You might also like
- Ana Nursing StandardsDocument10 pagesAna Nursing StandardsMildred Nurse Ratched BrooksNo ratings yet
- Comprehensive Health Assessment of The Older Person in Health Aged CareDocument2 pagesComprehensive Health Assessment of The Older Person in Health Aged CareMary Cleir CredoNo ratings yet
- Chapter 1 5Document132 pagesChapter 1 5Kylle AlimosaNo ratings yet
- 5 Essential PatDocument4 pages5 Essential PatMichael RotimiNo ratings yet
- SLaM Psychological Medicine CAG - Service User Advisory Group Meeting - October 2013Document1 pageSLaM Psychological Medicine CAG - Service User Advisory Group Meeting - October 2013Bridget Jones100% (1)
- Independent/Advanced Practice NurseDocument25 pagesIndependent/Advanced Practice NurseswethashakiNo ratings yet
- Latihan Soal EpidemiologiDocument3 pagesLatihan Soal EpidemiologisigitNo ratings yet
- CareMore: Innovative Healthcare DeliveryDocument30 pagesCareMore: Innovative Healthcare DeliveryPartnership to Fight Chronic DiseaseNo ratings yet
- What Is The Role of Regulatory Agencies in Continuous Quality ImprovementDocument14 pagesWhat Is The Role of Regulatory Agencies in Continuous Quality ImprovementJana-Tae KerrNo ratings yet
- Program Plan PowerpointDocument15 pagesProgram Plan Powerpointgkempf10No ratings yet
- Guide-Clinical-Preventive-Services 2012Document128 pagesGuide-Clinical-Preventive-Services 2012Gem BorjaNo ratings yet
- NS 01 YohanaDocument16 pagesNS 01 YohanaYohanaAbeysinghe100% (1)
- The Physician AssistantDocument12 pagesThe Physician AssistantThe Physician Assistant LifeNo ratings yet
- Final Group Project Revision VersionDocument16 pagesFinal Group Project Revision Versionapi-217735356No ratings yet
- Terjemahan 1 - 071545Document21 pagesTerjemahan 1 - 071545Merlin NenosonoNo ratings yet
- 5 Ways To Improve The Quality of HealthcareDocument12 pages5 Ways To Improve The Quality of Healthcarekasthu75No ratings yet
- Care Map FinalDocument18 pagesCare Map Finalapi-311540850No ratings yet
- Coursework For Nurse PractitionerDocument5 pagesCoursework For Nurse Practitionerbdg8266a100% (2)
- CareerGuide HCDocument12 pagesCareerGuide HCSasha50% (2)
- Policy BriefDocument8 pagesPolicy Briefapi-341635920No ratings yet
- PCP CC Addendum WebDocument24 pagesPCP CC Addendum WebPatient-Centered Primary Care CollaborativeNo ratings yet
- SLRHDocument48 pagesSLRHDCHS FriendsNo ratings yet
- PDF GettingStarted-AmbulatoryCareDocument27 pagesPDF GettingStarted-AmbulatoryCareChristian SoberonNo ratings yet
- Health Worker Training Evaluation ReportDocument38 pagesHealth Worker Training Evaluation ReportRana Zain Ul AbidinNo ratings yet
- GuideToDischargePlanning PDFDocument32 pagesGuideToDischargePlanning PDFSonyKurniawanNo ratings yet
- Week 5Document28 pagesWeek 5Alvia Magno100% (1)
- What Is Person-Centred Health Care A Literature ReviewDocument4 pagesWhat Is Person-Centred Health Care A Literature ReviewcmppcmwgfNo ratings yet
- Final Program ProposalDocument51 pagesFinal Program Proposalapi-340484697No ratings yet
- Medical Social Worker Course IndiaDocument5 pagesMedical Social Worker Course Indiaafjwdprlzaxewj100% (2)
- Health in Practice ProgrammeDocument6 pagesHealth in Practice Programmeevan mannionNo ratings yet
- The Future of PCMH PDFDocument12 pagesThe Future of PCMH PDFiggybauNo ratings yet
- Psy OutpatientDocument51 pagesPsy Outpatient健康生活園Healthy Life GardenNo ratings yet
- Case Study 2 CHBNDocument3 pagesCase Study 2 CHBNNaomi VirtudazoNo ratings yet
- Group 4 - Team WhatsAppDocument14 pagesGroup 4 - Team WhatsAppSulaiman Abibat DamilolaNo ratings yet
- Sports Health Care Service Manual DraftDocument429 pagesSports Health Care Service Manual DraftYa ChenNo ratings yet
- Wellness Group November 2013 NewsletterDocument4 pagesWellness Group November 2013 Newsletterlilli-pilliNo ratings yet
- Physical Therapy Assistant CourseworkDocument8 pagesPhysical Therapy Assistant Courseworkafazamfbk100% (2)
- Benchmark Nsg-436-Alexis GibsonDocument7 pagesBenchmark Nsg-436-Alexis Gibsonapi-521009603No ratings yet
- Running Head: Evaluating Organizational Change 1Document11 pagesRunning Head: Evaluating Organizational Change 1klm klmNo ratings yet
- Uermmmcigraduate Business PlanDocument4 pagesUermmmcigraduate Business PlanRon OpulenciaNo ratings yet
- Opening An Adult Day CareDocument4 pagesOpening An Adult Day CareKiara Peoples100% (1)
- Community and Public Health NursingDocument13 pagesCommunity and Public Health NursingEzekiel Bunda100% (1)
- Decent Work Employment AND Transcultural Nursing: Noel S. Ayala, MSN, RN, FRINDocument195 pagesDecent Work Employment AND Transcultural Nursing: Noel S. Ayala, MSN, RN, FRINMichtropolisNo ratings yet
- Sample of Job DescriptionsDocument48 pagesSample of Job DescriptionsLoresita Amoranto Rebong RNNo ratings yet
- NEUK 1464 (Revised) 1 (Updated)Document21 pagesNEUK 1464 (Revised) 1 (Updated)Sameen ShafaatNo ratings yet
- Future NursingDocument3 pagesFuture NursingAmelia ArnisNo ratings yet
- The Role of The Gerontological NurseDocument4 pagesThe Role of The Gerontological Nursesusan100% (1)
- Rec 314 Final ProjectDocument17 pagesRec 314 Final Projectapi-254984211No ratings yet
- Cognitive Levels of Long Term Residents Part IIIDocument28 pagesCognitive Levels of Long Term Residents Part IIIapi-339262219No ratings yet
- Running Head: Scope of Practice Is State Regulated 1Document7 pagesRunning Head: Scope of Practice Is State Regulated 1Carole MweuNo ratings yet
- Nurse Practitioner CourseworkDocument4 pagesNurse Practitioner Courseworkitvgpljbf100% (2)
- Research Paper On Licensed Practical NursesDocument4 pagesResearch Paper On Licensed Practical Nursesafnhlmluuaaymj100% (1)
- OrganizationalpaperDocument16 pagesOrganizationalpaperapi-283974130No ratings yet
- Business MemoDocument3 pagesBusiness MemoyourzxtrulyNo ratings yet
- Consumer Centered Mental Health EducationDocument6 pagesConsumer Centered Mental Health EducationfinazkyaloNo ratings yet
- Discussion For Module 7Document3 pagesDiscussion For Module 7Hussain MirzaNo ratings yet
- Fields of Nursing: Ariel M. Ortuoste, RNDocument30 pagesFields of Nursing: Ariel M. Ortuoste, RNortuosteNo ratings yet
- Health Promotion Prevention Plan Presentation (Capter 5)Document42 pagesHealth Promotion Prevention Plan Presentation (Capter 5)MuniraNo ratings yet
- SW 4020 Organizational AnalysisDocument13 pagesSW 4020 Organizational Analysisapi-282542988No ratings yet
- Empowerment Module1Document15 pagesEmpowerment Module1Glenda AstodilloNo ratings yet
- The Implications of The Dodo Bird Verdict For Training in Psychotherapy Prioritizing Process ObservationDocument4 pagesThe Implications of The Dodo Bird Verdict For Training in Psychotherapy Prioritizing Process ObservationSebastian PorcelNo ratings yet
- Diabetes Case Study - Jupyter NotebookDocument10 pagesDiabetes Case Study - Jupyter NotebookAbhising100% (1)
- My Favorite Meal EssayDocument7 pagesMy Favorite Meal Essayb71g37ac100% (2)
- Cambridge Aice Marine Science SyllabusDocument32 pagesCambridge Aice Marine Science Syllabusapi-280088207No ratings yet
- Dual-Attention GAN For Large-Pose Face FrontalizationDocument8 pagesDual-Attention GAN For Large-Pose Face FrontalizationGuillaume Vermeille SanchezNo ratings yet
- Literacy Unit Plan Lesson 4Document2 pagesLiteracy Unit Plan Lesson 4api-212727998No ratings yet
- Vibrant EdutechDocument7 pagesVibrant EdutechGaurav MahorNo ratings yet
- Soc CMM WhitepaperDocument6 pagesSoc CMM WhitepaperJorge D. Zunini C.No ratings yet
- SpringDocument24 pagesSpringRiya IndukuriNo ratings yet
- Principles of Information Technology Syllabus 2015Document4 pagesPrinciples of Information Technology Syllabus 2015api-234035809No ratings yet
- Simulado InglêsDocument3 pagesSimulado InglêsJkBrNo ratings yet
- Effective Teaching Methods and Strategies in The EFL Classroom To Facilitate Students' Vocabulary Development 2020Document29 pagesEffective Teaching Methods and Strategies in The EFL Classroom To Facilitate Students' Vocabulary Development 2020Amara PutriNo ratings yet
- Schoolcity Math q2Document2 pagesSchoolcity Math q2api-297797689No ratings yet
- PepsicoDocument17 pagesPepsicoUsman GhaniNo ratings yet
- Resume Parser Analysis Using Machine Learning and Natural Language ProcessingDocument7 pagesResume Parser Analysis Using Machine Learning and Natural Language ProcessingIJRASETPublicationsNo ratings yet
- Hidden CurriculumDocument11 pagesHidden CurriculumRamakant Patil100% (4)
- Gr5.Mathematics Teachers Guide JPDocument149 pagesGr5.Mathematics Teachers Guide JPRynette FerdinandezNo ratings yet
- ACS Event Report 2Document2 pagesACS Event Report 2Chilamakuri M V TejaNo ratings yet
- Rainbow Bridge 0Document26 pagesRainbow Bridge 0rezalene velez50% (4)
- WMS - IV Flexible Approach Case Study 2: Psychiatric DisorderDocument2 pagesWMS - IV Flexible Approach Case Study 2: Psychiatric DisorderAnaaaerobiosNo ratings yet
- Knowledge Is WealthDocument100 pagesKnowledge Is WealthmustaqNo ratings yet
- Mode of VerificationDocument15 pagesMode of VerificationVincent LibreaNo ratings yet
- Grammar D - Types of Processes in Experiential Meaning (Part 1)Document13 pagesGrammar D - Types of Processes in Experiential Meaning (Part 1)Dena BenNo ratings yet
- Spanish: Pearson Edexcel International GCSE 9-1Document4 pagesSpanish: Pearson Edexcel International GCSE 9-1Sharma DevNo ratings yet
- Web Based Gamo Gofa AgricultureDocument4 pagesWeb Based Gamo Gofa AgricultureAnonymous vNvtJINo ratings yet
- Variables Predictoras de La Lectura y La Escritura en CastellanoDocument14 pagesVariables Predictoras de La Lectura y La Escritura en CastellanoMontserratNo ratings yet
- q2 Lesson 9 Concept PaperDocument4 pagesq2 Lesson 9 Concept PaperShiela May DelacruzNo ratings yet
- Aparri School of Arts and Trades-Senior High School ProgramDocument12 pagesAparri School of Arts and Trades-Senior High School ProgramMyra Jane Pe BenitoNo ratings yet
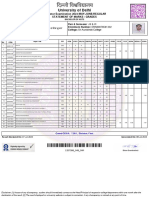
- University of Delhi: Semester Examination 2023-MAY-JUNE:REGULAR Statement of Marks / GradesDocument2 pagesUniversity of Delhi: Semester Examination 2023-MAY-JUNE:REGULAR Statement of Marks / GradesFit CollegeNo ratings yet
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (30)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (4)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (81)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (5)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)
- Empath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainFrom EverandEmpath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainRating: 4 out of 5 stars4/5 (95)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (61)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (60)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesFrom EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesRating: 4.5 out of 5 stars4.5/5 (1412)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (45)