You might also like
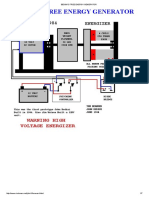
- Bedini's Free Energy Generator PDFDocument7 pagesBedini's Free Energy Generator PDFRafly Attila Al-Fiqri71% (7)
- The Basics of General, Organic and Biological Chemistry - AttributedDocument1,421 pagesThe Basics of General, Organic and Biological Chemistry - AttributedAlfonso J Sintjago100% (2)
- CH 10 Circular Motion Exercises AnswersDocument4 pagesCH 10 Circular Motion Exercises AnswersMuhammad Aslam0% (1)
- Fusion of Modern and Ancient: Feldspathic/refractory Veneers Using Zirconia PorcelainDocument7 pagesFusion of Modern and Ancient: Feldspathic/refractory Veneers Using Zirconia PorcelaintarekrabiNo ratings yet
- Black Pigmentation in Primary Dentition Case Report and Literature ReviewDocument5 pagesBlack Pigmentation in Primary Dentition Case Report and Literature ReviewlaloNo ratings yet
- Common Icd-10 Dental Codes: ICD-10 DESCRIPTOR FROM WHO (Complete)Document15 pagesCommon Icd-10 Dental Codes: ICD-10 DESCRIPTOR FROM WHO (Complete)Wulan OktavianiNo ratings yet
- Radar PlottingDocument23 pagesRadar Plottingthugsdei100% (2)
- ZirconiaDocument12 pagesZirconiaAna Massiel NarváezNo ratings yet
- A Review of Dental CAD/CAM: Current Status and Future Perspectives From 20 Years of ExperienceDocument13 pagesA Review of Dental CAD/CAM: Current Status and Future Perspectives From 20 Years of ExperienceRuiFiaoNo ratings yet
- All Ceramic Crown Restoration GuideDocument50 pagesAll Ceramic Crown Restoration GuideBishoy MaherNo ratings yet
- CAD/CAM Dental Technology Creates Crowns in One VisitDocument61 pagesCAD/CAM Dental Technology Creates Crowns in One VisitAnnaAffandieNo ratings yet
- CAD/CAM Dental Restorations ReviewedDocument7 pagesCAD/CAM Dental Restorations ReviewedLjubomirErdoglijaNo ratings yet
- Cor Tec Cor Tec: Applications and Functions For Coritec Machine SystemsDocument23 pagesCor Tec Cor Tec: Applications and Functions For Coritec Machine SystemsOzNo ratings yet
- Materiale Ceramice in StomatologieDocument23 pagesMateriale Ceramice in StomatologieMogos PaulNo ratings yet
- Sample Odontogram Description of Charting SymbolsDocument1 pageSample Odontogram Description of Charting Symbols085242486606No ratings yet
- Dental Ceramics For Restoration and Metal VeneeringDocument23 pagesDental Ceramics For Restoration and Metal VeneeringMichael XuNo ratings yet
- Retrograde PreparationDocument16 pagesRetrograde Preparationwhussien7376100% (1)
- Fabrication of Provisional Crowns and BridgesDocument22 pagesFabrication of Provisional Crowns and BridgesAdam PhillipsNo ratings yet
- Fracture Resistance and Marginal Discrepancy of Porcelain Laminate Veneers Influenced by Preparation Design and Restorative Material in Vitro PDFDocument8 pagesFracture Resistance and Marginal Discrepancy of Porcelain Laminate Veneers Influenced by Preparation Design and Restorative Material in Vitro PDFLuis Alberto Carpio MorenoNo ratings yet
- Metal Ceramic Crown Has Always Been The Most Popular Complete Veneer Restoration in DentistryDocument3 pagesMetal Ceramic Crown Has Always Been The Most Popular Complete Veneer Restoration in DentistryFlorian LitaNo ratings yet
- Method of Vital Extirpation PDFDocument23 pagesMethod of Vital Extirpation PDFShany SchwarzwaldNo ratings yet
- 2.-Tecnica Step BackDocument4 pages2.-Tecnica Step BackSamirNo ratings yet
- Fundamentals of Tooth Preparation PDFDocument74 pagesFundamentals of Tooth Preparation PDFAyesha AwanNo ratings yet
- RO0111 00-00 WebberDocument6 pagesRO0111 00-00 WebberARTNo ratings yet
- Titanium Framework Removable Partial Denture Used ForDocument4 pagesTitanium Framework Removable Partial Denture Used ForManjeev GuragainNo ratings yet
- 1proteza Partiala Mobilizabila, Nevoia Clinica de Inovare 2017 Journal of Prosthetic DentistryDocument8 pages1proteza Partiala Mobilizabila, Nevoia Clinica de Inovare 2017 Journal of Prosthetic DentistrydanielaNo ratings yet
- Causes and prevention of ledging and blockages in root canalsDocument19 pagesCauses and prevention of ledging and blockages in root canalsBunga Erlita RosaliaNo ratings yet
- TOV Implant CATALOG 2021 - IH CHDocument32 pagesTOV Implant CATALOG 2021 - IH CHPolitanouNo ratings yet
- The Next Generation of Zirconia in Dentistry: Ce EbookDocument9 pagesThe Next Generation of Zirconia in Dentistry: Ce EbookLuciano JesusNo ratings yet
- Restorative Technique Selection in Class IV Direct Composite RestorationsDocument6 pagesRestorative Technique Selection in Class IV Direct Composite RestorationsCalisto GomesNo ratings yet
- Apex LocatorsDocument19 pagesApex LocatorsChandra Dhar DwivediNo ratings yet
- ISO MethodDocument3 pagesISO MethodMuhammad GhufronNo ratings yet
- Ceramics in Dental RestorationsDocument11 pagesCeramics in Dental RestorationsDaniel CostinNo ratings yet
- The Circumferential Splint Reinvented: A Long-Term Treatment for Periodontally Compromised Anterior TeethDocument13 pagesThe Circumferential Splint Reinvented: A Long-Term Treatment for Periodontally Compromised Anterior TeethPaulNo ratings yet
- Periodontal Treatment Planning for Patients With Periodontal DiseasesDocument17 pagesPeriodontal Treatment Planning for Patients With Periodontal Diseasesفاطمة فالح ضايف مزعلNo ratings yet
- Soldering in RPDDocument4 pagesSoldering in RPDPraveen KumarNo ratings yet
- A Comparison of The Index of Complexity Outcome and Need (ICON) With The Peer Assessment Rating (PAR) and The Index of Orthodontic Treatment Need (IOTN)Document6 pagesA Comparison of The Index of Complexity Outcome and Need (ICON) With The Peer Assessment Rating (PAR) and The Index of Orthodontic Treatment Need (IOTN)Pattrisha RaeNo ratings yet
- Removable Complete DentureDocument59 pagesRemovable Complete DentureMuhammadFadliNo ratings yet
- Porcelain Fused To Metal CrownDocument11 pagesPorcelain Fused To Metal Crownabdullah aliNo ratings yet
- Retreatment in Persistent Apical PeriodontitisDocument169 pagesRetreatment in Persistent Apical PeriodontitisAnciya NazarNo ratings yet
- II - Alternative Technique To Conventional Casting For Construction of Metal Substructure in Metal - Ceramic Restorations.-1Document8 pagesII - Alternative Technique To Conventional Casting For Construction of Metal Substructure in Metal - Ceramic Restorations.-1Ahmed Yahya83% (6)
- Kanker MulutDocument2 pagesKanker MulutHamba AllahNo ratings yet
- Porcelain Fused To Metal CrownsDocument5 pagesPorcelain Fused To Metal CrownsCitra Dwi PrastiwieNo ratings yet
- Porcelain Fused To Metal CrownDocument17 pagesPorcelain Fused To Metal CrownAhmad SalehNo ratings yet
- A Randomised Clinical Study of The Effect of A Denture Soft Liner On Mandibular Ridge ResorptionDocument6 pagesA Randomised Clinical Study of The Effect of A Denture Soft Liner On Mandibular Ridge ResorptionIJRASETPublicationsNo ratings yet
- Oral Rehabilitation With Removable Partial Dentures in Advanced Tooth Loss SituationsDocument7 pagesOral Rehabilitation With Removable Partial Dentures in Advanced Tooth Loss SituationsIoana-NicoletaNicodimNo ratings yet
- Comparative Evaluation of The Mechanical Properties of Three Commercially Available Flexible Denture Base Materials - An in Vitro StudyDocument132 pagesComparative Evaluation of The Mechanical Properties of Three Commercially Available Flexible Denture Base Materials - An in Vitro StudySkAliHassanNo ratings yet
- All You Need to Know About Zirconium Dental ImplantsDocument5 pagesAll You Need to Know About Zirconium Dental ImplantsCostin VasilescuNo ratings yet
- Principles of EndodonticsDocument40 pagesPrinciples of EndodonticsRaj Joy0% (1)
- Clinical Features of Healthy Periodontal TissueDocument46 pagesClinical Features of Healthy Periodontal TissueNaviatul UlfaNo ratings yet
- Conservative Endodontics Textbooks PDFDocument1 pageConservative Endodontics Textbooks PDFVenkatesh Gavini0% (1)
- Jurnal RKG Kelompok 2Document9 pagesJurnal RKG Kelompok 2hayiarNo ratings yet
- VDW Dental Reciproc User Brochure enDocument32 pagesVDW Dental Reciproc User Brochure enAlvaro Alarcon Valenzuela67% (3)
- Access Cavity PreparationDocument18 pagesAccess Cavity PreparationEthanNo ratings yet
- Working Width 2 PDFDocument4 pagesWorking Width 2 PDFVinayak SinghNo ratings yet
- Cad CamDocument5 pagesCad CamsauriuaNo ratings yet
- RD placement armamentarium guideDocument4 pagesRD placement armamentarium guideSuresh Ferdaus Isa0% (1)
- Research and Reviews: Journal of Material Sciences: Zirconia: Creating A New Perspective To DentistryDocument3 pagesResearch and Reviews: Journal of Material Sciences: Zirconia: Creating A New Perspective To Dentistrysri afriyanti muntheNo ratings yet
- Influence of PreliminaryDocument8 pagesInfluence of PreliminaryOana MateiNo ratings yet
- Materials 05 01348Document13 pagesMaterials 05 01348Mike LiebermannNo ratings yet
- Use of Zirconia in Dentistry: An OverviewDocument9 pagesUse of Zirconia in Dentistry: An OverviewAhmed A. Madfa100% (1)
- Novel Innovations in Dental Implant Biomaterials Science: Zirconia and PEEK PolymersDocument5 pagesNovel Innovations in Dental Implant Biomaterials Science: Zirconia and PEEK PolymersSatya AsatyaNo ratings yet
- Application and Success Rates of Zirconia - A ReviewDocument9 pagesApplication and Success Rates of Zirconia - A ReviewIJAR JOURNALNo ratings yet
- Tugas EkonometrikaDocument8 pagesTugas EkonometrikaaliNo ratings yet
- Dampak Covid-19 Terhadap Perekonomian Masyarakat Dan Pembangunan DesaDocument11 pagesDampak Covid-19 Terhadap Perekonomian Masyarakat Dan Pembangunan DesaaliNo ratings yet
- A Review On Literature of Islamic Charities Between 2008-2018Document18 pagesA Review On Literature of Islamic Charities Between 2008-2018aliNo ratings yet
- Tabel IcastDocument1 pageTabel IcastaliNo ratings yet
- ENGGPHYSDocument13 pagesENGGPHYSUploader101No ratings yet
- Composite Beams & Columns To Eurocode 4Document155 pagesComposite Beams & Columns To Eurocode 4dfdfdfasd324sad100% (2)
- ATS - Design Manual CaterpillarDocument84 pagesATS - Design Manual CaterpillarSharik Khan100% (1)
- Numerical Programming I (For CSE) : Final ExamDocument7 pagesNumerical Programming I (For CSE) : Final ExamhisuinNo ratings yet
- Tutorial Chapter 1 2018Document3 pagesTutorial Chapter 1 2018Ain Syahira0% (1)
- Interference PatternsDocument8 pagesInterference PatternsAsa mathewNo ratings yet
- Hamilton-Jacobi-Bellman Equation ExplainedDocument7 pagesHamilton-Jacobi-Bellman Equation ExplainedMakinita CerveraNo ratings yet
- Theory of Chemical Kinetics and Charge Transfer Based On Nonequilibrium ThermodynamicsDocument17 pagesTheory of Chemical Kinetics and Charge Transfer Based On Nonequilibrium ThermodynamicsYoana Yoa YoaNo ratings yet
- Bearings ShaftsDocument74 pagesBearings ShaftsCik MinnNo ratings yet
- WMM Plant CalibrationDocument5 pagesWMM Plant CalibrationAnonymous zyIPjL9vNo ratings yet
- Maximum Material Boundary (MMB) and Its Advantages in GD&T Analysis PDFDocument6 pagesMaximum Material Boundary (MMB) and Its Advantages in GD&T Analysis PDFSangeethaNo ratings yet
- Introduction to Catalysis LectureDocument22 pagesIntroduction to Catalysis LectureVhyiitrii Shanqk Peñjhaqa Haatii100% (1)
- Flight Equations of Motion for 6 DOF Aircraft ModelDocument24 pagesFlight Equations of Motion for 6 DOF Aircraft ModelNeetu SharmaNo ratings yet
- Elzaki Transform For Two Tank Mixing Problems PDFDocument15 pagesElzaki Transform For Two Tank Mixing Problems PDFMarvin LabajoNo ratings yet
- Skema Chemistry Paper 3Document8 pagesSkema Chemistry Paper 3nurul atiqahNo ratings yet
- Ch15 Differential Momentum BalanceDocument20 pagesCh15 Differential Momentum Balance89kkNo ratings yet
- Principles of CT and CT TechnologyDocument15 pagesPrinciples of CT and CT TechnologyLida Velasquez SierraNo ratings yet
- An Overview of FMCW Systems in MATLABDocument7 pagesAn Overview of FMCW Systems in MATLABHenry TangNo ratings yet
- Book Review Electrochemistry: "Electrolysis". Pot-PourriDocument2 pagesBook Review Electrochemistry: "Electrolysis". Pot-PourriShashank ChandraNo ratings yet
- Mean Deviation - Wolfram MathWorldDocument4 pagesMean Deviation - Wolfram MathWorldbraulio.dantas-1No ratings yet
- Filter Vessel Calculations Per As Me Viii 1Document40 pagesFilter Vessel Calculations Per As Me Viii 1Anonymous J1vjrU2No ratings yet
- Art AnalysisDocument3 pagesArt AnalysisCheeny VelascoNo ratings yet
- Beryllium and Beryllium Compounds: 2005 Wiley-Vch Verlag GMBH & Co. Kgaa, WeinheimDocument28 pagesBeryllium and Beryllium Compounds: 2005 Wiley-Vch Verlag GMBH & Co. Kgaa, WeinheimjaimeNo ratings yet
- Development of Biomass-Based Plastic Resins From Natural Algal PolysaccharidesDocument72 pagesDevelopment of Biomass-Based Plastic Resins From Natural Algal Polysaccharidesjustin_domingo_2100% (2)
- Tutorial 16 - CEL - BottleDocument14 pagesTutorial 16 - CEL - BottleRezaNo ratings yet
- 53 TOP Structural Analysis - Civil Engineering Multiple Choice Questions AnDocument7 pages53 TOP Structural Analysis - Civil Engineering Multiple Choice Questions AnJohn Aries Almelor Sarza100% (1)