (1)
- B NCP On and Off Fever 2b ImproveddocxDocument6 pagesB NCP On and Off Fever 2b ImproveddocxKylie CatralNo ratings yet
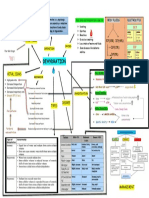
- Concept Map Group 1Document1 pageConcept Map Group 1eric macabiog100% (1)
- Carpal Tunnel SyndromeDocument25 pagesCarpal Tunnel SyndromeFranky Sukwendy100% (1)
- HyperthermiaDocument6 pagesHyperthermiaBerlyn FelicianoNo ratings yet
- Concept MapDocument1 pageConcept Mapadriana100% (1)
- NCP On Nerborn CareDocument7 pagesNCP On Nerborn CareMandeep KaurNo ratings yet
- Ppe4 Reflection AssignmentDocument11 pagesPpe4 Reflection Assignmentapi-318846856100% (1)
- Withering Flowers: A Multiple Case Study About The Life of An Elderly Inside A Home Care FacilityDocument67 pagesWithering Flowers: A Multiple Case Study About The Life of An Elderly Inside A Home Care FacilityRuben Medina SalvadorNo ratings yet
- Nursing SopDocument3 pagesNursing SopChelsy Sky SacanNo ratings yet
- Pathophysiology of Covid-19 Infection: What Is The Novel Coronavirus (Sars-Cov-2) Doing To Body? A Comprehensive Systematic ReviewDocument15 pagesPathophysiology of Covid-19 Infection: What Is The Novel Coronavirus (Sars-Cov-2) Doing To Body? A Comprehensive Systematic ReviewMade DeanaNo ratings yet
- University of Northern PhilippinesDocument30 pagesUniversity of Northern PhilippinesClaudine JaramilloNo ratings yet
- Ecologic ModelDocument4 pagesEcologic ModelJohnnette BedoniaNo ratings yet
- Case Scenario - NebulizationDocument2 pagesCase Scenario - NebulizationHilario. Hayascent.Reign.M.No ratings yet
- Rabi PurDocument3 pagesRabi PurDiana Laura LeiNo ratings yet
- NCP For Chronic PainDocument11 pagesNCP For Chronic PainRYAN SAPLADNo ratings yet
- Physical Assessment (Ippa)Document14 pagesPhysical Assessment (Ippa)Barbara HsuNo ratings yet
- PediculosisDocument14 pagesPediculosisREYMARK HACOSTA100% (1)
- Activity IntoleranceDocument1 pageActivity IntoleranceAndrea Francesca SantosNo ratings yet
- Soapie DocumentationDocument2 pagesSoapie DocumentationJubilee AngNo ratings yet
- NCP (Actual)Document2 pagesNCP (Actual)Silinna May Lee SanicoNo ratings yet
- Food and Waterborne Diseases Prevention and Control ProgramDocument3 pagesFood and Waterborne Diseases Prevention and Control ProgramRolena Johnette B. PiñeroNo ratings yet
- Fernandez, John PearlDocument2 pagesFernandez, John PearlJohn Pearl FernandezNo ratings yet
- Dengue Fever: A Case ManagementDocument11 pagesDengue Fever: A Case ManagementRez ApegoNo ratings yet
- Nursing Care PlanDocument1 pageNursing Care PlanMikki lor PuaganNo ratings yet
- Teaching PlanDocument3 pagesTeaching PlanJaninaPatriciaB100% (2)
- Chapter 9 Dengue Fever 1Document9 pagesChapter 9 Dengue Fever 1Kyla BalboaNo ratings yet
- What Is Dengue Fever?Document9 pagesWhat Is Dengue Fever?Sk RiazNo ratings yet
- Statement Uni - SenithaDocument2 pagesStatement Uni - SenithaSenitha MindulaNo ratings yet
- WI-962353 QEL03 Audit Plan LetterDocument3 pagesWI-962353 QEL03 Audit Plan LetterChakky DestinyNo ratings yet
- MSDS Serat Kaca PDFDocument11 pagesMSDS Serat Kaca PDFGita AzhariNo ratings yet
- World Bank & It's SubsidiariesDocument20 pagesWorld Bank & It's Subsidiariesamar635No ratings yet
- Atherosclerosis and Ischemic Heart Disease: UtlineDocument8 pagesAtherosclerosis and Ischemic Heart Disease: UtlinevmdcabanillaNo ratings yet
- Uganda Institute of Allied Health and Management Sciences - MulagoDocument8 pagesUganda Institute of Allied Health and Management Sciences - MulagoMartin SageNo ratings yet
- BioMedical Waste Management Issues ChallengesDocument23 pagesBioMedical Waste Management Issues ChallengesArun Shree RNo ratings yet
- SF2 - 2020 - Grade 6 - MALINISDocument2 pagesSF2 - 2020 - Grade 6 - MALINISJerson S. SantiagoNo ratings yet
- TZ Dairy Industry FAODocument46 pagesTZ Dairy Industry FAOKai GwalandaNo ratings yet
- Cardiac Troponin I Leve in STEMI and Clinical Correlation With LeftVentricular Dysfunction in Indian Population 2329 9517.1000116Document6 pagesCardiac Troponin I Leve in STEMI and Clinical Correlation With LeftVentricular Dysfunction in Indian Population 2329 9517.1000116panjiNo ratings yet
- SOP For Handling of Tablet Counter - Pharmaceutical Guidelines PDFDocument1 pageSOP For Handling of Tablet Counter - Pharmaceutical Guidelines PDFmeet2abhayNo ratings yet
- Healthmedicinet Com II 2014 AugDocument400 pagesHealthmedicinet Com II 2014 AugHeal ThmedicinetNo ratings yet
- Chapter 1-3Document35 pagesChapter 1-3pontiveros.fc67% (3)
- Healthy Food EssayDocument2 pagesHealthy Food EssayFebri FebrianiNo ratings yet
- 2-Personality - Humanistic TheoryDocument23 pages2-Personality - Humanistic TheorySindhu BabuNo ratings yet
- List of Crash Cart SuppliesDocument2 pagesList of Crash Cart SuppliesMariefel Villanueva AlejagaNo ratings yet
- Unlock Your Tight Hip FlexorsDocument63 pagesUnlock Your Tight Hip FlexorsPina Olson Campbell100% (2)
- Q3-PPT-HEALTH10 - Significance of Global Health InitiativesDocument20 pagesQ3-PPT-HEALTH10 - Significance of Global Health InitiativesJewel Emerald100% (8)
- 04.4 Sea April 2021 R4Document205 pages04.4 Sea April 2021 R4Pranay PatelNo ratings yet
- Running Head: Improving Care For Patients With HypertensionDocument6 pagesRunning Head: Improving Care For Patients With HypertensionCliff KaaraNo ratings yet
- Ellen Respiratory Module PortraitDocument11 pagesEllen Respiratory Module PortraitAbdelmar SusulanNo ratings yet
- AnxolamDocument38 pagesAnxolammanjitdeshmukh2No ratings yet
- MASUK MIAH POLAND AppointmentDocument3 pagesMASUK MIAH POLAND Appointmentkaisarmukadam100% (1)
- Ha NotesDocument34 pagesHa NotesLyssa KateNo ratings yet
- Complementary Feeding in Infants: An Ayurvedic Overview: ArticleDocument7 pagesComplementary Feeding in Infants: An Ayurvedic Overview: ArticleRadhika RNo ratings yet
- Married To The Job: How A Long-Hours Working Culture Keeps People Single and LonelyDocument12 pagesMarried To The Job: How A Long-Hours Working Culture Keeps People Single and LonelyDaxten KienNo ratings yet
- Jurnal Forensik 1Document7 pagesJurnal Forensik 1Rizky ErizkaNo ratings yet
- Purine Rich FoodDocument3 pagesPurine Rich Foodttstanescu4506No ratings yet
- Ortho PresentationDocument10 pagesOrtho PresentationarchanaNo ratings yet
- Manual For Doctors To Evaluate Permanent Physical ImpairmentDocument33 pagesManual For Doctors To Evaluate Permanent Physical Impairmentyuvrajavi100% (1)