You might also like
- 302 PpJ. Grayson, Freedom From Obsessive Compulsive Disorder A Personalized Recovery Program For LivingDocument2 pages302 PpJ. Grayson, Freedom From Obsessive Compulsive Disorder A Personalized Recovery Program For LivingMohammad Shoyyad L IkhsanNo ratings yet
- Boracay Brochure PDFDocument2 pagesBoracay Brochure PDFmolesag100% (1)
- Peta Kereta Api IndonesiaDocument1 pagePeta Kereta Api Indonesianna_husnaNo ratings yet
- Green Knowledge ActivityDocument12 pagesGreen Knowledge ActivityAgung Nugroho ZainiNo ratings yet
- Chapter 2: Context of The StudyDocument14 pagesChapter 2: Context of The StudyMounir Mc MounirNo ratings yet
- Chapter 2: Context of The StudyDocument14 pagesChapter 2: Context of The StudyMounir Mc MounirNo ratings yet
- The State of Children in Indonesia 2020Document78 pagesThe State of Children in Indonesia 2020firda FibrilaNo ratings yet
- Trans Sumatera RailwayDocument1 pageTrans Sumatera Railwayesun faizNo ratings yet
- Bahan Capaian Ispa KalbarDocument8 pagesBahan Capaian Ispa KalbarEva NurZalinaNo ratings yet
- FCO 348 - Malaysia Travel Advice Ed7Document1 pageFCO 348 - Malaysia Travel Advice Ed7yakiw25996No ratings yet
- Presentasi Rektor USSDocument15 pagesPresentasi Rektor USSkevina adtyNo ratings yet
- Important Class NotesDocument7 pagesImportant Class NotesJatinNo ratings yet
- Bagus Agro Pelaga PresentationDocument20 pagesBagus Agro Pelaga Presentationivon carolineNo ratings yet
- General - Indonesia IndonesiaDocument72 pagesGeneral - Indonesia Indonesiawaleed yehia100% (1)
- OCHA-PHL-MARAWI4 Brgy MapDocument1 pageOCHA-PHL-MARAWI4 Brgy MapDisoma RashidahNo ratings yet
- FGD FinalDocument33 pagesFGD Finalajeng putriNo ratings yet
- FY20FactBookJuly 2021 VFDocument38 pagesFY20FactBookJuly 2021 VFPrateek PandeyNo ratings yet
- Carte 2018-19Document1 pageCarte 2018-19XimeNo ratings yet
- GGGGG: LegendDocument1 pageGGGGG: LegendAkhmad Hata EfendiNo ratings yet
- Indonesia: Map ofDocument5 pagesIndonesia: Map ofLung KinNo ratings yet
- Indonesia: Map ofDocument5 pagesIndonesia: Map ofnasar adenNo ratings yet
- HTLS DDW ACEF 2015 16 June 2015Document19 pagesHTLS DDW ACEF 2015 16 June 2015Sube OhNo ratings yet
- Perak PMR 2016 PDFDocument118 pagesPerak PMR 2016 PDFNURAIN HANIS BINTI ARIFFNo ratings yet
- An Economic Research Project On ASEAN Nations: Brunei DarussalamDocument30 pagesAn Economic Research Project On ASEAN Nations: Brunei DarussalamGerard JuntillaNo ratings yet
- CFP Sesi 1 - Eko Budi KDocument7 pagesCFP Sesi 1 - Eko Budi KNdari SudjiantoNo ratings yet
- Rfi Workshop Presentation PDFDocument47 pagesRfi Workshop Presentation PDFFatan WikramaNo ratings yet
- Draf Report SDocument1 pageDraf Report SfahmiieNo ratings yet
- Indonesia: Map ofDocument5 pagesIndonesia: Map ofAlan FassetNo ratings yet
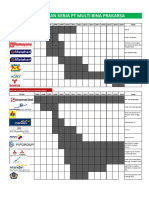
- Pengalam Kerja PT Multi Bina PrakarsaDocument5 pagesPengalam Kerja PT Multi Bina PrakarsaYanuar DwiputrantoNo ratings yet
- Bird Watching in MalaysiaDocument44 pagesBird Watching in MalaysiaEvert De Wolf100% (1)
- B2B Proposal DeckDocument23 pagesB2B Proposal Deckdhika asahimasNo ratings yet
- Beads in Lembah BujangDocument12 pagesBeads in Lembah BujangManjeetNo ratings yet
- Peta Bus BaliDocument1 pagePeta Bus Balimomo.cleo86No ratings yet
- C - 1054 - Aang Dwi Atma Nugraha PDFDocument3 pagesC - 1054 - Aang Dwi Atma Nugraha PDFDens AndrianNo ratings yet
- Pemodelan Sistem Panas Bumi - Ailimaxpem AkamigasDocument9 pagesPemodelan Sistem Panas Bumi - Ailimaxpem AkamigascitraNo ratings yet
- Contoh Transport Planning Tol RoadDocument40 pagesContoh Transport Planning Tol RoadBagus Sukma Putra100% (1)
- Port Development and PendulumDocument47 pagesPort Development and PendulumHerdy Pratama PutraNo ratings yet
- PT. SMART TBK., Padang Halaban Mill: This Is To Certify ThatDocument2 pagesPT. SMART TBK., Padang Halaban Mill: This Is To Certify ThatTai AnjingNo ratings yet
- Corporate Presentation INVESTORDocument15 pagesCorporate Presentation INVESTORHenry So E DiarkoNo ratings yet
- Bab 0 IndexDocument14 pagesBab 0 IndexChing Fu ChooiNo ratings yet
- Malaysia Islands & Beaches 2019-CompressedDocument40 pagesMalaysia Islands & Beaches 2019-CompressedMaria VidalNo ratings yet
- Delivery Service For IKEA Tebrau: Zones Delivery Locations FeesDocument1 pageDelivery Service For IKEA Tebrau: Zones Delivery Locations FeesNurul Nadiah Binti ZulkipliNo ratings yet
- Indonesian Container Port NetworkDocument3 pagesIndonesian Container Port NetworkTania Edna Bhakty SoetjiptoNo ratings yet
- TNB Substation MapDocument1 pageTNB Substation MapWong eZhengNo ratings yet
- Hostel Checklist: Brand New!Document11 pagesHostel Checklist: Brand New!Nikhil JainNo ratings yet
- ISP FiberstarDocument11 pagesISP FiberstarAhmad AfandiNo ratings yet
- EVCuzz Customer Gathering PresentationDocument25 pagesEVCuzz Customer Gathering PresentationMuhamad DimasyqiNo ratings yet
- A Profile of Central VisayasDocument6 pagesA Profile of Central VisayasiamfrancoiseNo ratings yet
- Lahan PadiDocument23 pagesLahan PadiSimon32 TooNo ratings yet
- 2nd Anti-Piracy Patrol in The Gulf of GuineaDocument3 pages2nd Anti-Piracy Patrol in The Gulf of GuineaWhite TigerNo ratings yet
- Brosur Investor KekDocument2 pagesBrosur Investor KekCynthia HerisnayanNo ratings yet
- The Government of Central Java Province Health OfficeDocument50 pagesThe Government of Central Java Province Health OfficeSarma Verawaty SilalahiNo ratings yet
- The Government of Central Java Province Health OfficeDocument50 pagesThe Government of Central Java Province Health OfficeRia Septiyani CloudsYesungNo ratings yet
- The Government of Central Java Province Health OfficeDocument50 pagesThe Government of Central Java Province Health OfficeAbu AzaimarNo ratings yet
- FINAL REPORT - Tanjung Pandan Master Plan+LA - HRDocument177 pagesFINAL REPORT - Tanjung Pandan Master Plan+LA - HRTomy Hastomo ArdhiNo ratings yet
- CorridorAcquisition InformationforInvestor VFDocument12 pagesCorridorAcquisition InformationforInvestor VFAdi HamdanNo ratings yet
- MA004 StormPath 300dpi PDFDocument1 pageMA004 StormPath 300dpi PDFPia QuillopeNo ratings yet
- Psau Scicat RoadmapDocument1 pagePsau Scicat RoadmapPSAU ICTRDNo ratings yet
- ENG DivingDocument20 pagesENG DivingWIRATNA WIRATNANo ratings yet
- Electrocardiography of Arrhythmias A Comprehensive Review A Companion To Cardiac Electrophysiology 2E Mar 8 2021 - 032368050X - Elsevier Mithilesh Kumar Das Full ChapterDocument68 pagesElectrocardiography of Arrhythmias A Comprehensive Review A Companion To Cardiac Electrophysiology 2E Mar 8 2021 - 032368050X - Elsevier Mithilesh Kumar Das Full Chaptermyrtle.leverenz833100% (5)
- Cis Self-Study Lesson Plan: Ophthalmology InstrumentationDocument3 pagesCis Self-Study Lesson Plan: Ophthalmology Instrumentationjerimiah_manzonNo ratings yet
- Resume of Od1206Document3 pagesResume of Od1206api-23436180No ratings yet
- Trauma Thoraks PDFDocument86 pagesTrauma Thoraks PDFMiftahurrahmiNo ratings yet
- A.S.P.E.N. Parenteral Nutrition 2014Document44 pagesA.S.P.E.N. Parenteral Nutrition 2014Debora FroehnerNo ratings yet
- Evaluation of Cyto-Toxic Potential of Aqua Distillate of Rosa Damascena Mill Using Brine Shrimp Lethality AssayDocument4 pagesEvaluation of Cyto-Toxic Potential of Aqua Distillate of Rosa Damascena Mill Using Brine Shrimp Lethality AssayDara Rustri ArdanaNo ratings yet
- William R. Miller and Ernest Kurtz - Models of Alcoholism - 1Document20 pagesWilliam R. Miller and Ernest Kurtz - Models of Alcoholism - 1Carey PickardNo ratings yet
- 16 Severity Scoring and Quality of Life Assessment in Atopic DermatitisDocument16 pages16 Severity Scoring and Quality of Life Assessment in Atopic Dermatitiscgs08No ratings yet
- Vaginal SecretionsDocument33 pagesVaginal SecretionsMatthew BaluyotNo ratings yet
- Xray FilmsDocument13 pagesXray FilmspriyankaagarwallNo ratings yet
- Keep Kicking Ass After 40Document13 pagesKeep Kicking Ass After 40Anonymous OAEuN9NE1sNo ratings yet
- Mollah MD Foysal - MALE - 21 Yrs +918867572813 AHJN.0000204829 2306447Document3 pagesMollah MD Foysal - MALE - 21 Yrs +918867572813 AHJN.0000204829 2306447Adyan FoysalNo ratings yet
- Mindfulness Based Yoga During PregnancyDocument10 pagesMindfulness Based Yoga During PregnancyAdhe AzengNo ratings yet
- Early Vertical CorrectionDocument20 pagesEarly Vertical CorrectionAnirban SarkarNo ratings yet
- (Dianne Watkins MSC PGCE RN RM HV RNT, Judy E (BookFi) PDFDocument368 pages(Dianne Watkins MSC PGCE RN RM HV RNT, Judy E (BookFi) PDFJasmine PradithaNo ratings yet
- Bandaging NewDocument26 pagesBandaging Newmalyn1218100% (7)
- Essentiality CertificateDocument2 pagesEssentiality CertificatePardeep MalikNo ratings yet
- Concor: The Different Beta BlockerDocument23 pagesConcor: The Different Beta BlockerSaud Shirwan100% (1)
- Cara-Imco Physician Catalog PDFDocument408 pagesCara-Imco Physician Catalog PDFmaria jose rodriguez lopezNo ratings yet
- Obstetrics & Gyn II PDF Abnormal PDFDocument305 pagesObstetrics & Gyn II PDF Abnormal PDFmaezu100% (3)
- Tourniquet Application During AnesthesiaDocument7 pagesTourniquet Application During AnesthesiaaksinuNo ratings yet
- All India Institute of Medical Sciences, Bhubaneswar Sijua, Post: Dumuduma, Bhubaneswar - 751 019Document9 pagesAll India Institute of Medical Sciences, Bhubaneswar Sijua, Post: Dumuduma, Bhubaneswar - 751 019mm1979No ratings yet
- 16complete Penokok DietDocument96 pages16complete Penokok DietJAKLIN EMPOLNo ratings yet
- Maternity Waiting HomesDocument2 pagesMaternity Waiting HomesRicky BustosNo ratings yet
- ULG Review Step 1Document34 pagesULG Review Step 1Paul Lexus Gomez LorenzoNo ratings yet
- An Applied Research Project Proposal On INFRASTRUCTURE STIPULATED BY LAW FOR MENTAL HEALTH CARE CENTRESDocument26 pagesAn Applied Research Project Proposal On INFRASTRUCTURE STIPULATED BY LAW FOR MENTAL HEALTH CARE CENTRESShaji Viswanathan. Mcom, MBA (U.K)100% (1)
- Primary Secondary Skin Lesions 2003Document32 pagesPrimary Secondary Skin Lesions 2003Louisa Abigail D'CruzNo ratings yet
- 10th English Practice MCQs KeysDocument4 pages10th English Practice MCQs KeyshamaddijahaNo ratings yet
- Brain InjuryDocument50 pagesBrain InjuryMuhammad Abdul RahmanNo ratings yet