You might also like
- Personal ReflectionDocument18 pagesPersonal ReflectionCamela Jane Dela PeñaNo ratings yet
- Personality Development PDFDocument15 pagesPersonality Development PDFblitzkrig100% (12)
- The Balanced Musician EssayDocument2 pagesThe Balanced Musician EssayAlexander DavadillaNo ratings yet
- Stages of Psychosexual Development and Stages of Psychosocial DevelopmentDocument7 pagesStages of Psychosexual Development and Stages of Psychosocial DevelopmentjosedenniolimNo ratings yet
- Assignment of Multiple Choice Questions Psychology)Document17 pagesAssignment of Multiple Choice Questions Psychology)nraghaveNo ratings yet
- Depression PDFDocument16 pagesDepression PDFMakmur SejatiNo ratings yet
- Final Reflection ENC 1101Document2 pagesFinal Reflection ENC 1101MontanaNo ratings yet
- Course ReflectionDocument4 pagesCourse Reflectionapi-316657882No ratings yet
- Personal StatementDocument6 pagesPersonal Statementapi-312642927No ratings yet
- How To Prepare A Research Proposal - Asya Al-RiyamiDocument4 pagesHow To Prepare A Research Proposal - Asya Al-RiyamishemjazNo ratings yet
- Nikola Grahek - Feeling Pain and Being in PainDocument199 pagesNikola Grahek - Feeling Pain and Being in PainАндреа Ковачевић100% (2)
- James New Personal StatementDocument1 pageJames New Personal StatementJames HarrisonNo ratings yet
- Practice Test Questions Downloaded From FILIPINO NURSES CENTRALDocument17 pagesPractice Test Questions Downloaded From FILIPINO NURSES CENTRALFilipino Nurses CentralNo ratings yet
- Career Development Self ReflectionDocument3 pagesCareer Development Self Reflectionapi-492276783No ratings yet
- 2020 Healthy Minds PowerpointDocument112 pages2020 Healthy Minds Powerpointapi-461452779No ratings yet
- Course Reflection FinalDocument9 pagesCourse Reflection Finalapi-285262009No ratings yet
- The Rise (Rare Disease) Selling Framework: Rising Above Traditional Skill Sets. Transformational Rare and Ultra-Rare Disease Therapeutics Demand Transformational Customer InterfacingFrom EverandThe Rise (Rare Disease) Selling Framework: Rising Above Traditional Skill Sets. Transformational Rare and Ultra-Rare Disease Therapeutics Demand Transformational Customer InterfacingNo ratings yet
- Multidisciplinary Team and Pharmacists Role in That TeamDocument5 pagesMultidisciplinary Team and Pharmacists Role in That TeamTimothy OgomaNo ratings yet
- Professionalism Professional Development PlanDocument9 pagesProfessionalism Professional Development PlanPrasiddha ParajuliNo ratings yet
- The Resume Critique The Gentle ArtDocument4 pagesThe Resume Critique The Gentle ArtAndrew SeguelNo ratings yet
- This Study Resource Was: Student Name: Madeline Hammett HAMMD1901Document5 pagesThis Study Resource Was: Student Name: Madeline Hammett HAMMD1901Ambika Suwal100% (1)
- ReflectionDocument3 pagesReflectionapi-238773232No ratings yet
- Educ2181 PP WeeblyDocument4 pagesEduc2181 PP Weeblyapi-363014935No ratings yet
- Assignment 2 - Critical Reflection JournalDocument16 pagesAssignment 2 - Critical Reflection Journalapi-299544727No ratings yet
- Final Evaluation: NURS 3021H Clinical Practice Focused On Chronic Disease ManagementDocument14 pagesFinal Evaluation: NURS 3021H Clinical Practice Focused On Chronic Disease Managementapi-271855323No ratings yet
- Report On Field PlacementDocument6 pagesReport On Field Placementapi-283974130No ratings yet
- Areas For Growth PortfolioDocument8 pagesAreas For Growth Portfolioapi-383463670No ratings yet
- Adlerian Theory and The Case of MargaritaDocument4 pagesAdlerian Theory and The Case of MargaritaEzzah SobliNo ratings yet
- Reflection Paper Kamia Solomon Georgia College and State UniversityDocument7 pagesReflection Paper Kamia Solomon Georgia College and State Universityapi-506846662No ratings yet
- Assessment and Care of Adults at Risk For Suicidal Ideation and BehaviourDocument2 pagesAssessment and Care of Adults at Risk For Suicidal Ideation and Behaviourmpetrov_2No ratings yet
- Portfolio Narrative Area For GrowthDocument8 pagesPortfolio Narrative Area For Growthapi-438194331No ratings yet
- Am A YoungDocument2 pagesAm A YoungPavni JainNo ratings yet
- FesarahDocument8 pagesFesarahapi-271855323No ratings yet
- Theoretical FinalDocument2 pagesTheoretical FinalShain Ciara C. CanopinNo ratings yet
- Supervisor Connected LessonDocument7 pagesSupervisor Connected Lessonapi-298252147No ratings yet
- Self Awareness and LeadershipDocument6 pagesSelf Awareness and LeadershipVikram . PanchalNo ratings yet
- Literature ReviewDocument2 pagesLiterature ReviewMargie BernabeNo ratings yet
- Roy Sed 765 Leadership FrameworkDocument12 pagesRoy Sed 765 Leadership Frameworkapi-5466258060% (1)
- Kannaiah and Shanthi 2015Document9 pagesKannaiah and Shanthi 2015shammu mayrajNo ratings yet
- NS 622 AssignmentDocument16 pagesNS 622 AssignmentGareth McKnightNo ratings yet
- CompetenciesDocument40 pagesCompetenciesapi-433742884No ratings yet
- Workshop - Emotional IntelligenceDocument1 pageWorkshop - Emotional IntelligencemysticblissNo ratings yet
- HRM 320 Sexual Harassment PaperDocument10 pagesHRM 320 Sexual Harassment Paperraahatali_633732570No ratings yet
- CompetenciesDocument40 pagesCompetenciesapi-328744175No ratings yet
- Ahrq 2004 PDFDocument74 pagesAhrq 2004 PDFDelly TunggalNo ratings yet
- My NLN CompetenciesDocument5 pagesMy NLN Competenciesapi-285244567No ratings yet
- Usa & Russia School ComparisonDocument5 pagesUsa & Russia School ComparisonDariaNo ratings yet
- EUO NRSG263 FinalDocument17 pagesEUO NRSG263 FinalJosh TuibeoNo ratings yet
- Competency 2Document40 pagesCompetency 2api-345830847No ratings yet
- Role of HR Policies in Motivating EmployeesDocument6 pagesRole of HR Policies in Motivating EmployeesShivam TiwariNo ratings yet
- Final EssayDocument9 pagesFinal Essayapi-383024083No ratings yet
- Annotated BibliographyDocument6 pagesAnnotated BibliographyAcidicHumanNo ratings yet
- The Dangers of ComplacencyDocument3 pagesThe Dangers of Complacencyegahmulia100% (2)
- Portfolio Reflection-2Document3 pagesPortfolio Reflection-2api-507520601No ratings yet
- Case PresentationDocument22 pagesCase Presentationapi-295014480No ratings yet
- OC Awards (Dec10)Document3 pagesOC Awards (Dec10)olympiacollegeNo ratings yet
- Organ Donation: From Diagnosis To Transplant: ReviewDocument10 pagesOrgan Donation: From Diagnosis To Transplant: ReviewFIA SlotNo ratings yet
- Performance Management and The Employee ExperienceDocument12 pagesPerformance Management and The Employee Experiencepremier writersNo ratings yet
- Sonu Scaria Literature ReviewDocument13 pagesSonu Scaria Literature ReviewAnonymous aUrycuWgyNo ratings yet
- Practicum Learning ContractDocument2 pagesPracticum Learning Contractapi-272845852No ratings yet
- Leadership Final ReflectionDocument2 pagesLeadership Final Reflectionapi-290880850100% (1)
- Research Methods ReflectionDocument2 pagesResearch Methods Reflectionapi-250564112No ratings yet
- Essay - Therapeutic CommunicationDocument5 pagesEssay - Therapeutic CommunicationTimoci NavacokowaleNo ratings yet
- Exploring HomelessnessDocument3 pagesExploring HomelessnessLILABYNo ratings yet
- Personal Change Project 2 ComDocument5 pagesPersonal Change Project 2 Comapi-484659785No ratings yet
- Ana Self AssessmentDocument7 pagesAna Self Assessmentapi-301349934No ratings yet
- Program Graduate Competency ReflectionDocument8 pagesProgram Graduate Competency Reflectionapi-499926602No ratings yet
- Applied Learning PaperDocument6 pagesApplied Learning PaperJam EsNo ratings yet
- Self-Reflection - EportfolioDocument2 pagesSelf-Reflection - Eportfolioapi-254345179100% (1)
- Resume 2Document1 pageResume 2api-436090845No ratings yet
- Deaf Culture Presentation-Brady-Angie-KaylaDocument13 pagesDeaf Culture Presentation-Brady-Angie-Kaylaapi-436090845100% (1)
- Casemapping 7 Analyzing Goals and TX PlansDocument14 pagesCasemapping 7 Analyzing Goals and TX Plansapi-436090845No ratings yet
- CC StrokeDocument13 pagesCC Strokeapi-436090845100% (1)
- Teaching and Learning: Philosophies, Principles and PracticesDocument10 pagesTeaching and Learning: Philosophies, Principles and PracticesGilang NugrahaNo ratings yet
- Brainsci 10 00502 v2Document18 pagesBrainsci 10 00502 v2Serque777No ratings yet
- Possible Sources of Organisational ConflictDocument8 pagesPossible Sources of Organisational ConflictVivi VikashNo ratings yet
- Organisational Behaviour-Jan 2006 To July-2008Document3 pagesOrganisational Behaviour-Jan 2006 To July-2008Raj KamalNo ratings yet
- Uncertainty and Stress Why It Causes Diseases and How It Is Mastered by The BrainDocument25 pagesUncertainty and Stress Why It Causes Diseases and How It Is Mastered by The Brainair benderNo ratings yet
- Apa Itu Terapi BermainDocument19 pagesApa Itu Terapi Bermainjasmiechuee100% (1)
- Vika-Glick Larsen Johnson Branstiter 2005Document7 pagesVika-Glick Larsen Johnson Branstiter 2005kharaldsdottirNo ratings yet
- Int246 PDFDocument1 pageInt246 PDFAJAY KUMAR0% (2)
- PerfectionismDocument87 pagesPerfectionismPaul Jorge TagleNo ratings yet
- Convolutional Neural Network Committees For Handwritten Character ClassificationDocument5 pagesConvolutional Neural Network Committees For Handwritten Character ClassificationMad ManNo ratings yet
- Fruit StroopDocument7 pagesFruit StroopFARHAT HAJERNo ratings yet
- Toma de DecisionesDocument6 pagesToma de DecisionesRocioRojasHernandezNo ratings yet
- 1991 Uhl Et Al (1991)Document4 pages1991 Uhl Et Al (1991)Nidhi AggarwalNo ratings yet
- DLP 3 Q2W1Document2 pagesDLP 3 Q2W1Hazel Kate FloresNo ratings yet
- Physiology of Breathing and Respiratory Control During SleepDocument8 pagesPhysiology of Breathing and Respiratory Control During SleepAchmad Hafidz BaraqbahNo ratings yet
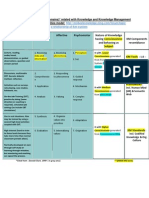
- Bloom's Taxonomy (Learning Domains) Related With Knowledge and Knowledge Management (KM)Document1 pageBloom's Taxonomy (Learning Domains) Related With Knowledge and Knowledge Management (KM)Md SantoNo ratings yet
- Mandolesi Et Al, 2018Document11 pagesMandolesi Et Al, 2018Mateus CarvalhoNo ratings yet
- Chapter 4 Organizations As BrainsDocument13 pagesChapter 4 Organizations As BrainsNamanNo ratings yet
- 3 Language ComprehensionDocument14 pages3 Language ComprehensionZidan Muhammad RausyanNo ratings yet
- Role of An Effective LeaderDocument11 pagesRole of An Effective Leaderdivya kalraNo ratings yet
- Brain-Based-Coaching - CoachingToolkit - ParticipantManualDocument69 pagesBrain-Based-Coaching - CoachingToolkit - ParticipantManualEden PadayacheeNo ratings yet