You might also like
- Lecture 5 TAG Metabolism + Adipose + Fatty LiverDocument38 pagesLecture 5 TAG Metabolism + Adipose + Fatty Livernironkushbhuyan2002No ratings yet
- Integration of Metabolism 2019Document68 pagesIntegration of Metabolism 2019Cahyani Tiara Safitri100% (1)
- Study 2 - ComprehensiveDocument47 pagesStudy 2 - ComprehensivepeytonNo ratings yet
- Biochemistry Notes 2Document903 pagesBiochemistry Notes 2madhu PriyaNo ratings yet
- (ENDOCRINE) Tugas Biochemistry Week 2 Jeremy Evans Darmawan 01071180101Document4 pages(ENDOCRINE) Tugas Biochemistry Week 2 Jeremy Evans Darmawan 01071180101Jeremy EvansNo ratings yet
- Bch242-Bch252 2021 CarbohydrateDocument31 pagesBch242-Bch252 2021 CarbohydrateEmmanuella OffiongNo ratings yet
- TAG BiosynthesisDocument4 pagesTAG Biosynthesishassanainshahi13No ratings yet
- Energy Metabolism1Document8 pagesEnergy Metabolism1edimulyanaNo ratings yet
- Chapter 2 - Metabolism & Bioenergetics (Part 2) PDFDocument69 pagesChapter 2 - Metabolism & Bioenergetics (Part 2) PDFdarren100% (2)
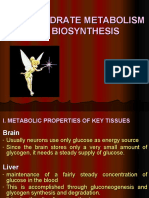
- Carbohydrate Metabolism and BiosynthesisDocument44 pagesCarbohydrate Metabolism and BiosynthesisEmman RegondolaNo ratings yet
- Pink Illustrative Cute Brainstorm PresentationDocument62 pagesPink Illustrative Cute Brainstorm PresentationAlexia Mary Solei BacolodNo ratings yet
- Lipid Metabolism Dental and PhysiotherapyDocument43 pagesLipid Metabolism Dental and PhysiotherapyNada Atef KoraitemNo ratings yet
- Glycolysis For NursesDocument17 pagesGlycolysis For NursesAaron WallaceNo ratings yet
- Bio Chem LMRP 2019Document36 pagesBio Chem LMRP 2019skNo ratings yet
- Glycolysis 1Document33 pagesGlycolysis 1AhmedA.SharafNo ratings yet
- Kuliah Biokimia Blok 2.4.1Document44 pagesKuliah Biokimia Blok 2.4.1Prajna PNo ratings yet
- Biochemistry: Proteins and Amino AcidsDocument8 pagesBiochemistry: Proteins and Amino AcidsrajanOrajanNo ratings yet
- Gluconeogenesis 2Document2 pagesGluconeogenesis 2Nikhitha NunnaNo ratings yet
- GluconeogenesisDocument3 pagesGluconeogenesisClairyssa Myn D CaballeroNo ratings yet
- Biochemistry Notes For BoardsDocument35 pagesBiochemistry Notes For BoardsUjjwal PyakurelNo ratings yet
- Overview of The Major Metabolic PathwaysDocument6 pagesOverview of The Major Metabolic Pathwayssmilechance80% (1)
- Recitation - Metabolic Fate of Glucose and Fatty AcidsDocument2 pagesRecitation - Metabolic Fate of Glucose and Fatty AcidshoythereNo ratings yet
- METABOLISM of CARBOHYDRATESDocument62 pagesMETABOLISM of CARBOHYDRATESmohaysin pirinoNo ratings yet
- Case 1Document10 pagesCase 1DevianaNo ratings yet
- Glucose John SantangeloDocument45 pagesGlucose John Santangelosaint5470No ratings yet
- Carbohydrates Part 2 - MetabolismsDocument60 pagesCarbohydrates Part 2 - MetabolismsNikka Mia AbadiesNo ratings yet
- Glycolysis: Location of GluconeogenesisDocument31 pagesGlycolysis: Location of GluconeogenesisTahera AhmedNo ratings yet
- GlycolysisDocument43 pagesGlycolysisAshish KumarNo ratings yet
- Location of GluconeogenesisDocument4 pagesLocation of GluconeogenesisAhsan AliNo ratings yet
- Gluconeogenesis and Cori CycleDocument21 pagesGluconeogenesis and Cori CycleAboubakar Moalim Mahad moh'dNo ratings yet
- Carbohydrate Metabolism - AnggelDocument32 pagesCarbohydrate Metabolism - Anggeldrnewton03No ratings yet
- Lecture 03. Carbohydrate Metabolism. Common Pathway, Regulation and PathologyDocument80 pagesLecture 03. Carbohydrate Metabolism. Common Pathway, Regulation and PathologyВіталій Михайлович НечипорукNo ratings yet
- BCHEM 254 Metabolism of Nutrients II-Lecture 1 20180121-1Document140 pagesBCHEM 254 Metabolism of Nutrients II-Lecture 1 20180121-1Nicholas BoampongNo ratings yet
- Sugar MetabolismDocument113 pagesSugar MetabolismmismaelNo ratings yet
- Aliaappp Id enDocument20 pagesAliaappp Id enAlia PutriNo ratings yet
- Glycolysis 3MDDocument48 pagesGlycolysis 3MDgostrider0093sNo ratings yet
- 13 Cau Hoa SinhDocument37 pages13 Cau Hoa SinhTran Danh NhanNo ratings yet
- Jurnal KedokteranDocument29 pagesJurnal KedokteranRatna ChairunnisaNo ratings yet
- Overview of MetabolismDocument10 pagesOverview of MetabolismKimberlee Ced NoolNo ratings yet
- Terms For A Medical Student:: 1. GlycolysisDocument24 pagesTerms For A Medical Student:: 1. Glycolysischarmin_limNo ratings yet
- Glycolysis MergedDocument15 pagesGlycolysis MergedNikhitha NunnaNo ratings yet
- Metab Lemak ExtendedDocument50 pagesMetab Lemak ExtendedAlfiyatur rohmaniahNo ratings yet
- Integration of Metabolism: Dr. Farzana Hakim Assistant Professor Biochemistry DepartmentDocument63 pagesIntegration of Metabolism: Dr. Farzana Hakim Assistant Professor Biochemistry DepartmentGriffinNo ratings yet
- Week 9 10. MetabolismDocument37 pagesWeek 9 10. MetabolismKatherine bundalianNo ratings yet
- GlycolysisDocument62 pagesGlycolysisafuaserwaa489No ratings yet
- GluconeogenesisDocument48 pagesGluconeogenesisQshyanNo ratings yet
- Carbohydrate Metabolism b-170810140942 PDFDocument119 pagesCarbohydrate Metabolism b-170810140942 PDFsimasNo ratings yet
- Physiotherapy (Post.) Lipid Metabolism DR - Amal BadrDocument35 pagesPhysiotherapy (Post.) Lipid Metabolism DR - Amal BadrthestaffforpediatricptNo ratings yet
- Metabolism IntegrationDocument10 pagesMetabolism IntegrationValine Cysteine MethionineNo ratings yet
- LIPOGENESISDocument6 pagesLIPOGENESISMUTHONI IRERINo ratings yet
- Chapter 5 Glucose HomeostasisDocument15 pagesChapter 5 Glucose Homeostasistliviu334066No ratings yet
- HW - Carbohydrate Metabolism II & Lipid MetabolismDocument2 pagesHW - Carbohydrate Metabolism II & Lipid MetabolismyanNo ratings yet
- B314 AssignmentDocument23 pagesB314 AssignmentPalesa NtsekalleNo ratings yet
- Checklist: A. B. C. D. eDocument18 pagesChecklist: A. B. C. D. eHoanNo ratings yet
- Fed Fast CycleDocument7 pagesFed Fast CycleZahra AlaradiNo ratings yet
- Lec Notes - Carbohydrates Metabolism II and Lipid MetabolismDocument12 pagesLec Notes - Carbohydrates Metabolism II and Lipid MetabolismyanNo ratings yet
- Carbohydrate MetabolismDocument30 pagesCarbohydrate MetabolismHafsahNo ratings yet
- Type 1 DiabetesDocument5 pagesType 1 DiabetesKehoe MathsNo ratings yet
- 2.7 (BIOCHEMISTRY) Gluconeogenesis - Better PicturesDocument12 pages2.7 (BIOCHEMISTRY) Gluconeogenesis - Better Pictureslovelots1234No ratings yet
- (+) Pain and (+) Discharge (-) Pain and (+) Discharge: Red EyeDocument1 page(+) Pain and (+) Discharge (-) Pain and (+) Discharge: Red EyeMariel TagazaNo ratings yet
- TEARING PDF Final PDFDocument1 pageTEARING PDF Final PDFMariel TagazaNo ratings yet
- Bacteriology Bacterial Classification:: Sequencing Produced by The BodyDocument2 pagesBacteriology Bacterial Classification:: Sequencing Produced by The BodyMariel TagazaNo ratings yet
- Heart and Mediastinum NotesDocument2 pagesHeart and Mediastinum NotesMariel TagazaNo ratings yet
- Resolution of (Co (En) As ( (+) - Co (En) : Synthesis and Characterization of Cobalt Complexes (Day 3) Part 1. SynthesisDocument2 pagesResolution of (Co (En) As ( (+) - Co (En) : Synthesis and Characterization of Cobalt Complexes (Day 3) Part 1. SynthesisMariel TagazaNo ratings yet
- Cheat SheetDocument2 pagesCheat SheetMariel TagazaNo ratings yet
- Background of The Experiment Results and DiscussionDocument1 pageBackground of The Experiment Results and DiscussionMariel TagazaNo ratings yet
- Endocrine System NotesDocument8 pagesEndocrine System NotesShiela Mae SagayoNo ratings yet
- Ajcn 138214Document9 pagesAjcn 138214Gustavo AlmeidaNo ratings yet
- Biochemistry MCQsDocument19 pagesBiochemistry MCQsschxzerrydawn100% (1)
- Diabetes: Statistics Symptoms Causes Diagnosis PreventionDocument67 pagesDiabetes: Statistics Symptoms Causes Diagnosis PreventionShanthi_KVNo ratings yet
- Homeostasis in The Human BodyDocument6 pagesHomeostasis in The Human BodyfakhirNo ratings yet
- Biochemistry Basic Science MCQsDocument26 pagesBiochemistry Basic Science MCQsSidharta Chatterjee50% (2)
- Biochemistry Revalida 2021Document30 pagesBiochemistry Revalida 2021RM DulawanNo ratings yet
- Biokimia Kelompok 5 Revisi (Enzim, Hormon Dan Vitamin)Document50 pagesBiokimia Kelompok 5 Revisi (Enzim, Hormon Dan Vitamin)Uni NadhilaNo ratings yet
- Pancreatic Hormones & Antidiabetic DrugsDocument41 pagesPancreatic Hormones & Antidiabetic DrugsSaddamix AL OmariNo ratings yet
- Module QuestionsDocument11 pagesModule QuestionszulkarnainNo ratings yet
- Diabetes Mellitus in Children (Pedi Clinics of N. America Vol 52, No 6) WW PDFDocument275 pagesDiabetes Mellitus in Children (Pedi Clinics of N. America Vol 52, No 6) WW PDFEliMihaelaNo ratings yet
- Healthy Eating For Type 2 Diabetes: A Harvard Medical School Special Health ReportDocument57 pagesHealthy Eating For Type 2 Diabetes: A Harvard Medical School Special Health ReportCaroline JeeNo ratings yet
- Ch24 ShortAnswer and Essay QuestionsDocument3 pagesCh24 ShortAnswer and Essay Questionsomar83% (6)
- Patho of DM-2, Case PresentationDocument5 pagesPatho of DM-2, Case PresentationLouella Mae CoraldeNo ratings yet
- DKA, HHS, HypoglycemiaDocument63 pagesDKA, HHS, Hypoglycemiacitra dewiNo ratings yet
- PCOL - Diabetes MellitusDocument7 pagesPCOL - Diabetes MellitusTerepe CrimsonNo ratings yet
- HOMEOSTASISDocument24 pagesHOMEOSTASISBasty BERNALESNo ratings yet
- PAP Review KEY - Unit 7 CBA 2016-2017Document5 pagesPAP Review KEY - Unit 7 CBA 2016-2017Tom PunnenNo ratings yet
- New Test - February 14, 2018: MarkschemeDocument28 pagesNew Test - February 14, 2018: MarkschemeRitika GulguliaNo ratings yet
- DnlodDocument43 pagesDnlod312887No ratings yet
- 2.2 Biological Molecules PDFDocument73 pages2.2 Biological Molecules PDFtess_15No ratings yet
- Endocrine System Research TaskDocument4 pagesEndocrine System Research TaskShaheen AliNo ratings yet
- Integration of Metabolism WebDocument72 pagesIntegration of Metabolism WebLini Anisfatus SholihahNo ratings yet
- DB31 - Pathophysiology of Diabetes Mellitus and HypoglycemiaDocument5 pagesDB31 - Pathophysiology of Diabetes Mellitus and HypoglycemiaNeil Alcazaren かわいいNo ratings yet
- Homeostasis, Inflammation, and Disease SusceptibilityDocument12 pagesHomeostasis, Inflammation, and Disease SusceptibilityserodriguezpNo ratings yet
- Ayurveda Book PDFDocument147 pagesAyurveda Book PDFradhaNo ratings yet
- Estado Pos Pran DialDocument10 pagesEstado Pos Pran DialSilvia Melendez LozaNo ratings yet
- Diabetes Mellitus and Pancreatitis - Cause or EffectDocument10 pagesDiabetes Mellitus and Pancreatitis - Cause or EffectRoberto Gutiérrez GonzálezNo ratings yet
- GlycogenesisDocument7 pagesGlycogenesishammad646No ratings yet
- Dental Hygiene Board Exam Sample QuestionsDocument3 pagesDental Hygiene Board Exam Sample Questionsgeislernet100% (5)