You might also like
- Clinical Approach To CT BrainDocument34 pagesClinical Approach To CT BrainXiaoThoong LohNo ratings yet
- IEE STD C37.104-2002 IEEE Guide For Automatic Reclosing PDFDocument55 pagesIEE STD C37.104-2002 IEEE Guide For Automatic Reclosing PDFJohnatan HernándezNo ratings yet
- Eurocopter EC 135Document205 pagesEurocopter EC 135Varnita Rana100% (6)
- Student Exploration - Radiation (ANSWER KEY)Document3 pagesStudent Exploration - Radiation (ANSWER KEY)Easy Eight0% (5)
- Test Bank For Lehninger Principles of Biochemistry Sixth EditionDocument11 pagesTest Bank For Lehninger Principles of Biochemistry Sixth Editioncosimalocu68xb1No ratings yet
- 4 5947281651888292650 PDFDocument286 pages4 5947281651888292650 PDFicaeeNo ratings yet
- Ball LevitationDocument7 pagesBall LevitationsumlusemloNo ratings yet
- CT of Globe Rupture: Analysis and Frequency of FindingsDocument8 pagesCT of Globe Rupture: Analysis and Frequency of FindingsdrmgroaNo ratings yet
- Excavatum 3Document6 pagesExcavatum 3nadiaNo ratings yet
- Small-Bowel Obstruction From Adhesive Bands and Matted Adhesions: CT DifferentiationDocument5 pagesSmall-Bowel Obstruction From Adhesive Bands and Matted Adhesions: CT DifferentiationOlga DianaNo ratings yet
- Respiratory System - Pulmonary Function TestsDocument2 pagesRespiratory System - Pulmonary Function TestsUnavailable 32No ratings yet
- Recurrence in The Thyroidectomy Bed Sonographic FindingsDocument7 pagesRecurrence in The Thyroidectomy Bed Sonographic Findingspunct_org3256No ratings yet
- Chapter 2 - Med TermDocument21 pagesChapter 2 - Med TermJoy MiascoNo ratings yet
- Uas CT Scan - Jurnal - Dwi Ajeng Risqy Hasanah Syam - P1337430219162 PDFDocument6 pagesUas CT Scan - Jurnal - Dwi Ajeng Risqy Hasanah Syam - P1337430219162 PDFDwi Ajeng Risqy HasanahSyamNo ratings yet
- ISUOG Practice Guidelines - Performance of Firsttrimester Fetal Ultrasound ScanDocument1 pageISUOG Practice Guidelines - Performance of Firsttrimester Fetal Ultrasound ScansandrogvaladzeNo ratings yet
- Congenital Dislocation OF THE HIP AND Computerised: Axial TomographyDocument7 pagesCongenital Dislocation OF THE HIP AND Computerised: Axial Tomographydiablo3 3No ratings yet
- Jurnal CT ScanDocument12 pagesJurnal CT ScanJefri Rudolf WomsiworNo ratings yet
- Aortic DissectionDocument5 pagesAortic DissectionCosminNGDNNo ratings yet
- Ajr 15 14445Document8 pagesAjr 15 14445Yuriansyah Dwi Rahma PutraNo ratings yet
- Neuroimaging in SchizophreniaDocument15 pagesNeuroimaging in SchizophreniaSam InvincibleNo ratings yet
- Revewer by Bambang Daru Irwanto 1613010006 Inggil Indes RahmantoDocument10 pagesRevewer by Bambang Daru Irwanto 1613010006 Inggil Indes RahmantoadiiiiiiiiiiiiiiNo ratings yet
- Usg Abdomen Pelvis MaleDocument2 pagesUsg Abdomen Pelvis MaleBhaktivedanta HospitalNo ratings yet
- Dietrich Et Al-2002-Journal of Ultrasound in MedicineDocument9 pagesDietrich Et Al-2002-Journal of Ultrasound in MedicineErikaMRSiaNo ratings yet
- JurnalDocument5 pagesJurnalmira ariantiNo ratings yet
- 1 PB PDFDocument7 pages1 PB PDFtrkonjicNo ratings yet
- 01 Cir 57 2 278Document8 pages01 Cir 57 2 278KeneniNo ratings yet
- Lee Et Al 2012 The Utility of Sonography For The Triage of Blunt Abdominal Trauma Patients To Exploratory LaparotomyDocument7 pagesLee Et Al 2012 The Utility of Sonography For The Triage of Blunt Abdominal Trauma Patients To Exploratory LaparotomyThesisaurus IDNo ratings yet
- John Martinelli Ob/Gyn Case: Uterine Fibroids/Anemia 11/17/13Document8 pagesJohn Martinelli Ob/Gyn Case: Uterine Fibroids/Anemia 11/17/13NinaNo ratings yet
- J Ultrasmedbio 2014 12 509Document1 pageJ Ultrasmedbio 2014 12 509Mahatria RajNo ratings yet
- Embryology and Imaging Review of Aortic Arch.3Document12 pagesEmbryology and Imaging Review of Aortic Arch.3Esra SiddigNo ratings yet
- Sindromul AicardiDocument3 pagesSindromul AicardiClaudia Moldovanu100% (1)
- 1.2 Ohkuchi2001Document4 pages1.2 Ohkuchi2001Lina BorreroNo ratings yet
- Congenital Haemangiomas: A Single-Centre Retrospective ReviewDocument7 pagesCongenital Haemangiomas: A Single-Centre Retrospective ReviewIndra GunawanNo ratings yet
- Takotsubo Syndrome: An Overview of Pathophysiology, Diagnosis and Treatment With Emphasis On Cancer PatientsDocument14 pagesTakotsubo Syndrome: An Overview of Pathophysiology, Diagnosis and Treatment With Emphasis On Cancer PatientsAdrián BeltránNo ratings yet
- Symptomatic Bochdalek Hernia in An AdultDocument4 pagesSymptomatic Bochdalek Hernia in An Adultika nur utamiNo ratings yet
- Alport SD Ald Thin MembraneDocument48 pagesAlport SD Ald Thin MembraneHignacio AlarcónNo ratings yet
- Mrs. YUL/ 30 YO/ 1190671/ Bangka Belitung/ Did-Ian/ Ab: Multiple Congenital Malformations O36.5Document16 pagesMrs. YUL/ 30 YO/ 1190671/ Bangka Belitung/ Did-Ian/ Ab: Multiple Congenital Malformations O36.5dian_067No ratings yet
- CR InterpretationDocument2 pagesCR InterpretationDokdem AjaNo ratings yet
- Kojima 2001Document6 pagesKojima 2001Juan Carlos CANo ratings yet
- Glanda HipofizaDocument9 pagesGlanda HipofizaElena-Raluca CiolanNo ratings yet
- Paper Nerve Sheath Tumors 2008 - Da Costa Et AlDocument5 pagesPaper Nerve Sheath Tumors 2008 - Da Costa Et AlRafael Porto GoncalvesNo ratings yet
- History of DysphagiaDocument2 pagesHistory of DysphagiaNader SugarNo ratings yet
- Brief Clinical Report: The Floating Harbor Syndrome With Cardiac Septa1 DefectDocument3 pagesBrief Clinical Report: The Floating Harbor Syndrome With Cardiac Septa1 DefectSarly FebrianaNo ratings yet
- RSC Advances: PaperDocument8 pagesRSC Advances: PaperTrần Thị Như HoaNo ratings yet
- Journal of Ultrasound in Medicine 2007 26 11 1601-1610 PDFDocument10 pagesJournal of Ultrasound in Medicine 2007 26 11 1601-1610 PDFRodrigo AlejandroNo ratings yet
- Comparison of Gadolinium-Enhanced Fat-Saturated T1 - Weighted FLAIR and Fast Spin - Echo MRI of The Spine at 3 T For Evaluation of Extradural LesionsDocument7 pagesComparison of Gadolinium-Enhanced Fat-Saturated T1 - Weighted FLAIR and Fast Spin - Echo MRI of The Spine at 3 T For Evaluation of Extradural Lesionsanon_302681452No ratings yet
- Management of Anterior Shoulder Instability Ask TheDocument10 pagesManagement of Anterior Shoulder Instability Ask Themarcelogascon.oNo ratings yet
- Isolated Diffuse Ground-Glass Opacity in Thoracic CTDocument10 pagesIsolated Diffuse Ground-Glass Opacity in Thoracic CTAyşe BanuNo ratings yet
- Odette's Sonography Portfolio: Patient HistoryDocument2 pagesOdette's Sonography Portfolio: Patient Historyqditya nurNo ratings yet
- Aneurysm Bone Cyst of Proximal PhalynxDocument6 pagesAneurysm Bone Cyst of Proximal Phalynxhemanarasimha gandikotaNo ratings yet
- Miller Shah 2012 Isolated Diffuse Ground Glass Opacity in Thoracic CT Causes and Clinical PresentationsDocument10 pagesMiller Shah 2012 Isolated Diffuse Ground Glass Opacity in Thoracic CT Causes and Clinical PresentationsAndrea PescosolidoNo ratings yet
- Trauma: HX and PE (Adults) : For The EMS Providers, (Prior To Patient'sDocument3 pagesTrauma: HX and PE (Adults) : For The EMS Providers, (Prior To Patient'sJustine CastilloNo ratings yet
- Lung Nodule Detection by Microdose CT Versus Chest RadiographyDocument9 pagesLung Nodule Detection by Microdose CT Versus Chest RadiographyTatiana RecinosNo ratings yet
- Wieczorek 2003Document5 pagesWieczorek 2003ladybieibiNo ratings yet
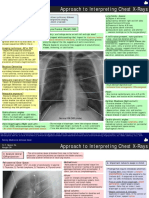
- Chest X RaysDocument19 pagesChest X RaysAbhimanyuKumarNo ratings yet
- COPDDocument14 pagesCOPDaswad 0008No ratings yet
- Patterns of Atrophy in Pathologically Confirmed Dementias: A Voxelwise AnalysisDocument9 pagesPatterns of Atrophy in Pathologically Confirmed Dementias: A Voxelwise AnalysisCaramel luvNo ratings yet
- PATIENT CASE HPI J.O. Is A 5 Yo Girl Who Is Brought To The PediatricDocument5 pagesPATIENT CASE HPI J.O. Is A 5 Yo Girl Who Is Brought To The PediatricKyla ValenciaNo ratings yet
- Transabdominal Sonography in Assessment of The Bowel in AdultsDocument16 pagesTransabdominal Sonography in Assessment of The Bowel in AdultsСергей СадовниковNo ratings yet
- Stree Roga .04Document7 pagesStree Roga .04Prince SoniNo ratings yet
- Eberle 2010Document10 pagesEberle 2010Nasc710No ratings yet
- Can Malignant and Benign Pulmonary Nodules Be Differentiated With Diffusion-Weighted MRI?Document7 pagesCan Malignant and Benign Pulmonary Nodules Be Differentiated With Diffusion-Weighted MRI?Patta DaengNo ratings yet
- Pitfalls in The Sonographic Diagnosis of Uterine Fibroids: American Journal of Roentgenology November 1988Document5 pagesPitfalls in The Sonographic Diagnosis of Uterine Fibroids: American Journal of Roentgenology November 1988MetharisaNo ratings yet
- Incidence of The Bell'Clapper Deformity in An Autopsy SeriesDocument3 pagesIncidence of The Bell'Clapper Deformity in An Autopsy SeriesOttofianus Hewick KalangiNo ratings yet
- Role of Limited Whole-BodyDocument9 pagesRole of Limited Whole-BodytopNo ratings yet
- DiabetesDocument31 pagesDiabetesicaeeNo ratings yet
- What Exactly Are PFTS?: - SpirometryDocument67 pagesWhat Exactly Are PFTS?: - SpirometryicaeeNo ratings yet
- Increased Risk of Latent Tuberculous Infection Among Persons With Pre-Diabetes and Diabetes MellitusDocument9 pagesIncreased Risk of Latent Tuberculous Infection Among Persons With Pre-Diabetes and Diabetes MellitusicaeeNo ratings yet
- Oxidative Stress and TB Outcomes in Patients With Diabetes Mellitus?Document4 pagesOxidative Stress and TB Outcomes in Patients With Diabetes Mellitus?icaeeNo ratings yet
- Treatment of Latent Tuberculosis Infection: Patrick Tang, MD, PHD James Johnston, MDDocument9 pagesTreatment of Latent Tuberculosis Infection: Patrick Tang, MD, PHD James Johnston, MDicaeeNo ratings yet
- HHS Public Access: The Immunology of Tuberculosis: From Bench To BedsideDocument30 pagesHHS Public Access: The Immunology of Tuberculosis: From Bench To BedsideicaeeNo ratings yet
- FervDocument9 pagesFervicaeeNo ratings yet
- Intensified TB Case FindingDocument7 pagesIntensified TB Case FindingicaeeNo ratings yet
- Inflammation and Immunopathogenesis of Tuberculosis ProgressionDocument25 pagesInflammation and Immunopathogenesis of Tuberculosis ProgressionicaeeNo ratings yet
- Reported Edmonton Frail Scale: Frailty Domain Item 0 Point 1 Point 2 Points CognitionDocument1 pageReported Edmonton Frail Scale: Frailty Domain Item 0 Point 1 Point 2 Points CognitionicaeeNo ratings yet
- Tilburg Frailty Indicator (TFI) : Part A Determinants of FrailtyDocument3 pagesTilburg Frailty Indicator (TFI) : Part A Determinants of FrailtyicaeeNo ratings yet
- Pulmonary Manifestations of Birt-Hogg-Dube SyndromeDocument10 pagesPulmonary Manifestations of Birt-Hogg-Dube SyndromeicaeeNo ratings yet
- Tobacco Cessation: Zen Ahmad Pulmonology Division, Internal Medicine Department RSMH PalembangDocument83 pagesTobacco Cessation: Zen Ahmad Pulmonology Division, Internal Medicine Department RSMH PalembangicaeeNo ratings yet
- Three Attempts of Earthquake Prediction With Satellite Cloud ImagesDocument5 pagesThree Attempts of Earthquake Prediction With Satellite Cloud ImagesicaeeNo ratings yet
- Poster Sessions: Abstract P217 Table 1Document3 pagesPoster Sessions: Abstract P217 Table 1icaeeNo ratings yet
- Cattle Yards Third EditionDocument74 pagesCattle Yards Third EditionJose Antonio Alvizo FloresNo ratings yet
- Progress Test 1 (Units 1-3) : A Complete The Sentences With The Words in The BoxDocument7 pagesProgress Test 1 (Units 1-3) : A Complete The Sentences With The Words in The BoxArtur ArnautovNo ratings yet
- Textbook PMDocument46 pagesTextbook PMLai QuocNo ratings yet
- Electronics PDFDocument165 pagesElectronics PDF3334333No ratings yet
- GRP WRKDocument5 pagesGRP WRKrheaNo ratings yet
- CEVNA KAPA DIN2617-Steel-butt-welding-pipe-fittings-capsDocument2 pagesCEVNA KAPA DIN2617-Steel-butt-welding-pipe-fittings-capsBojan BučarNo ratings yet
- Lecture 02Document19 pagesLecture 02Sajjad AhmadNo ratings yet
- Correcting Students' Errors: Theory and Practice: June 2018Document14 pagesCorrecting Students' Errors: Theory and Practice: June 2018Ella Mansel (Carmen M.)No ratings yet
- Weekly Home Learning Plan For Modular Distance Learning Grade 11 - GAS/ICTDocument4 pagesWeekly Home Learning Plan For Modular Distance Learning Grade 11 - GAS/ICTJarven SaguinNo ratings yet
- Natres CasesDocument357 pagesNatres CasesqwertyuiopNo ratings yet
- Multiple-Criteria Policy Anaysis of Circular Debt in PakistanDocument7 pagesMultiple-Criteria Policy Anaysis of Circular Debt in PakistanumairNo ratings yet
- Cognizant: Process AssociateDocument3 pagesCognizant: Process AssociateNomadic World TourNo ratings yet
- First FS - Audioscript - Test 1Document10 pagesFirst FS - Audioscript - Test 1Patrícia Faria0% (2)
- 1 Major PhIlippines Government AgenciesDocument53 pages1 Major PhIlippines Government AgenciesCheska DocumentsNo ratings yet
- Henry ReflectionDocument4 pagesHenry Reflectionapi-584851650No ratings yet
- c12 Chemistry - Tests For The Functional Groups in Organic Compounds Fcs Y1Document6 pagesc12 Chemistry - Tests For The Functional Groups in Organic Compounds Fcs Y1freefireboss633No ratings yet
- Seguimiento Post Tratamiento Hsil AsccpDocument15 pagesSeguimiento Post Tratamiento Hsil AsccpSelene CandiotiNo ratings yet
- Chapter-2 Answer KeyDocument18 pagesChapter-2 Answer KeyKylie sheena MendezNo ratings yet
- Introduction To Traffic EngineeringDocument24 pagesIntroduction To Traffic EngineeringUmar Khan100% (1)
- ch5 DiodecircuitsDocument80 pagesch5 Diodecircuitsadesh patelNo ratings yet
- Kumail Nanjiani Workout PDFDocument11 pagesKumail Nanjiani Workout PDFUlisesYairMayCanoNo ratings yet
- Embedded Systems Lecture 3Document96 pagesEmbedded Systems Lecture 3ኦፍ ላይንNo ratings yet
- Ais Fraud-Case StudyDocument3 pagesAis Fraud-Case StudyErica AlimpolosNo ratings yet
- Focus Group APIC Seattle Confidentiality Agreement 031115Document1 pageFocus Group APIC Seattle Confidentiality Agreement 031115Maira HassanNo ratings yet
- Kristian Solhaug / Kristian - Solhaug@fishbones - As / Phone No. +47 976 56 453Document14 pagesKristian Solhaug / Kristian - Solhaug@fishbones - As / Phone No. +47 976 56 453Darryan DhanpatNo ratings yet