You might also like
- Salivary Gland Cancer: From Diagnosis to Tailored TreatmentFrom EverandSalivary Gland Cancer: From Diagnosis to Tailored TreatmentLisa LicitraNo ratings yet
- Breast Cancer Didactics - ManzanoDocument49 pagesBreast Cancer Didactics - ManzanoJoy ManzanoNo ratings yet
- The Molecular Biology of Cancer: A Bridge from Bench to BedsideFrom EverandThe Molecular Biology of Cancer: A Bridge from Bench to BedsideStella PelengarisNo ratings yet
- Breast CancerDocument56 pagesBreast Cancersarguss14No ratings yet
- Malignant Diseases of BreastDocument70 pagesMalignant Diseases of BreastdranjupradhanNo ratings yet
- Breast PathologDocument51 pagesBreast Pathologjusttin779No ratings yet
- Breast CancerDocument6 pagesBreast Cancersarguss14No ratings yet
- Carcinoma Breast GuideDocument8 pagesCarcinoma Breast GuideYeshvi s100% (1)
- #Surgery - DR - Mohamed - Breast Tumors - 2Document53 pages#Surgery - DR - Mohamed - Breast Tumors - 2mariamNo ratings yet
- CarcinomaofbreastDocument71 pagesCarcinomaofbreastAghisha Subeesh100% (1)
- Prognostic Histologic Features of Colorectal CarcinomaDocument18 pagesPrognostic Histologic Features of Colorectal CarcinomaThomas KlebNo ratings yet
- Ovarian Tumours: Epidemiology, Risk Factors, Classification, and ManagementDocument49 pagesOvarian Tumours: Epidemiology, Risk Factors, Classification, and ManagementChoden JamyangNo ratings yet
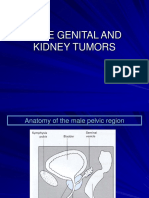
- Male Genital and KidneyDocument69 pagesMale Genital and KidneyPrakasa WicaksonoNo ratings yet
- Breast Cancer (Aka BR CA) : - Routine Screening For Genetic Abnormalities of A Strong Family HX of BR CA Is NOT NeededDocument6 pagesBreast Cancer (Aka BR CA) : - Routine Screening For Genetic Abnormalities of A Strong Family HX of BR CA Is NOT NeededChanthorn SokNo ratings yet
- Pathology of Breast CancerDocument4 pagesPathology of Breast CancerEugene Osei AmoakoNo ratings yet
- Salivaryglandtumors 150912063235 Lva1 App6892Document213 pagesSalivaryglandtumors 150912063235 Lva1 App6892Waqas IqbalNo ratings yet
- Endometrial Cancer: DR P Mukonoweshuro Consultant Pathologist RUH BathDocument59 pagesEndometrial Cancer: DR P Mukonoweshuro Consultant Pathologist RUH BathmesNo ratings yet
- 4th Bimonthly Pathology ReviewerDocument91 pages4th Bimonthly Pathology ReviewerRoselle Louise L. PublicoNo ratings yet
- Cervic Tumour - SummaryDocument9 pagesCervic Tumour - SummaryRUDOLF YUSON BM20110052No ratings yet
- NEOPLASIADocument70 pagesNEOPLASIARose de DiosNo ratings yet
- General AspectsDocument53 pagesGeneral AspectsDhyey PandyaNo ratings yet
- The Breast: Kristoff Armand E. Tan Hannah Lois Kangleon-TanDocument30 pagesThe Breast: Kristoff Armand E. Tan Hannah Lois Kangleon-TanKenneth NuñezNo ratings yet
- Ovary Neoplasm IDocument18 pagesOvary Neoplasm ICatherine JosephNo ratings yet
- 3 Male Genital and KidneyDocument126 pages3 Male Genital and Kidneyindriana sariNo ratings yet
- CACXDocument34 pagesCACXMax ZealNo ratings yet
- Onco Andraine LI-Day-1Document8 pagesOnco Andraine LI-Day-1Errold Joseph LahaganNo ratings yet
- Understanding Neoplasia and TumorsDocument28 pagesUnderstanding Neoplasia and TumorsDaniel SutantoNo ratings yet
- Breast PathologyDocument6 pagesBreast Pathologyanupama menonNo ratings yet
- Current Controversies in The Management of Malignant Parotid TumorsDocument8 pagesCurrent Controversies in The Management of Malignant Parotid TumorsDirga Rasyidin LNo ratings yet
- Appendix Mucinous NeoplasmsDocument122 pagesAppendix Mucinous NeoplasmsBogdan NiculaeNo ratings yet
- Breast Pathology Fumc 2022Document145 pagesBreast Pathology Fumc 2022Bahzad AkramNo ratings yet
- The Breast: AnatomyDocument3 pagesThe Breast: AnatomyRyan James Lorenzo Miguel50% (2)
- Lectura 2Document11 pagesLectura 2CristianNo ratings yet
- Polyps AdvancedDocument5 pagesPolyps AdvancedblablalbablablablaNo ratings yet
- Tumors of Melanocytes Benign: (Mole) Acquired Congenital MalignantDocument73 pagesTumors of Melanocytes Benign: (Mole) Acquired Congenital Malignantlovelyc95No ratings yet
- Spindle Cell Lesions-Romania 2022-5-9-22Document117 pagesSpindle Cell Lesions-Romania 2022-5-9-22Olteanu Dragos-NicolaeNo ratings yet
- Ocular LymphomaDocument67 pagesOcular LymphomaFera Yunita RodhiatyNo ratings yet
- Pancreas: 1. Congenital Anomalies of Pancreas. 2. Pancreatic Cysts. 3. Acute and Chronic Pancreatitis. 4. Pancreatic CancerDocument31 pagesPancreas: 1. Congenital Anomalies of Pancreas. 2. Pancreatic Cysts. 3. Acute and Chronic Pancreatitis. 4. Pancreatic Cancerjwan ahmedNo ratings yet
- Endometrial CarcinomaDocument6 pagesEndometrial CarcinomaĶHwola ƏľsHokryNo ratings yet
- Neoplasia (II) : Department of Pathology, Sun Yat-Sen UniversityDocument138 pagesNeoplasia (II) : Department of Pathology, Sun Yat-Sen UniversityleyreaNo ratings yet
- Etiology, Diagnosis and Staging of TumorsDocument44 pagesEtiology, Diagnosis and Staging of TumorsJeevan SunaNo ratings yet
- Lung Tumour Types and CausesDocument7 pagesLung Tumour Types and CausesNestley TiongsonNo ratings yet
- MALE GENITAL AND KIDNEY TUMOR GUIDEDocument119 pagesMALE GENITAL AND KIDNEY TUMOR GUIDEFaerusNo ratings yet
- Histopathology of Oral Epithelial TumorsDocument44 pagesHistopathology of Oral Epithelial TumorsRanjit DanielNo ratings yet
- Benign Ovarian MassDocument39 pagesBenign Ovarian MassVidhi Chaudhary100% (1)
- Ovarian TumorsDocument19 pagesOvarian TumorsNandita JaliNo ratings yet
- Ovid: Cancer: Principles & Practice of OncologyDocument42 pagesOvid: Cancer: Principles & Practice of Oncology7vhpkwgc6jNo ratings yet
- Breast CancerDocument68 pagesBreast Cancerapi-3748365100% (4)
- Breast Cancer Risk Factors, Diagnosis and ManagementDocument49 pagesBreast Cancer Risk Factors, Diagnosis and ManagementJoy ManzanoNo ratings yet
- Breast Carcinoma EtiopathogenesisDocument22 pagesBreast Carcinoma EtiopathogenesisprinceejNo ratings yet
- Clinical Case CAPDocument82 pagesClinical Case CAPIna GargNo ratings yet
- Diseases of Female Reproductive SystemDocument13 pagesDiseases of Female Reproductive SystemSalon LamichhaneNo ratings yet
- Thyroid Malignancy With MRNDDocument25 pagesThyroid Malignancy With MRNDRashma JosephNo ratings yet
- Female-Genital 2 PDFDocument16 pagesFemale-Genital 2 PDFMuhammad SalmanNo ratings yet
- Epidermal Nevi, Neoplasms, and CystsDocument106 pagesEpidermal Nevi, Neoplasms, and CystsmesNo ratings yet
- Neoplasia 2Document57 pagesNeoplasia 2Dyvanal ArifinNo ratings yet
- Endometrial Carcinoma - ClinicalKeyDocument25 pagesEndometrial Carcinoma - ClinicalKeyValentina Grajales RestrepoNo ratings yet
- Singapore SalivaryDocument149 pagesSingapore Salivaryna huNo ratings yet
- 1 - Cervical CancerDocument87 pages1 - Cervical Cancerzuzuyasi65No ratings yet
- NeoplasiaDocument70 pagesNeoplasiaNestly QuerubinNo ratings yet
- Intestinal Obstruction Causes and TreatmentDocument56 pagesIntestinal Obstruction Causes and Treatmentjayvee digitalNo ratings yet
- Laparotomi Pada TraumaDocument10 pagesLaparotomi Pada TraumaIntan Eklesiana NapitupuluNo ratings yet
- PR To Hernia Angkatan 1bDocument3 pagesPR To Hernia Angkatan 1bIntan Eklesiana NapitupuluNo ratings yet
- Fisa de Observatie EndocrinologieDocument25 pagesFisa de Observatie EndocrinologieMarina DomencoNo ratings yet
- CPC 06 2003Document38 pagesCPC 06 2003Intan Eklesiana NapitupuluNo ratings yet
- Anticoagulan DrugsDocument35 pagesAnticoagulan Drugsintan_ekleNo ratings yet
- Critical Appraisal of The TopicsDocument11 pagesCritical Appraisal of The TopicsIntan Eklesiana NapitupuluNo ratings yet
- Name Tag Instruktur ATLS Desember 2017 (1) NEWDocument12 pagesName Tag Instruktur ATLS Desember 2017 (1) NEWIntan Eklesiana NapitupuluNo ratings yet
- Knot TyingDocument28 pagesKnot TyingIntan Eklesiana NapitupuluNo ratings yet
- FastDocument10 pagesFastAnonymous Lxho3INo ratings yet
- English Setences With ExamplesDocument20 pagesEnglish Setences With ExamplesphaywaNo ratings yet
- Medical Retrieval and Transfer-Pre and Post TesDocument13 pagesMedical Retrieval and Transfer-Pre and Post TesIntan Eklesiana NapitupuluNo ratings yet
- Critical Appraisal of The TopicsDocument13 pagesCritical Appraisal of The TopicsIntan Eklesiana NapitupuluNo ratings yet
- Daftar Pustaka To Hernia Lateralis Inguinalis - AgistiaDocument1 pageDaftar Pustaka To Hernia Lateralis Inguinalis - AgistiaIntan Eklesiana NapitupuluNo ratings yet
- Daftar Kode ICD 10 dan ICD 9 paling sering Kasus BedahDocument16 pagesDaftar Kode ICD 10 dan ICD 9 paling sering Kasus BedahIntan Eklesiana NapitupuluNo ratings yet
- Jti 30 091Document7 pagesJti 30 091Intan Eklesiana NapitupuluNo ratings yet
- OrthoDocument41 pagesOrthodoos1No ratings yet
- Cat Jurnal Pediatric - IntanDocument11 pagesCat Jurnal Pediatric - IntanIntan Eklesiana NapitupuluNo ratings yet
- Daftar Kode ICD 10 dan ICD 9 paling sering Kasus BedahDocument16 pagesDaftar Kode ICD 10 dan ICD 9 paling sering Kasus BedahIntan Eklesiana NapitupuluNo ratings yet
- Instructions For The Preparation of A Final ManuscriptDocument3 pagesInstructions For The Preparation of A Final ManuscriptIntan Eklesiana NapitupuluNo ratings yet
- Food StallDocument1 pageFood StallIntan Eklesiana NapitupuluNo ratings yet
- Medical Retrieval and Transfer-Pre and Post TesDocument13 pagesMedical Retrieval and Transfer-Pre and Post TesIntan Eklesiana NapitupuluNo ratings yet
- Trauma ThoraxDocument23 pagesTrauma ThoraxIntan Eklesiana NapitupuluNo ratings yet
- HBP + Large IntestineDocument54 pagesHBP + Large IntestineIntan Eklesiana NapitupuluNo ratings yet
- Daftar Kode ICD 10 dan ICD 9 paling sering Kasus BedahDocument16 pagesDaftar Kode ICD 10 dan ICD 9 paling sering Kasus BedahIntan Eklesiana NapitupuluNo ratings yet
- The Relationship Between Ethics, Values, Moral, Religion, Etiquette, Law, & Code of ConductDocument12 pagesThe Relationship Between Ethics, Values, Moral, Religion, Etiquette, Law, & Code of ConductIntan Eklesiana NapitupuluNo ratings yet
- WJGS 9 153Document9 pagesWJGS 9 153Intan Eklesiana NapitupuluNo ratings yet
- Daftar Kode ICD 10 dan ICD 9 paling sering Kasus BedahDocument16 pagesDaftar Kode ICD 10 dan ICD 9 paling sering Kasus BedahIntan Eklesiana NapitupuluNo ratings yet
- Count Head BleedingDocument7 pagesCount Head BleedingIntan Eklesiana NapitupuluNo ratings yet
- Critical View of SafetyDocument4 pagesCritical View of SafetyIntan Eklesiana NapitupuluNo ratings yet
- Early Diabetic Risk Prediction Using Machine Learning Classification TechniquesDocument6 pagesEarly Diabetic Risk Prediction Using Machine Learning Classification TechniquesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Visualization BenchmarkingDocument15 pagesVisualization BenchmarkingRanjith S100% (1)
- Document-SAP EWM For Fashion 1.0: 1.general IntroductionDocument3 pagesDocument-SAP EWM For Fashion 1.0: 1.general IntroductionAnonymous u3PhTjWZRNo ratings yet
- Copy Resit APLC MiniAssignmentDocument5 pagesCopy Resit APLC MiniAssignmentChong yaoNo ratings yet
- A ULTIMA ReleaseNotesAxiomV PDFDocument38 pagesA ULTIMA ReleaseNotesAxiomV PDFIVANALTAMARNo ratings yet
- Chanel SWOT AnalysisDocument5 pagesChanel SWOT AnalysisJeish KimNo ratings yet
- Lean Management AssignmentDocument14 pagesLean Management AssignmentElorm Oben-Torkornoo100% (1)
- Structural IfpDocument4 pagesStructural IfpDanny NguyenNo ratings yet
- Pharma TestDocument2 pagesPharma TestMuhammad AdilNo ratings yet
- Ketchikan Shipyard Improvements Plan CompleteDocument230 pagesKetchikan Shipyard Improvements Plan CompleteOpó Ishak Bawias Adare100% (1)
- An Introduction To Liturgy of The Catholic ChurchDocument27 pagesAn Introduction To Liturgy of The Catholic ChurchElsha DamoloNo ratings yet
- WEEK 8. - Gen Math-PortfolioDocument12 pagesWEEK 8. - Gen Math-PortfolioOreo ProductionsNo ratings yet
- K230F Equipment ManualsDocument166 pagesK230F Equipment ManualsHui ChenNo ratings yet
- Organic Chem Diels-Alder Reaction LabDocument9 pagesOrganic Chem Diels-Alder Reaction LabPryanka BalleyNo ratings yet
- Analysis and Design of Multi Storey Building by Using STAAD ProDocument5 pagesAnalysis and Design of Multi Storey Building by Using STAAD Prolikith rockNo ratings yet
- 2010 HSC Exam PhysicsDocument42 pages2010 HSC Exam PhysicsVictor345No ratings yet
- mcs2019 All PDFDocument204 pagesmcs2019 All PDFRheydel BartolomeNo ratings yet
- Apps Tables Excel FRMTDocument4 pagesApps Tables Excel FRMTSunil ReddyNo ratings yet
- 2 5 Marking ScheduleDocument6 pages2 5 Marking Scheduleapi-218511741No ratings yet
- Political Engineering and Party Politics in Conflict-Prone SocietiesDocument18 pagesPolitical Engineering and Party Politics in Conflict-Prone SocietiesNashiba Dida-AgunNo ratings yet
- Smoktech Vmax User ManualDocument9 pagesSmoktech Vmax User ManualStella PapaNo ratings yet
- Act 1&2 and SAQ No - LawDocument4 pagesAct 1&2 and SAQ No - LawBududut BurnikNo ratings yet
- Week 1 Gec 106Document16 pagesWeek 1 Gec 106Junjie FuentesNo ratings yet
- A Summer Internship Project ON " To Study The Supply Chain Management On Amul Fresh Products" AT GCMMF, AmulDocument19 pagesA Summer Internship Project ON " To Study The Supply Chain Management On Amul Fresh Products" AT GCMMF, AmulweetrydhNo ratings yet
- Integrating Therapeutic Play Into Nursing and Allied Health PracticeDocument214 pagesIntegrating Therapeutic Play Into Nursing and Allied Health PracticeIbrahim SabraNo ratings yet
- POPULARITY OF CREDIT CARDS ISSUED BY DIFFERENT BANKSDocument25 pagesPOPULARITY OF CREDIT CARDS ISSUED BY DIFFERENT BANKSNaveed Karim Baksh75% (8)
- ChromosomesDocument24 pagesChromosomesapi-249102379No ratings yet
- GVB 1Document8 pagesGVB 1Aaron SylvestreNo ratings yet
- Guillermo Estrella TolentinoDocument15 pagesGuillermo Estrella TolentinoJessale JoieNo ratings yet
- ??????? ?? ??????Document29 pages??????? ?? ??????Aysha ShahabNo ratings yet