You might also like
- Chronic Pain Management: Dr. Ankit GajjarDocument74 pagesChronic Pain Management: Dr. Ankit GajjarDivya Rekha KolliNo ratings yet
- Neurological AssessmentDocument43 pagesNeurological AssessmentBhoransh VatsNo ratings yet
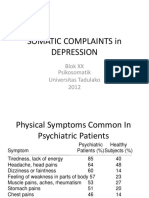
- Somatic Complaints in Depression Psikosomatik Untad 2012Document19 pagesSomatic Complaints in Depression Psikosomatik Untad 2012Muhammad mukramNo ratings yet
- cnCIzdCeRBewaZ4AOGFq - Narcolepsy Talk Psychiatry Update 2020 FINALDocument21 pagescnCIzdCeRBewaZ4AOGFq - Narcolepsy Talk Psychiatry Update 2020 FINALKreshnik IdrizajNo ratings yet
- Psycho-Social Aspects of Pain-1Document29 pagesPsycho-Social Aspects of Pain-1nugraha sultanNo ratings yet
- 'Urdaneta City University College of Health Sciences: Bachelor of Science in NursingDocument4 pages'Urdaneta City University College of Health Sciences: Bachelor of Science in NursingDan Dan ManaoisNo ratings yet
- Epidemiology and Definition: o Most Common Locations: o Acute PainDocument4 pagesEpidemiology and Definition: o Most Common Locations: o Acute PainJudy Ignacio EclarinoNo ratings yet
- Effectiveness of Myofascial Trigger Point Release Technique To Evaluate Pain in Chronic Tension Type Headache Patients.Document40 pagesEffectiveness of Myofascial Trigger Point Release Technique To Evaluate Pain in Chronic Tension Type Headache Patients.Dr.Gopinath SaravananNo ratings yet
- Materi Webinar Morfin MartinDocument70 pagesMateri Webinar Morfin Martinfatma watiNo ratings yet
- NM20110200002 13838543Document7 pagesNM20110200002 13838543Roy AriadyNo ratings yet
- Aaf85c-A6e5-7c84-8365-8b1cb2640f45 Free BCP Quick Reference GuidesDocument3 pagesAaf85c-A6e5-7c84-8365-8b1cb2640f45 Free BCP Quick Reference GuidesDavid StreisselNo ratings yet
- Beyond Sadness PowerpointDocument12 pagesBeyond Sadness PowerpointJoanne BlancoNo ratings yet
- Complex Regional Pain SyndromeDocument27 pagesComplex Regional Pain SyndromeKapil LakhwaraNo ratings yet
- MEGHA A S Project Ppt-1Document20 pagesMEGHA A S Project Ppt-1Sachin AbsNo ratings yet
- Data Nursing Diagnos IS Scientific Backgrou ND Goal/Objective Nursing Interventions Rationale EvaluationDocument4 pagesData Nursing Diagnos IS Scientific Backgrou ND Goal/Objective Nursing Interventions Rationale EvaluationDienizs LabiniNo ratings yet
- Dry Needling e Sono 2019Document13 pagesDry Needling e Sono 2019Rafel FisioNo ratings yet
- Multiple Sclerosis: Saadia Perwaiz, PT BSPT, M. Phil-MskDocument39 pagesMultiple Sclerosis: Saadia Perwaiz, PT BSPT, M. Phil-MskArslan Aslam100% (2)
- Bell TylerDocument18 pagesBell Tylerhelenlamlam200011No ratings yet
- J JMPT 2012 09 003Document6 pagesJ JMPT 2012 09 003Tahira RajputNo ratings yet
- Prevalence and Incidence of Shoulder Pain in The General Population A Systematic ReviewDocument9 pagesPrevalence and Incidence of Shoulder Pain in The General Population A Systematic ReviewOmar CirineoNo ratings yet
- In Uenceofcraniosacral Therapy On Anxiety, Depression and Quality of Life in Patients With FibromyalgiaDocument9 pagesIn Uenceofcraniosacral Therapy On Anxiety, Depression and Quality of Life in Patients With FibromyalgiaGiovanniNo ratings yet
- Acute Pain Management FDK RSUD KLDocument36 pagesAcute Pain Management FDK RSUD KLAgoenk PrabowoNo ratings yet
- Orofacial PainDocument7 pagesOrofacial PainAkram AlsharaeeNo ratings yet
- Pain Acute Chronic: Nociceptive Pain Neuropathic Pain Mixed or Unspecified Pain Pain Due To Psychological DisordersDocument3 pagesPain Acute Chronic: Nociceptive Pain Neuropathic Pain Mixed or Unspecified Pain Pain Due To Psychological DisordersPaigufanNo ratings yet
- Nursing Care Plan Age: 60 Years OldDocument4 pagesNursing Care Plan Age: 60 Years OldLouise GudmalinNo ratings yet
- Pleno p2 Musket Kelompok 2Document51 pagesPleno p2 Musket Kelompok 2Ade Cahyo IslamiNo ratings yet
- 5Document10 pages5doctorhealthNo ratings yet
- Articulo #4Document9 pagesArticulo #4Jorge GámezNo ratings yet
- Progressive Muscle RelaxationDhandapanietalDocument13 pagesProgressive Muscle RelaxationDhandapanietalS.N HanifahNo ratings yet
- Role of A Nurse in Palliative Care: Jhessie L. Abella, RN, RM, MANDocument64 pagesRole of A Nurse in Palliative Care: Jhessie L. Abella, RN, RM, MANaramulescuNo ratings yet
- Health Assessment Notes Pain and ViolenceDocument5 pagesHealth Assessment Notes Pain and ViolenceDazell VarronNo ratings yet
- Pain Management PDFDocument38 pagesPain Management PDFYulia Fransisca PurbaNo ratings yet
- Understand Why You Hurt All Over and What You Can Take To Stop The PainDocument48 pagesUnderstand Why You Hurt All Over and What You Can Take To Stop The Painhasan fehmi ocakNo ratings yet
- TM and Therapy PDFDocument46 pagesTM and Therapy PDFljlNo ratings yet
- Assessing Pain in Older Adults With DementiaDocument2 pagesAssessing Pain in Older Adults With DementiaLucia CorlatNo ratings yet
- Assessing Pain: Fifth Vital SignDocument10 pagesAssessing Pain: Fifth Vital SignShaira Dawn D. PLANCONo ratings yet
- Print 10Document4 pagesPrint 10FARAH MOHAMMEDNo ratings yet
- Health Assessment in Nursing (LEC)Document50 pagesHealth Assessment in Nursing (LEC)Cj MayoyoNo ratings yet
- Treating Somatization: A Multimodal ApproachDocument7 pagesTreating Somatization: A Multimodal ApproachDr. Ranjan KumarNo ratings yet
- Somatization: Diagnosing It Sooner Through Emotion-Focused InterviewingDocument10 pagesSomatization: Diagnosing It Sooner Through Emotion-Focused Interviewingscribd4kmhNo ratings yet
- Complex Regional Pain Syndrome: Stephen BruehlDocument13 pagesComplex Regional Pain Syndrome: Stephen BruehlAnaGravíssimaNo ratings yet
- Infectious DemoDocument42 pagesInfectious DemoLaura TapiaNo ratings yet
- Reflexology & Diabetic NeuropathyDocument50 pagesReflexology & Diabetic NeuropathyDr Vaishali MathapatiNo ratings yet
- Correlations Between Brain Changes and Pain Management After Cognitive and Meditative Therapies - A Systematic Review of Neuroimaging Studies-2018Document9 pagesCorrelations Between Brain Changes and Pain Management After Cognitive and Meditative Therapies - A Systematic Review of Neuroimaging Studies-2018Juan ParedesNo ratings yet
- Risk For Acute Pain Related To Surgical IncisionDocument4 pagesRisk For Acute Pain Related To Surgical IncisionMia Grace Garcia100% (1)
- The Clinical and Cost-Effectiveness of Neurostimulation For Relief of Chronic Neuropathic PainDocument252 pagesThe Clinical and Cost-Effectiveness of Neurostimulation For Relief of Chronic Neuropathic PainTannov SiregarNo ratings yet
- MDT Education Updates 2015Document6 pagesMDT Education Updates 2015Tomáš KrajíčekNo ratings yet
- Diagnosis and Treatment of Myofascial Pain Syndrome Diagnosis Dan Tatalaksana Sindrom Nyeri MyofasialDocument12 pagesDiagnosis and Treatment of Myofascial Pain Syndrome Diagnosis Dan Tatalaksana Sindrom Nyeri MyofasialyuliaNo ratings yet
- 41 Handout Fibromyalgia in 60 SecondsDocument1 page41 Handout Fibromyalgia in 60 SecondsmariammemoredaNo ratings yet
- A Comparison of Somatic Symptoms Between Depressive Disorder and Somatoform DisorderDocument8 pagesA Comparison of Somatic Symptoms Between Depressive Disorder and Somatoform DisorderInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- SoftTissueMobilizationTechniques Foster PDFUpdateDocument11 pagesSoftTissueMobilizationTechniques Foster PDFUpdatemalindamaureen75No ratings yet
- History Taking: Hanzara PanolDocument27 pagesHistory Taking: Hanzara PanolHanzara PanolNo ratings yet
- Clinical Neurophysiology: Janneke Terhaar, Filipa Campos Viola, Karl-Jürgen Bär, Stefan DebenerDocument8 pagesClinical Neurophysiology: Janneke Terhaar, Filipa Campos Viola, Karl-Jürgen Bär, Stefan DebenersoylahijadeunvampiroNo ratings yet
- Brain Chronic PainDocument23 pagesBrain Chronic PainDedy SavradinataNo ratings yet
- Pain Assessment & ManagementDocument36 pagesPain Assessment & ManagementremeroseNo ratings yet
- Inhibition and Heart Rate Variability in ExperimenDocument11 pagesInhibition and Heart Rate Variability in ExperimenzuveriaNo ratings yet
- SD Dolor RegionalDocument8 pagesSD Dolor RegionalYadira SantosNo ratings yet
- 1 s2.0 S0007091217329677 MainDocument5 pages1 s2.0 S0007091217329677 MainAndy OrtizNo ratings yet
- Fibromyalgia: Basic InformationDocument5 pagesFibromyalgia: Basic InformationhectorNo ratings yet
- Bhimbra-GENERALIZED THEORY ELECTRICAL MACHINES PDFDocument582 pagesBhimbra-GENERALIZED THEORY ELECTRICAL MACHINES PDFdebasishmee5808No ratings yet
- Sophus 3Document1 pageSophus 3debasishmee5808No ratings yet
- Adjunct 2Document5 pagesAdjunct 2debasishmee5808No ratings yet
- Adaptive Control of Linearizable Systems: Fully-StateDocument9 pagesAdaptive Control of Linearizable Systems: Fully-Statedebasishmee5808No ratings yet
- Book ListDocument6 pagesBook Listdebasishmee58080% (1)
- Control System - I: Weekly Lesson PlanDocument5 pagesControl System - I: Weekly Lesson Plandebasishmee5808No ratings yet
- Electromagnetic Field TheoryDocument3 pagesElectromagnetic Field Theorydebasishmee5808No ratings yet
- Duplicate Doc Diploma CertiDocument1 pageDuplicate Doc Diploma Certidebasishmee5808No ratings yet
- Best Practices of Report Writing Based On Study of Reports: Venue: India Habitat Centre, New DelhiDocument24 pagesBest Practices of Report Writing Based On Study of Reports: Venue: India Habitat Centre, New Delhidebasishmee5808No ratings yet
- Graphical AbstractDocument2 pagesGraphical Abstractdebasishmee5808No ratings yet
- Adaptive Output Feedback Based On Closed-Loop Reference ModelsDocument6 pagesAdaptive Output Feedback Based On Closed-Loop Reference Modelsdebasishmee5808No ratings yet
- Comparison Between Integer Order and Fractional Order ControllersDocument6 pagesComparison Between Integer Order and Fractional Order Controllersdebasishmee5808No ratings yet
- Computers and Mathematics With Applications: Ramiro S. Barbosa, J.A. Tenreiro Machado, Isabel S. JesusDocument8 pagesComputers and Mathematics With Applications: Ramiro S. Barbosa, J.A. Tenreiro Machado, Isabel S. Jesusdebasishmee5808No ratings yet
- Medical Management Include Drug Therapy: Hydatidiform MoleDocument2 pagesMedical Management Include Drug Therapy: Hydatidiform MoleMaye ArugayNo ratings yet
- Foot CareDocument5 pagesFoot CareSarah EddiahNo ratings yet
- PP-MIR-US-0477-1 Mirena Patient Brochure DigitalDocument13 pagesPP-MIR-US-0477-1 Mirena Patient Brochure DigitalimtariqueNo ratings yet
- A Case Study On Renal CancerDocument5 pagesA Case Study On Renal CancerrlinaoNo ratings yet
- IBS Summit - FSD (Slide Deck) v2Document45 pagesIBS Summit - FSD (Slide Deck) v2shamail1No ratings yet
- Leiomioma - Histologia y PatogenesisDocument6 pagesLeiomioma - Histologia y PatogenesisNella SolanoNo ratings yet
- 4 Central Venous Pressure MonitoringDocument1 page4 Central Venous Pressure MonitoringCAROLYN BORDONNo ratings yet
- Gastropathy DMDocument7 pagesGastropathy DMIlham Suryo Wibowo AntonoNo ratings yet
- Rheumatic FeverDocument3 pagesRheumatic FeverPanji SaksonoNo ratings yet
- 334-Article Text-1213-1-10-20160514Document7 pages334-Article Text-1213-1-10-20160514Balakrishna GopinathNo ratings yet
- 011 Exam Focus Dec 22Document25 pages011 Exam Focus Dec 22Moyooree BiswasNo ratings yet
- The Management of Common and Selected Psychiatric EmergenciesDocument129 pagesThe Management of Common and Selected Psychiatric EmergenciesHasaan Khan100% (1)
- NCP (Afp)Document7 pagesNCP (Afp)Summer SuarezNo ratings yet
- Assessment of The Respiratory SystemDocument49 pagesAssessment of The Respiratory SystemMilanisti22No ratings yet
- GIT System: Bader Al-Mukhtar - RCSI - SCDocument15 pagesGIT System: Bader Al-Mukhtar - RCSI - SCkinanNo ratings yet
- Ankylosing Spondylitis and HomoeopathyDocument12 pagesAnkylosing Spondylitis and HomoeopathyDr. Rajneesh Kumar Sharma MD HomNo ratings yet
- Low Back Pain ProposalDocument15 pagesLow Back Pain ProposalNur Faza RosliNo ratings yet
- Diseases o F Urinary System 5 LevelDocument6 pagesDiseases o F Urinary System 5 LevelABDULLAH AMROONNo ratings yet
- Family Medicine Miniosce SerotoninDocument14 pagesFamily Medicine Miniosce SerotoninSyed AhmedNo ratings yet
- D-37/1, TTC MIDC, Turbhe, Navi Mumbai-400 703: ThyrocareDocument3 pagesD-37/1, TTC MIDC, Turbhe, Navi Mumbai-400 703: ThyrocareSyed's Way PoolNo ratings yet
- Genetic Screening, Prenatal DiagnosisDocument56 pagesGenetic Screening, Prenatal DiagnosisLunaLure100% (1)
- Ruli, Novan - IcdDocument45 pagesRuli, Novan - IcdruliamriNo ratings yet
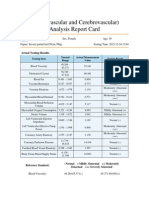
- Cardiovascular and CerebrovascularDocument6 pagesCardiovascular and CerebrovascularJoshelle B. Bancilo0% (1)
- Common Classifications of Aphasia PDFDocument1 pageCommon Classifications of Aphasia PDFAhmad HasanNo ratings yet
- Pre-Operative & Post-Operative Care PlansDocument4 pagesPre-Operative & Post-Operative Care PlansHal00mNo ratings yet
- MobilityDocument40 pagesMobilityUzzy Lintang SavitriNo ratings yet
- Ectopic PregnancyDocument34 pagesEctopic Pregnancyannu panchalNo ratings yet
- Mass Hysteria: Celebrity & Fan Culture Bart Pacult & Anna ZiemkiewiczDocument12 pagesMass Hysteria: Celebrity & Fan Culture Bart Pacult & Anna ZiemkiewiczBart PacultNo ratings yet
- Antibiotic Optimization in CIAIDocument33 pagesAntibiotic Optimization in CIAIAditya Pradana KNo ratings yet
- Encyclopedia of OphthalmologyDocument1,998 pagesEncyclopedia of OphthalmologySmara100% (3)