Professional Documents
Culture Documents
Dietary Fat Fro Fow To Friend
Uploaded by
FerMoralesOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Dietary Fat Fro Fow To Friend
Uploaded by
FerMoralesCopyright:
Available Formats
D IE T A N D H E AL TH
REVIEW with energy intake derived mainly from fat. In
support of higher fat intake, several meta-analyses
found slightly greater weight loss on high-fat rather
Dietary fat: From foe to friend? than low-fat diets (9, 10), and preliminary data
suggest the potential for excellent control of dia-
betes through carbohydrate restriction (11, 12).
David S. Ludwig1,2*, Walter C. Willett2,3, Jeff S. Volek4, Marian L. Neuhouser5
But versions of low-carbohydrate, high-fat diets
have been around at least as early as the 1800s,
For decades, dietary advice was based on the premise that high intakes of fat cause
with no clear evidence of superiority for long-term
obesity, diabetes, heart disease, and possibly cancer. Recently, evidence for the adverse
obesity treatment at present. And regardless of
metabolic effects of processed carbohydrate has led to a resurgence in interest in
body weight, high intakes of fat—especially from
lower-carbohydrate and ketogenic diets with high fat content. However, some argue
red meat and dairy products—might increase risk
that the relative quantity of dietary fat and carbohydrate has little relevance to health and
for heart disease or cancer.
that focus should instead be placed on which particular fat or carbohydrate sources are
Perhaps both high-carbohydrate, low-fat and
consumed. This review, by nutrition scientists with widely varying perspectives,
low-carbohydrate, high-fat diets have benefit for
summarizes existing evidence to identify areas of broad consensus amid ongoing
different populations or for different clinical out-
controversy regarding macronutrients and chronic disease.
comes, and the critical issue is to identify the op-
A
timal macronutrient ratio for an individual. Or
report by the U.S. Senate Select Commit- pasta while limiting all fats and oils. To facil- perhaps the focus on macronutrient quantity has
tee on Nutrition and Human Needs in 1977 itate this goal, the U.S. Healthy People 2000 been a distraction, and qualitative aspects (the
called on Americans to reduce consump- report of the Department of Health and Human particular sources of fat or carbohydrate) and
Downloaded from http://science.sciencemag.org/ on November 27, 2018
tion of total and saturated fat, increase car- Services called on the food industry to market overall eating patterns are more important.
bohydrate intake, and lower calorie intake, thousands of new “processed food products that To explore these issues, we have joined to-
among other dietary goals (1). This report, by are reduced in fat and saturated fat” (4). This gether as scientists with a diversity of expertise,
elected members of Congress with little scientific intensive focus on reducing dietary fat was driv- perspectives, and prior research focus. Our aim is
training, was written against a backdrop of grow- en by a prevailing belief that carbohydrates—all not to assemble a premature consensus among
ing public concern about diet-related chronic dis- carbohydrates, including highly processed grains the like-minded, but rather to identify areas of
ease, precipitated in part by attention surrounding and sugar—were innocuous and possibly protec- general agreement and delineate a research agenda
President Eisenhower’s heart attack in 1955. tive against weight gain, cancer, and cardiovas- to address long-standing controversies.
Even then, the recommendations were hotly cular disease through multiple mechanisms (5).
debated. The American Medical Association stated As a result, the proportion of fat in the U.S. The case for a low-fat,
that “The evidence for assuming benefits to be diet decreased from about 42% in the 1970s to high-carbohydrate diet
derived from the adoption of such universal die- about 34% of total calories today (somewhat Physiologic mechanisms
tary goals as set forth in the report is not con- greater than the stated goal of <30%) and the Among many societies worldwide, carbohydrate
clusive … [with] potential for harmful effects.” proportion of dietary carbohydrates increased is the primary source of energy, providing 50% or
Indeed, the lack of scientific consensus was re- substantially (6). During this time, rates of obesity more of daily energy, with lesser amounts from
flected in the voluminous, 869-page “Supplemental and diabetes increased greatly, contributing to both fat and more expensive and scarce protein.
Views” published contemporaneously by the com- the first nationwide decrease in life expectancy Population-level or ecological studies comparing
mittee. Nonetheless, reduction in fat consumption since the flu pandemic 100 years ago (7). These global chronic disease rates show that less devel-
soon became a central principle of dietary guide- trends could be causally connected or unrelated. oped countries have lower rates of cardiovascular
lines from the U.S. government and virtually all If causal, how could some traditional socie- disease, obesity, and cancer than more Wester-
nutrition- and health-related professional organi- ties, such as that of Okinawa, enjoy relative free- nized countries. When individuals move from
zations. [Note that modern approaches to the dom from chronic disease and long lifespan countries with low chronic disease rates to Wester-
study of diet-related chronic diseases were at when they consume a low-fat diet (8)? In Mexico, nized countries, their incidence of chronic diseases
that time in their infancy; previously, nutritional Brazil, and China, rates of obesity and diet-related approaches that of their new country within one
science was focused on individual nutrients for chronic diseases have also increased without sim- to two generations. This rapid shift in chronic
the prevention of deficiency diseases (2).] ilar government dietary guidance to individuals disease rates spurred thinking that environmental
The Surgeon General’s Report on Nutrition and food manufacturers. Moreover, many other exposures, such as adoption of a higher-fat Western
and Health in 1988 identified reduction of fat aspects of the American diet changed in the past diet, may be causally related to disease risk pat-
consumption as the “primary dietary priority,” 40 years, including increased portion sizes, greater terns. [A low-fat diet typically contains <30% en-
with sugar consumption only a secondary con- consumption of foods away from home, and more ergy as fat, and a very-low-fat diet ≤20%, versus
cern for children at risk for dental caries (3). The extreme food processing. At the same time, labor- 32 to 36% in the United States (6).]
1992 Food Guide Pyramid of the U.S. Department saving technology and the digital age have led to Humans ingest complex food mixtures that
of Agriculture advised eating 6 to 11 daily servings declines in occupational and recreational physical include macronutrients (fat, carbohydrate, and
of starchy foods such as bread, cereal, rice, and activity, and budget shortfalls in schools have led protein) and alcohol as energy sources. Macro-
to curtailments in physical education classes, recess nutrients have highly regulated yet integrated
time, and after-school recreation opportunities. metabolic interactions. One consideration for
1
New Balance Foundation Obesity Prevention Center, Boston Despite a lack of clear evidence specifically judging optimal macronutrient intake is the
Children’s Hospital, Boston, MA, USA. 2Harvard Medical relating fat consumption (as a proportion of relative efficiency of substrate oxidation and inter-
School, Boston, MA, USA. 3Departments of Epidemiology total energy intake) to the epidemics of diet- conversion. Humans preferentially oxidize carbo-
and Nutrition, Harvard T. H. Chan School of Public Health
and Channing Division of Network Medicine, Brigham and
related disease—and a lack of high-quality, hydrate over fat, a process that helps to maintain
Women’s Hospital, Boston, MA, USA. 4Department of Human long-term trials focused on macronutrients in blood glucose within homeostatically controlled
Sciences, The Ohio State University, Columbus, OH, USA. general—the pendulum has recently swung in the ranges. Further, carbohydrate consumption acutely
5
Cancer Prevention Program, Division of Public Health opposite direction, with rising consumer popu- increases carbohydrate oxidation, with only a quan-
Sciences, Fred Hutchinson Cancer Research Center, Seattle,
WA, USA.
larity of low-carbohydrate, high-fat diets. Among titatively small increase in de novo lipogenesis
*Corresponding author. Email: david.ludwig@childrens. the current top-10 best-selling weight loss books under typical conditions (13–16). Humans have
harvard.edu on Amazon.com, four promote a ketogenic diet limited storage capacity for carbohydrate but also
Ludwig et al., Science 362, 764–770 (2018) 16 November 2018 1 of 7
have extensive adipose stores, thus favoring fat with less secondary bile acid production and Dietary Modification Trial (WHI-DM), the low-
deposition with excess fat intake (17, 18). Fat is greater production of butyrate and other short- fat intervention (20% energy as fat, as part of
also highly palatable and may have a weak effect chain fatty acids that lower inflammation, decrease a healthy eating pattern) was associated with
on satiation, potentially leading to passive over- cellular proliferation, and enhance expression significant, small reductions in body weight,
consumption (18). This excess intake, if not coupled of genes with antineoplastic properties. Low-fat total fat mass, and percent body fat as measured
with increased energy expenditure, results in weight diets may also decrease serum estradiol and in- by dual x-ray absorptiometry (35). Another ran-
gain. This effect may be enhanced because, by crease sex hormone–binding globulin (32, 33) domized controlled trial (RCT) in postmenopausal
weight, fat provides more than twice as much and may reduce other breast cancer risk factors women tested a lower-fat, higher-carbohydrate
energy (9 kcal/g) as carbohydrate or protein such as mammographic density (34), although diet (20% and 65% energy, respectively), a lower-
(4 kcal/g). Conversely, diets rich in whole grains, the persistence of these effects remains unclear. carbohydrate, higher-fat diet (45% and 35% ener-
which are low in fat and have a relatively low Taken together, these multiple physiologic mech- gy, respectively), and a walnut-rich higher-fat,
glycemic load, promote satiety and reduce over- anisms suggest that higher dietary fat may be lower-carbohydrate diet (18%, 35%, and 45%
consumption, possibly by increasing concentra- harmful for health. However, it is critically im- energy, respectively) for weight loss. All three
tions of glucagon-like peptide–1 after eating (19). portant to consider carbohydrate quality when diets led to weight loss at 12 months, with slightly
Of 29 diets with varying macronutrient com- fat intake is lowered. Refined grains provide negli- higher weight loss in the lower-fat diet group
position tested in mice, only high-fat diets, but not gible nutrition and their high glycemic load causes (33). A meta-analysis of dietary intervention trials
high-carbohydrate diets, led to overconsumption unhealthful spikes in postprandial glucose and showed that low-fat diets were effective for weight
and weight gain (20). Of particular interest, the insulin, promoting hunger, inflammation, insulin loss under ad libitum conditions (36); however,
high-fat diets increased expression of three sero- resistance, and dyslipidemia. However, with a this was published prior to recent carbohydrate-
tonin receptors and both dopamine and opioid lower-fat diet containing high-fiber, low-glycemic restricted diet studies.
signaling pathways, components of the reward carbohydrates such as minimally processed grains, Although obesity has a dominant role in the
Downloaded from http://science.sciencemag.org/ on November 27, 2018
system in the hypothalamus. legumes, and nonstarchy fruits and vegetables, development of diabetes, clinical trial evidence
Fat and specific fatty acids also have adverse these measures improve. Whole plant foods are suggests benefit for low-fat eating patterns in risk
metabolic effects independent of calorie content. also rich sources of micronutrients, antioxidants, reduction and disease management. The Diabetes
High-fat diets up-regulate inflammatory media- and phytochemicals with beneficial health effects. Prevention Program (DPP) was an RCT of 3234
tors including tumor necrosis factor–a (TNF-a), adults at risk for diabetes (37). DPP’s primary goal
interleukins (IL-1b, IL-6) (21), complement (22), Obesity and diabetes was to compare the effect of at least 7% reduc-
and Toll-like receptors (23) in human and animal Low-fat diets may favorably influence body weight tion in body weight achieved by following a low-
studies. In contrast, lower-fat diets reduce amounts and adiposity. In the Women’s Health Initiative calorie, low-fat diet and increasing physical
of these and other inflammatory cyto- activity, with that of the drug metformin
kines, as well as activity of the tran- or a placebo. Rates of diabetes incidence
Box 1. Current controversies.
scription factor NF-kB (24). Palmitic and were reduced by 58% in the lifestyle inter-
stearic acids (abundant in animal foods) 1. Do diets with various carbohydrate-to-fat proportions
vention group and by 31% in those taking
influence the structure and function of metformin, although the effects of dietary
affect body composition (ratio of fat to lean tissue)
mitochondrial membranes, such that an independently of energy intake? Do they affect energy
composition cannot be fully disentangled
increase in these saturated fatty acids expenditure independently of body weight?
from weight loss and other factors. Nu-
leads to impaired membrane function merous other trials and observational
(25). High-fat diets may also promote 2. Do ketogenic diets provide metabolic benefits beyond studies support the use of high-fiber whole
unfavorable epigenetic profiles. For ex- those of moderate carbohydrate restriction? Can they grains and fiber supplements for diabetes
ample, excess saturated fat changes help with prevention or treatment of cardiometabolic disease? prevention and control. A recent meta-
DNA methylation patterns in adipose 3. What are the optimal amounts of specific fatty acids analysis found that fiber, typically con-
tissue (26) and skeletal muscle, and (saturated, monounsaturated, polyunsaturated) in the sumed in greater amounts in low-fat,
alters histone acetylation (27, 28). When context of a very-low-carbohydrate diet? high-carbohydrate diets, improved mea-
acetyl–coenzyme A concentrations are 4. What is the relative importance for cardiovascular disease sures of glycemia and weight (38).
high, such as under conditions of low of the amounts of LDL cholesterol, HDL cholesterol,
glucose, histone acetylation increases Cardiovascular disease
and triglycerides in the blood, or of lipoprotein particle size,
according to in vitro human and animal for persons on diets with distinct fat-to-carbohydrate ratios? The effects of dietary macronutrient com-
studies (28). Are other biomarkers of equivalent or greater importance? position on cardiovascular disease (CVD)
High-fat diets also stimulate hepatic risk have been a subject of debate for
5. What are the effects of dietary fat amount and quality
bile acid synthesis, which, after conver- more than 40 years. Ecological studies
across the lifespan on risk of neurodegenerative, pulmo-
sion into secondary bile acids in the and controlled feeding trials supported
nary, and other diseases that have not been well studied?
colon, may promote tumorigenesis (29–31). associations of higher-fat diets with CVD
Among Africans consuming a diet high 6. What are the long-term efficacies of diets with different or its biomarkers of risk. However, defin-
in minimally processed carbohydrates, carbohydrate-to-fat proportions in chronic disease pre- itive trials have not been conducted that
gut microbial communities were domi- vention and treatment under optimal intervention conditions explicitly test this “diet-heart hypothesis.”
nated by butyrate-producing bacteria, (designed to maximize dietary compliance)? WHI-DM was not designed to test CVD
whereas genetically similar African Amer- 7. What behavioral and environmental interventions can endpoints; even so, participants in the
icans consuming a high-fat diet had a maximize long-term dietary compliance? low-fat group had significantly lower low-
less healthful gut microbiome with high density lipoprotein (LDL) cholesterol and
8. What individual genetic and phenotypic factors predict
secondary bile acid production (31). Fat- metabolic syndrome scores and no un-
long-term beneficial outcomes on diets with various fat-to-
stimulated production of bile acids was favorable changes to high-density lipo-
carbohydrate compositions? Can this knowledge inform per-
also unfavorably associated with in- protein (HDL) cholesterol or triglycerides
sonalized nutrition, with translation to prevention and treatment?
flammation and proliferation in colonic relative to those of controls (39). Although
biopsy samples (29–31). Conversely, high- 9. How does variation in the carbohydrate-to-fat ratio and in the overall results of WHI-DM were neg-
carbohydrate diets containing whole sources of dietary fat affect the affordability and ative for CVD, follow-up showed that
grains and other high-fiber foods provide environmental sustainability of diets? women without baseline hypertension
the preferred fuel for colonic bacteria, had a 30% reduced CVD risk, whereas
Ludwig et al., Science 362, 764–770 (2018) 16 November 2018 2 of 7
D IE T A N D H E AL TH
Substrate oxidation Ketone uptake gests that they may have a role in the public
Carbohydrate brain, heart, muscle health crisis of diet-related chronic disease (49).
Fatty acids As dietary carbohydrate is replaced by fat,
Dietary postprandial spikes in the blood concentrations
Anabolic signaling in adipose carbohydrate βOHB signaling
restriction of glucose and insulin decrease, glucagon secre-
Altered fuel partitioning (HDAC inhibition, NLRP3
inflammasome, NAD+) tion increases, and metabolism shifts to a greater
reliance on fat oxidation (Fig. 1). These metabolic
Effects Additional and hormonal responses are associated with at-
related to pathways
Postprandial oxidative lower associated Reactive oxygen species tenuated oxidative stress and inflammatory re-
stress and inflammation postprandial with Membrane highly sponses after eating (50, 51), reduced hormone
glycemia and ketogenic unsaturated fatty acids resistance [to insulin, leptin, fibroblast growth
insulinemia diets factor–21 (FGF-21), and thyroxine] (52, 53), and
Metabolic syndrome Anti-seizure, improvements in many features of metabolic
components neuroprotection syndrome (54–56)—effects that increase through-
HDL cholesterol
Triglycerides
out the range of carbohydrate restriction. Ad-
Hepatic fat Insulin / IGF-1 signaling (mTOR, PI3K, NF-κB) ditional mechanisms arise as carbohydrate is
Coagulopathy Hormone sensitivity (leptin, insulin, FGF-21, thyroid) restricted to a point that results in nutritional
Chronic inflammation Appetite ketosis, in which serum concentrations of b-
hydroxybutyrate increase from <0.1 mM to 0.5 to
Fig. 1. Pleiotropic effects of low-carbohydrate, high-fat diets. Ketogenic diets (aqua) may 5 mM. This normal physiological state differs from
enhance these effects and act through additional mechanisms. Abbreviations: bOHB, b-hydroxybutyrate; diabetic ketoacidosis, in which b-hydroxybutyrate
Downloaded from http://science.sciencemag.org/ on November 27, 2018
HDAC, histone deacetylase; NAD+, nicotinamide adenine dinucleotide; mTOR, mechanistic target concentrations exceed 10 mM. Ketones, an al-
of rapamycin. ternative fuel used by the brain (57) and heart,
affect metabolic efficiency and a panoply of
signaling functions, producing beneficial changes
those with baseline hypertension or prior CVD Specific types of fats may influence prostate in gene expression, inflammation, oxidative stress,
had no benefit or increased CVD risk; these cancer risk, possibly as a result of effects on cell and possibly health span (58, 59).
findings suggest that a low-fat diet might have a signaling and other cancer-related pathways. In From a pathophysiological perspective, low-
greater effect on prevention than treatment (40). the Prostate Cancer Prevention Trial and the carbohydrate, high-fat diets may directly target
In a meta-analysis of RCTs, addition of at Selenium and Vitamin E Cancer Prevention Trial, underlying metabolic dysfunction in insulin re-
least 3 g of oat b-glucan per day reduced total higher blood measures of omega-3 (N-3) fatty sistance and type 2 diabetes, characterized by
and LDL cholesterol without unfavorable ef- acids, particularly docosahexaenoic acid (DHA), defects in the body’s ability to oxidize ingested
fects on triglycerides or HDL cholesterol (41), were associated with increased risks of both total carbohydrate. With insulin resistance, dietary car-
highlighting the benefits of a low-fat, grain- and high-grade prostate cancer (46, 47). These bohydrate is diverted at increased rates into hepat-
based diet. In another meta-analysis of examined findings are consistent with a study in which ic de novo lipogenesis, resulting in increased
RCTs, low-fat diets lowered LDL cholesterol, a prostate cancer patients were randomly assigned hepatic triglyceride synthesis and abnormal con-
major CVD risk factor, whereas low-carbohydrate to flaxseed supplements [a rich source of the N-3 centrations of lipids in the blood (60). From a
diets lowered triglycerides (42). fat a-linolenic acid (ALA)] or placebo (48). The historical perspective, some aboriginal hunting
supplement led to increased tumor proliferation and fishing cultures (e.g., Inuit of the Arctic and
Cancer and higher prostate-specific antigen (PSA) at First Nations groups in Canada) survived for
Cancer includes more than 100 disease types and prostatectomy. However, the clinical implications millennia with little available dietary carbohy-
subtypes, precluding a comprehensive assess- remain unknown; research is needed to determine drate. In fact, mild ketosis was the “normal” meta-
ment of potential diet effects here, but several whether specific fatty acids should be reduced bolic state for many cultures before the advent
major trials provide useful evidence. In the low- in people at risk for specific cancers. of agriculture (i.e., for all but the last 1% or less
fat diet arm of WHI-DM, there was no significant of the existence of humans as a species). When
effect on total breast cancer incidence, but estro- The case for a low-carbohydrate, these ethnic groups underwent a transition from
gen receptor–positive, progesterone receptor– high-fat diet their low-carbohydrate and high-fat traditional
negative cancers were significantly reduced by Carbohydrate-restricted diets vary in macro- diets, the prevalence of obesity and type 2 diabetes
36% over a mean of 8.1 years of follow-up (32). nutrient composition, but the defining feature increased markedly, although changes in other
Among women who had higher baseline fat is that contributions to total energy are reduced lifestyle factors may have also had a role.
intake (>36.8% of energy), overall risk of breast for carbohydrate and increased for fat (≥40% of
cancer was significantly reduced by 22% over energy) relative to conventional diets. Emerging Obesity, type 2 diabetes, and
a median of 11.5 years. For these women, total evidence suggests that a ketogenic diet—a special cardiovascular disease
and breast cancer deaths were reduced by 22% type of low-carbohydrate diet with fat typically The most recent systematic reviews and meta-
and 14%, respectively. However, a low-fat, high- ≥70% of energy—may have unique therapeutic analyses have concluded that carbohydrate-
carbohydrate intervention conducted in high- effects beyond those of less restrictive regimens. restricted diets tend to outperform low-fat diets
risk women had no significant effect on incidence for short- to medium-term weight loss, espe-
of invasive breast cancer in another study with Physiological mechanism cially in trials that involved a ketogenic diet
a mean 10-year follow-up (43). Breast cancer Conventional lifestyle recommendations and (9, 10, 54, 61). Whereas individuals with insulin
patients in the Women’s Intervention Nutrition existing drug treatments have failed to stem the sensitivity seem to respond similarly to low-fat
Study randomly assigned to the low-fat diet group twin epidemics of obesity and type 2 diabetes. or low-carbohydrate diets, those with insulin
had a statistically significant 24% reduced risk of Nearly three-fourths of U.S. adults are overweight resistance, glucose intolerance, or insulin hy-
cancer relapse relative to controls over a median or obese, and half have prediabetes or diabetes, persecretion may lose more weight on a low-
of 5 years (44). In another randomized trial among despite a 40-year focus on reducing dietary fat. carbohydrate, high-fat diet (62, 63). The lower
breast cancer patients with very low risk of re- The most salient change in macronutrient intake insulin concentrations and accelerated rates
currence, a low-fat, plant-based diet had no effect over this period has been a marked increase in of adipose tissue lipolysis and ketogenesis may
on recurrence or mortality (45). processed starches and added sugars, which sug- provide more stable metabolic fuel availability,
Ludwig et al., Science 362, 764–770 (2018) 16 November 2018 3 of 7
especially for the brain, resulting in greater average glucose concentration) was reduced by Cancer
satiety during weight loss; potential effects on 1.3%, and a majority had HbA1c levels of <6.5% Certain cancer cells rely on glycolysis for energy
energy expenditure remain a subject of inves- (i.e., below the diagnostic threshold for diabe- metabolism. By decreasing glucose flux into tumor
tigation (63). tes) while taking no medications other than cells, a ketogenic diet could target the defective
Metabolic syndrome—including central adi- metformin (11). mitochondrial oxidative phosphorylation spe-
posity, high circulating concentrations of trigly- Low-carbohydrate diets are typically (but not cific to some cancers. Carbohydrate restriction
cerides, low levels of HDL cholesterol, high blood necessarily) high in saturated fat. As discussed might also help to prevent or treat cancer by low-
pressure, glucose intolerance, fatty liver, and below, saturated fat is directly associated with ering oxidative stress, inflammation, and cellular
chronic inflammation—comprises a constellation cardiovascular and total mortality in the gen- signaling involving anabolic hormones such as
of clinical risk factors associated with insulin eral population (although this relation has been insulin (which is thought to mediate in part the
resistance that predispose to diabetes and CVD. a subject of controversy, related in part to the association between obesity and cancer risk)
Reduction in dietary carbohydrate may improve nature of the substituted calories) (68, 69). How- (70, 71). Preclinical data involving various models
these markers more effectively than do low-fat ever, with the higher rates of fatty acid oxidation appear promising, including the use of a ketogenic
diets (54–56, 64). In an 8-week trial of patients and decreased de novo lipogenesis on a ketogenic diet to enhance the effectiveness of phosphoino-
with type 2 diabetes in Italy, a diet high in total diet, blood concentrations of saturated fatty acids sitide 3-kinase (PI3K) inhibitors in cancer treat-
(42% of energy) and monounsaturated (MUFA) and palmitoleic acid (a marker of de novo lipo- ment (72). However, clinical reports are largely
fat decreased liver fat significantly more than did genesis) may decrease (50, 55, 56), suggesting a limited to small case series, with no high-quality
a low-fat (28% of energy), high-fiber diet (65). In lower risk of diabetes and CVD. Furthermore, RCTs.
a 2-year trial conducted at a worksite in Israel, any effects of increased LDL cholesterol (a risk
participants in the low-carbohydrate diet group marker for CVD that occurs in about half of Clinical translation
(fat approximately 40% of energy) lost more individuals on a ketogenic diet) need to be con- Moderately low-carbohydrate diets entail rela-
Downloaded from http://science.sciencemag.org/ on November 27, 2018
weight and experienced greater improvements sidered together with improvements in trigly- tively simple changes in diet, focused primarily
in HDL cholesterol and triglycerides than did cerides, HDL cholesterol, inflammatory markers, on substituting high-fat foods for processed car-
those in the low-fat diet group (fat approximately and other features of metabolic syndrome. How- bohydrates while allowing several daily servings
30% of energy) (66). With restriction of carbohy- ever, there are no long-term studies tracking CVD of whole fruits, legumes, and minimally processed
drate to ketogenic levels (<50 g/day), individ- outcomes. grains. A ketogenic diet may include various
uals with metabolic syndrome lost more nutrient-dense whole foods such as non-
weight, total fat, and abdominal fat than starchy vegetables, nuts, eggs, cheese, but-
did those consuming a low-fat (24% of Box 2. Points of consensus. ter/cream, fish, meats, oils, and select fruits.
energy), calorie-restricted diet (56). The Proper formulation of a ketogenic diet
ketogenic diet also significantly decreased 1. With a focus on nutrient quality, good health and low entails restriction of carbohydrate, adequate
serum triglycerides, increased HDL cho- chronic disease risk can be achieved for many people on but not high intake of protein, and suf-
lesterol concentration, lowered inflamma- diets with a broad range of carbohydrate-to-fat ratios. ficient sodium to offset the natriuretic
tory markers, and reduced concentrations 2. Replacement of saturated fat with naturally occurring effect of ketosis and reduced insulinemia.
of circulating saturated fatty acids (50), unsaturated fats provides health benefits for the general Recent data among motivated patients sug-
consistent with metabolic benefits seen population. Industrially produced trans fats are harmful and gest the possibility of good compliance
in other studies (67). should be eliminated.The metabolism of saturated fat may differ and improved quality of life through 1 year
Carbohydrate restriction in general, on carbohydrate-restricted diets, an issue that requires study. (11), although safety has not been fully as-
and specifically a ketogenic diet, may 3. Replacement of highly processed carbohydrates (includ- sessed in long-term trials.
provide exceptional benefits in the set- ing refined grains, potato products, and free sugars) with
ting of diabetes, essentially a disease of The case for dietary fat quality
unprocessed carbohydrates (nonstarchy vegetables, whole
carbohydrate intolerance. Historically, fruits, legumes, and whole or minimally processed grains) At one time, dietary fat, primarily trigly-
ketogenic diets were the treatment of provides health benefits. cerides, was considered simply a source
choice for diabetes, but the discovery 4. Biological factors appear to influence responses to diets
of energy. However, the fatty acids in
of insulin in the early 1920s allowed for of differing macronutrient composition. People with rela-
triglycerides can vary in chain length,
control of acute symptoms on higher- tively normal insulin sensitivity and b cell function may do
number and position of double bonds,
carbohydrate diets. By the 1980s, low- well on diets with a wide range of carbohydrate-to-fat
and whether the double bonds are in cis
fat diets with up to 60% energy from ratios; those with insulin resistance, hypersecretion of
or trans configuration. These features
carbohydrate had become the standard insulin, or glucose intolerance may benefit from a lower-
profoundly affect the biological function
of care, although current recommenda- carbohydrate, higher-fat diet.
of fatty acids, and thus their effects on
tions emphasize individualizing macro- heath, in complex, incompletely under-
5. A ketogenic diet may confer particular metabolic benefits
nutrient composition. However, despite stood ways.
for some people with abnormal carbohydrate metabolism,
modern insulin analogs and glucose mon- The position of double bonds, described
a possibility that requires long-term study.
itoring technologies, management of dia- by the number of carbons from the non-
betes remains suboptimal. In a recent 6. Well-formulated low-carbohydrate, high-fat diets do carboxyl end of the fatty acid to the first
survey, 316 children and adults with type 1 not require high intakes of protein or animal products. double bond, has particular importance.
diabetes following a low-carbohydrate, Reduced carbohydrate consumption can be achieved by Two families of polyunsaturated fatty
high-fat diet for a mean of >2 years re- substituting grains, starchy vegetables, and sugars with acids (PUFAs), the N-3 and N-6 fatty acids,
ported exceptional glycemic control, low nonhydrogenated plant oils, nuts, seeds, avocado, and are essential because they cannot be syn-
rates of complications, and excellent other high-fat plant foods. thesized by humans. Both are critical com-
metabolic health markers (12). Among 7. There is broad agreement regarding the fundamental ponents of every human cell membrane
262 participants with type 2 diabetes components of a healthful diet that can serve to inform and are precursors of eicosanoid hormones
assigned to a ketogenic diet with inten- policy, clinical management, and individual dietary choice. that mediate inflammation, thrombosis,
sive telemedicine support, 83% completed Nonetheless, important questions relevant to the epidemics immunity, and insulin resistance. An in-
the 1-year intervention; in this group, of diet-related chronic disease remain. Greater investment in crease in N-3 fatty acid intake alters expres-
weight was reduced by 12%, hemoglobin nutrition research should assume a high priority. sion of more than 6000 genes, underscoring
A1c (HbA1c, a measure of long-term this biological complexity (73).
Ludwig et al., Science 362, 764–770 (2018) 16 November 2018 4 of 7
D IE T A N D H E AL TH
A vast literature based on controlled feeding gained widespread recognition. In animals, N-3
about 75%, although lower rates of tobacco use
studies with physiologic endpoints, long-term fatty acids protect against cardiac arrhythmias,
and other prevention efforts (e.g., statins) con-
epidemiologic studies, and randomized trials tributed to this secular trend. and in epidemiologic studies, intakes of N-3 fatty
with clinical outcomes has documented that the acids [DHA or eicosapentaenoic acid (EPA) from
In subsequent epidemiologic studies, blood
type of dietary fat strongly influences human fish and ALA from plant sources] are inversely
lipid subfractions predicted CVD better than did
health independent of total fat intake. N-6 and but nonlinearly associated with risk of sudden
total cholesterol; higher amounts of LDL choles-
N-3 fatty acids provide benefit at intakes above cardiac death (88). Specifically, risk decreases
terol and triglycerides are associated with higher
minimum levels to prevent essential fatty acid with intakes up to about 250 mg/day (equivalent
risk, whereas higher amounts of HDL cholesterol
deficiency, and nonessential dietary fatty acids to one or two servings of fish per week) but then
predict lower risk (82). In further controlled feed-
also have important metabolic effects. plateaus. The inconsistent effects of supplements
ing studies, replacement of saturated fat with
seen in these RCTs may relate to the variability in
carbohydrates reduced both LDL cholesterol and
Obesity and diabetes intakes within and among populations (intakes
HDL cholesterol and increased blood concen-
Whereas the literature on total fat intake is ex- among some individuals in the United States
trations of triglyceride during fasting, suggest-
tensive, little is known about the effects of specific and mean intakes in many countries remain very
ing little or potentially adverse effects on risk of
types of fat on weight control and body com- low) (89). At high dosage, fish oil supplements
CVD. Replacement of monounsaturated or poly-
position. In a 7-week controlled overfeeding study, may reduce the risk of cardiovascular events
unsaturated fat with carbohydrate increased LDL
saturated fat increased hepatic and visceral fat such as heart attack and stroke among people
cholesterol and had minimal effects on HDL
storage relative to polyunsaturated fat (74). In cholesterol or triglycerides. with hypertriglyceridemia, according to prelim-
a large cohort analysis (75), increases in the in- inary data from a large trial (90)—a possibility
Consistent with the controlled feeding studies
takes of trans and saturated fat were positively that warrants further study.
of blood lipids, in several randomized trials with
associated with weight gain when The main N-6 PUFA in diets, linoleic
Downloaded from http://science.sciencemag.org/ on November 27, 2018
compared isocalorically with carbo- acid, can be elongated and desaturated
20 Trans fat
hydrate, but intakes of MUFA and to form eicosanoids that are prothrom-
15
Change in total mortality, %
PUFAs did not influence weight. To Saturated fat botic and proinflammatory. In addi-
our knowledge, no RCTs lasting 1 year 10 tion, linoleic acid may competitively
or longer have compared the effects of 5 inhibit biosynthetic pathways shared
different types of fat on body weight. by the N-3 fatty acid ALA in the for-
0
Consistent with the effects of trans mation of antithrombotic and anti-
fat on multiple components of meta- -5 inflammatory eicosanoids. For these
bolic syndrome (see below), higher -10 reasons, some have concluded that
Monounsaturated fat
intake was associated with risk of type -15 higher N-6 fatty acid intake should be
2 diabetes in a large cohort study with -20 minimized to prevent CVD and other
repeated measures of diet (76). In a diseases associated with chronic in-
-25
10-week randomized trial, consumption Polyunsaturated fat flammation. However, this reasoning
of PUFA reduced biomarkers of in- -30 disregards evidence that N-6 PUFA
0 1 2 3 4 5
sulin resistance relative to consumption intermediates in these pathways, such
of saturated fat (77 ). In a large cohort Increment of energy from specific type of fat, % as arachidonic acid, are highly regu-
study, the ratio of polyunsaturated lated (91). Although very high intakes
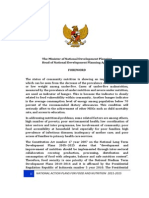
Fig. 2. Relation between increasing intakes of trans, saturated,
to saturated fat intake was inversely of N-6 PUFA increase inflammatory
unsaturated, monounsaturated, and polyunsaturated fatty acid
associated with risk of type 2 diabetes measures in some animal models, this
(compared isocalorically with carbohydrate) in relation to total
(76), and relative blood levels of linoleic effect has not been convincingly dem-
mortality. Data are based on 126,233 men and women followed
acid, which reflect intake, were inverse- onstrated in humans (92); higher in-
for up to 32 years, with assessments every 4 years, as described in
ly associated with risk of type 2 dia- take of linoleic acid in humans may
Wang et al. (94). The strong inverse association with polyunsaturated
betes in a pooled analysis of 20 cohort actually have anti-inflammatory effects
fatty acids was primarily due to N-6 polyunsaturated fatty acids;
studies (78). (93). Moreover, the ratio of N-6 to N-3
associations with N-3 polyunsaturated fatty acids were weaker.
fatty acids has not been associated
Cardiovascular disease with risk of CVD, consistent with both
Early evidence on dietary fats and CVD was based CVD as the outcome, replacement of saturated being beneficial (94). Nonetheless, special effects
FIGURE 2 REPRINTED WITH PERMISSION OF THE AMERICAN MEDICAL ASSOCIATION
on comparisons of incidence and mortality rates fat with PUFA reduced the risk of CVD, whereas in subgroups or at very low intakes of carbohy-
across geographical areas, and on knowledge of replacement with carbohydrate did not (83); how- drate cannot be ruled out.
the effects of dietary fats on blood cholesterol ever, these studies were small, short-term, and The process of partial hydrogenation, which
levels. In the Seven Countries Study (79), per had other limitations (e.g., a lack of emphasis on creates trans isomers from the natural cis double
capita intake of saturated fat, but not total fat, carbohydrate quality). Long-term prospective bonds of fatty acids, was widely used to create
was strongly correlated with rates of CVD; although cohort studies are also consistent with these find- margarine and vegetable shortening with favor-
potentially confounded by other variables, this ings: When compared isocalorically with saturated able commercial properties (solidity at room tem-
provided a strong incentive to understand the fat, N-6 PUFAs—but not typical carbohydrates perature, long shelf life). This industrial process
major geographical variation in CVD rates. In in Western diets—are associated with lower risk altered the structure and function of linoleic acid
controlled feeding studies lasting several weeks, of CVD (84–86). Controlled for other types of fat, and ALA, the dominant fatty acids in many widely
compared isocalorically to carbohydrate, satu- MUFAs are also inversely associated with risk. used oils, resulting in major health impacts. Trans
rated fat increased blood cholesterol concentra- This inverse association with PUFA is linear up fat has uniquely adverse effects on LDL, LDL par-
tions, whereas PUFA reduced them (80, 81). Thus, to about 8% of energy, beyond which data are ticle size, HDL, triglycerides, and inflammatory
from the 1960s, dietary advice to reduce CVD sparse. These epidemiologic studies also high- factors (95). In multiple large-cohort studies, in-
emphasized replacing saturated fat with PUFAs, light the importance of carbohydrate quality; take of trans fat is directly associated with risk of
primarily N-6, and consumption of N-6 PUFA in relative to saturated fat, whole grains are asso- coronary heart disease and other chronic illnesses.
the United States increased from approximately ciated with lower CVD risk (87). Through regulations, education, and food label-
3% to 7% of energy. Concurrently, age-adjusted By the 1990s, the distinction between N-6 and ing, trans fat was largely eliminated from the food
coronary heart disease mortality decreased by N-3 PUFAs and between cis and trans isomers supply in the United States and some European
Ludwig et al., Science 362, 764–770 (2018) 16 November 2018 5 of 7
countries. However, intake remains high in some United States invests a fraction of a cent on nu- 17. A. Astrup, A. Raben, Eur. J. Clin. Nutr. 46, 611–620
parts of the world. trition research for each dollar spent on treatment (1992).
18. J. E. Blundell, J. I. MacDiarmid, J. Am. Diet. Assoc. 97
of diet-related chronic disease. All too often,
Cancer (suppl.), S63–S69 (1997).
scientific results in this field have been ambig- 19. S. S. Runchey et al., Metabolism 62, 188–195
Mechanistic studies have suggested that both uous: Macronutrient feeding studies have been (2013).
N-6 and N-3 fatty acids could either increase or too short and too small to distinguish transient 20. S. Hu et al., Cell Metab. 28, 415–431.e4 (2018).
reduce cancer risk (46–48), and some animal from chronic effects; many behavioral trials have 21. M. Valdearcos, A. W. Xu, S. K. Koliwad, Annu. Rev. Physiol. 77,
131–160 (2015).
studies have suggested that intakes of PUFA lacked the intensity to produce meaningful differ-
22. S. K. Doerner et al., Mol. Cancer Res. 14, 953–965
beyond the range of typical human diets might ences between dietary treatment groups; and (2016).
increase risks. In human studies, consumption observational studies can be affected by con- 23. R. G. Snodgrass, S. Huang, I. W. Choi, J. C. Rutledge,
of these fatty acids and other specific types of fat founding, inability to distinguish cause and effect, D. H. Hwang, J. Immunol. 191, 4337–4347 (2013).
during midlife do not have consistent relation- and other methodological problems. Furthermore, 24. J. V. Heymach et al., Cancer Prev. Res. 4, 1590–1598
(2011).
ships to risks of various cancers, according to despite promising preliminary data, few major 25. E. M. Sullivan et al., Adv. Nutr. 9, 247–262 (2018).
biomarkers of intake and assessments of diet studies of a ketogenic diet in the treatment of di- 26. A. Perfilyev et al., Am. J. Clin. Nutr. 105, 991–1000
(96). Higher intake of fat from animal sources, abetes have been conducted. Additional questions (2017).
but not vegetable sources, during early adult life related to sustainability for the individual (whether 27. J. A. Martínez, F. I. Milagro, K. J. Claycombe, K. L. Schalinske,
was associated with higher risk of breast cancer, people can realistically remain on prescribed diets) Adv. Nutr. 5, 71–81 (2014).
28. B. Paul et al., Clin. Epigenetics 7, 112 (2015).
which may reflect the type of fat or nonlipid factors and for the environment (the impacts of specific 29. S. J. O’Keefe, Nat. Rev. Gastroenterol. Hepatol. 13, 691–706
(97). Because of long latencies and windows of dietary patterns on natural resources and climate (2016).
vulnerability for carcinogenic influences, further change) require more study. Given the enormous 30. S. Ocvirk, S. J. O’Keefe, Curr. Nutr. Rep. 6, 315–322
studies of specific types of fat across the lifespan human and economic toll of diet-related disease, (2017).
Downloaded from http://science.sciencemag.org/ on November 27, 2018
are desirable. high-quality research into key controversies should 31. J. Ou et al., Am. J. Clin. Nutr. 98, 111–120 (2013).
32. R. L. Prentice et al., JAMA 295, 629–642 (2006).
be given priority. 33. C. L. Rock et al., Metabolism 65, 1605–1613 (2016).
Other outcomes The incomplete nature of research notwith- 34. N. F. Boyd et al., J. Natl. Cancer Inst. 89, 488–496
Adequate intake of both N-6 and N-3 fatty acids standing, data from multiple lines of investiga- (1997).
in utero and during early life is critical for neuro- tion have led to important areas of consensus 35. C. L. Carty et al., Am. J. Clin. Nutr. 93, 516–524
logical development because these fatty acids (Box 2). Current evidence indicates that no (2011).
36. A. Astrup, G. K. Grunwald, E. L. Melanson, W. H. M. Saris,
constitute much of the lipid in the central nervous specific carbohydrate-to-fat ratio in the diet is J. O. Hill, Int. J. Obes. 24, 1545–1552 (2000).
system. Low consumption of fish, the primary best for the general population. Nor do all diets, 37. Diabetes Prevention Program Research Group, N. Engl. J.
source of DHA and EPA, during pregnancy is as- and calorie sources, have similar metabolic effects Med. 346, 393–403 (2002).
sociated with lower cognitive function and preterm in everyone. With attention to diet quality—and 38. S. V. Thompson, B. A. Hannon, R. An, H. D. Holscher, Am. J.
Clin. Nutr. 106, 1514–1528 (2017).
birth (98, 99). In later life, lower consumption of specifically a focus on reducing processed foods,
39. B. V. Howard et al., JAMA 295, 655–666 (2006).
N-3 fatty acids and higher consumption of trans including sugar and refined grains—many peo- 40. R. L. Prentice et al., Am. J. Clin. Nutr. 106, 35–43
fats have been associated with greater risk of ple do relatively well with substantial variation (2017).
dementia (100). in macronutrient composition (102). For the rapid- 41. A. Whitehead, E. J. Beck, S. Tosh, T. M. Wolever, Am. J. Clin.
In a recent prospective study, 126,233 men and ly rising proportion of the population with severe Nutr. 100, 1413–1421 (2014).
42. A. J. Nordmann et al., Arch. Intern. Med. 166, 285–293
women were followed for up to 32 years, with metabolic dysfunction or diabetes, a more specific (2006).
diet assessed every 4 years (94). Compared iso- dietary prescription may be needed. 43. L. J. Martin et al., Cancer Res. 71, 123–133 (2011).
calorically to carbohydrate intake, intake of trans 44. R. T. Chlebowski et al., J. Natl. Cancer Inst. 98, 1767–1776
fat was strongly associated with higher mortality. (2006).
45. J. P. Pierce et al., JAMA 298, 289–298 (2007).
Intakes of MUFA and N-3 PUFA were weakly RE FERENCES AND NOTES 46. T. M. Brasky et al., J. Natl. Cancer Inst. 105, 1132–1141
associated with lower mortality, and intake of 1. U. S. Senate Select Committee on Nutrition and Human (2013).
N-6 PUFA was strongly associated with lower Needs, Dietary Goals for the United States, Second Edition 47. T. M. Brasky et al., Am. J. Epidemiol. 173, 1429–1439
mortality (Fig. 2). Because of reductions in sat- (U.S. Government Printing Office, 1977). (2011).
2. D. Mozaffarian, D. S. Ludwig, JAMA 304, 681–682 48. M. Azrad et al., PLOS ONE 7, e53104 (2012).
urated and trans fats over the study period, (2010). 49. E. Cohen et al., Nutrition 31, 727–732 (2015).
total fat intake was inversely associated with 3. J. M. McGinnis, M. Nestle, Am. J. Clin. Nutr. 49, 23–28 50. C. E. Forsythe et al., Lipids 43, 65–77 (2008).
mortality. (1989). 51. D. S. Ludwig, JAMA 287, 2414–2423 (2002).
4. Public Health Service, U.S. Department of Health and Human 52. B. M. Hron, C. B. Ebbeling, H. A. Feldman, D. S. Ludwig,
Conclusion Services, Healthy People 2000: National Health Promotion Nutr. Metab. 14, 44 (2017).
and Disease Prevention Objective (1991). 53. C. B. Ebbeling et al., JAMA 307, 2627–2634 (2012).
The optimal proportion of carbohydrate to fat 5. J. O. Hill, A. M. Prentice, Am. J. Clin. Nutr. 62, 264S–273S 54. N. Mansoor, K. J. Vinknes, M. B. Veierød, K. Retterstøl, Br. J.
in the diet for obesity treatment and chronic (1995). Nutr. 115, 466–479 (2016).
disease prevention has been a topic of debate 6. G. L. Austin, L. G. Ogden, J. O. Hill, Am. J. Clin. Nutr. 93, 55. J. S. Volek, M. L. Fernandez, R. D. Feinman, S. D. Phinney,
836–843 (2011). Prog. Lipid Res. 47, 307–318 (2008).
for decades, often generating more heat than 7. D. S. Ludwig, JAMA 315, 2269–2270 (2016). 56. J. S. Volek et al., Lipids 44, 297–309 (2009).
light (101). Of course, any meaningful assessment 8. D. C. Willcox, B. J. Willcox, H. Todoriki, M. Suzuki, J. Am. Coll. 57. S. C. Cunnane et al., Front. Mol. Neurosci. 9, 53
of a diet’s impact on health must extend far beyond Nutr. 28 (suppl.), 500S–516S (2009). (2016).
macronutrient quantity, to include the myriad 9. N. B. Bueno, I. S. de Melo, S. L. de Oliveira, 58. G. F. Cahill Jr., Annu. Rev. Nutr. 26, 1–22 (2006).
T. da Rocha Ataide, Br. J. Nutr. 110, 1178–1187 (2013). 59. J. C. Newman, E. Verdin, Annu. Rev. Nutr. 37, 51–76
qualitative aspects of food and food combina- 10. D. K. Tobias et al., Lancet Diabetes Endocrinol. 3, 968–979 (2017).
tions that influence hormonal response, gene (2015). 60. K. F. Petersen et al., Proc. Natl. Acad. Sci. U.S.A. 104,
expression, and metabolic pathways. Further 11. S. J. Hallberg et al., Diabetes Ther. 9, 583–612 12587–12594 (2007).
complicating this issue is the likelihood that (2018). 61. J. Sackner-Bernstein, D. Kanter, S. Kaul, PLOS ONE 10,
12. B. S. Lennerz et al., Pediatrics 141, e20173349 e0139817 (2015).
inherent or acquired biological differences among (2018). 62. M. F. Hjorth, Y. Zohar, J. O. Hill, A. Astrup, Annu. Rev. Nutr.
individuals or populations, especially related to 13. F. Diraison et al., J. Lipid Res. 44, 846–853 (2003). 38, 245–272 (2018).
glucose homeostasis, affect response to specific 14. L. C. Hudgins et al., J. Nutr. Biochem. 19, 237–245 63. D. S. Ludwig, C. B. Ebbeling, JAMA Intern. Med. 178,
diets. (2008). 1098–1103 (2018).
15. E. J. Parks, R. M. Krauss, M. P. Christiansen, R. A. Neese, 64. E. J. van Zuuren, Z. Fedorowicz, T. Kuijpers, H. Pijl, Am. J.
Unfortunately, the national nutrition research M. K. Hellerstein, J. Clin. Invest. 104, 1087–1096 (1999). Clin. Nutr. 108, 300–331 (2018).
agenda has not been adequate to address impor- 16. J. M. Schwarz, R. A. Neese, S. Turner, D. Dare, 65. L. Bozzetto et al., Diabetes Care 35, 1429–1435
tant areas of controversy (Box 1). Currently, the M. K. Hellerstein, J. Clin. Invest. 96, 2735–2743 (1995). (2012).
Ludwig et al., Science 362, 764–770 (2018) 16 November 2018 6 of 7
D IE T A N D H E AL TH
66. I. Shai et al., N. Engl. J. Med. 359, 229–241 (2008). 82. R. P. Mensink, P. L. Zock, A. D. Kester, M. B. Katan, Am. J. 96. World Cancer Research Fund and American Institute for
67. N. H. Bhanpuri et al., Cardiovasc. Diabetol. 17, 56 (2018). Clin. Nutr. 77, 1146–1155 (2003). Cancer Research, Diet, Nutrition, Physical Activity and
68. P. W. Siri-Tarino, Q. Sun, F. B. Hu, R. M. Krauss, Am. J. Clin. 83. F. M. Sacks et al., Circulation 136, e1–e23 (2017). Cancer: A Global Perspective (2018); www.wcrf.org/sites/
Nutr. 91, 535–546 (2010). 84. M. U. Jakobsen et al., Am. J. Clin. Nutr. 89, 1425–1432 default/files/Summary-third-expert-report.pdf.
69. M. Dehghan et al., Lancet 390, 2050–2062 (2017). (2009). 97. E. Cho et al., J. Natl. Cancer Inst. 95, 1079–1085
70. A. Poff, A. P. Koutnik, K. M. Egan, S. Sahebjam, 85. F. B. Hu et al., N. Engl. J. Med. 337, 1491–1499 (2003).
D. D’Agostino, Semin. Cancer Biol. 10.1016/ (1997). 98. E. Oken et al., Am. J. Epidemiol. 167, 1171–1181
j.semcancer.2017.12.011 (2017). 86. M. S. Farvid et al., Circulation 130, 1568–1578 (2008).
71. P. N. Hyde, M. B. Lustberg, V. J. Miller, R. A. LaFountain, (2014). 99. A. Horvath, B. Koletzko, H. Szajewska, Br. J. Nutr. 98,
J. S. Volek, Cancer Treat. Res. Commun. 12, 32–39 87. G. Zong et al., BMJ 355, i5796 (2016). 253–259 (2007).
(2017). 88. D. Mozaffarian, J. H. Wu, J. Am. Coll. Cardiol. 58, 2047–2067 100. M. C. Morris, Proc. Nutr. Soc. 71, 1–13 (2012).
72. B. D. Hopkins et al., Nature 560, 499–503 (2018). (2011). 101. J. Palfreman, producer, “Diet Wars” episode of Frontline
73. A. Jans et al., Am. J. Clin. Nutr. 95, 825–836 (2012). 89. S. Petrova, P. Dimitrov, W. C. Willett, H. Campos, Public (WGBH-TV, 2004); www.pbs.org/wgbh/pages/frontline/
74. F. Rosqvist et al., Diabetes 63, 2356–2368 (2014). Health Nutr. 14, 1157–1164 (2011). shows/diet/.
75. A. E. Field, W. C. Willett, L. Lissner, G. A. Colditz, Obesity 15, 90. A. O’Connor, “Fish oil drug may reduce heart attack and 102. C. D. Gardner et al., JAMA 319, 667–679 (2018).
967–976 (2007). stroke risks for some.” New York Times, 25 September 2018;
76. F. B. Hu et al., N. Engl. J. Med. 345, 790–797 (2001). www.nytimes.com/2018/09/25/well/fish-oil-heart-attack- AC KNOWLED GME NTS
77. H. Bjermo et al., Am. J. Clin. Nutr. 95, 1003–1012 stroke-triglycerides-omega-3s.html. Funding: D.S.L. was supported in part by a career award from
(2012). 91. B. S. Rett, J. Whelan, Nutr. Metab. 8, 36 (2011). the National Institute of Diabetes and Digestive and Kidney
78. J. H. Y. Wu et al., Lancet Diabetes Endocrinol. 5, 965–974 92. H. Su, R. Liu, M. Chang, J. Huang, X. Wang, Food Funct. 8, Diseases (K24DK082730). Competing interests: D.S.L., W.C.W.,
(2017). 3091–3103 (2017). and J.S.V. received royalties for books about obesity and nutrition
79. A. Keys, Seven Countries: A Multivariate Analysis 93. K. L. Fritsche, Prostaglandins Leukot. Essent. Fatty Acids 79, that include recommendations on dietary fat. J.S.V. is a founder,
of Death and Coronary Heart Disease (Harvard Univ. Press, 173–175 (2008). stockholder, and consultant for VirtaHealth Corp. and a member
1980). 94. D. D. Wang et al., JAMA Intern. Med. 176, 1134–1145 of the advisory boards for Atkins Nutritionals Inc., UCAN Co.,
80. A. Keyes, J. T. Anderson, F. Grande, Metabolism 14, 747–758 (2016). and Axcess Global.
Downloaded from http://science.sciencemag.org/ on November 27, 2018
(1965). 95. D. Mozaffarian, M. B. Katan, A. Ascherio, M. J. Stampfer,
81. D. M. Hegsted, Am. J. Clin. Nutr. 44, 299–305 (1986). W. C. Willett, N. Engl. J. Med. 354, 1601–1613 (2006). 10.1126/science.aau2096
Ludwig et al., Science 362, 764–770 (2018) 16 November 2018 7 of 7
Dietary fat: From foe to friend?
David S. Ludwig, Walter C. Willett, Jeff S. Volek and Marian L. Neuhouser
Science 362 (6416), 764-770.
DOI: 10.1126/science.aau2096
Downloaded from http://science.sciencemag.org/ on November 27, 2018
ARTICLE TOOLS http://science.sciencemag.org/content/362/6416/764
RELATED http://science.sciencemag.org/content/sci/362/6416/762.full
CONTENT
http://science.sciencemag.org/content/sci/362/6416/770.full
http://science.sciencemag.org/content/sci/362/6416/776.full
http://science.sciencemag.org/content/sci/362/6416/781.full
REFERENCES This article cites 95 articles, 27 of which you can access for free
http://science.sciencemag.org/content/362/6416/764#BIBL
PERMISSIONS http://www.sciencemag.org/help/reprints-and-permissions
Use of this article is subject to the Terms of Service
Science (print ISSN 0036-8075; online ISSN 1095-9203) is published by the American Association for the Advancement of
Science, 1200 New York Avenue NW, Washington, DC 20005. 2017 © The Authors, some rights reserved; exclusive
licensee American Association for the Advancement of Science. No claim to original U.S. Government Works. The title
Science is a registered trademark of AAAS.
You might also like
- ACHTERBERG - Is One Theory Better Than Another in Nutrition Education PDFDocument3 pagesACHTERBERG - Is One Theory Better Than Another in Nutrition Education PDFfeflao1203No ratings yet
- Human Energy RequirementsDocument103 pagesHuman Energy RequirementsDaisy100% (2)
- C2 - Lectura Obligatoria PDFDocument10 pagesC2 - Lectura Obligatoria PDFFerMoralesNo ratings yet
- Contextualizing Salutogenesis and Antonovsky in Public Health DevelopmentDocument7 pagesContextualizing Salutogenesis and Antonovsky in Public Health DevelopmentFerMoralesNo ratings yet
- Human Energy RequirementsDocument103 pagesHuman Energy RequirementsDaisy100% (2)
- Dietary Fat Fro Fow To FriendDocument8 pagesDietary Fat Fro Fow To FriendFerMoralesNo ratings yet
- Human Energy RequirementsDocument103 pagesHuman Energy RequirementsDaisy100% (2)
- Manual Antropometría Nanhes PDFDocument95 pagesManual Antropometría Nanhes PDFFerMoralesNo ratings yet
- Local Anesthesia Techniques in Oral and Maxillofacial SurgeryDocument102 pagesLocal Anesthesia Techniques in Oral and Maxillofacial Surgerydr_jamal1983No ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Sleep DisordersDocument32 pagesSleep Disordersmbah&dukunNo ratings yet
- Pe TransesDocument3 pagesPe TransesMa. Erika Charisse DacerNo ratings yet
- National Food and Nutrition Action PlanDocument83 pagesNational Food and Nutrition Action PlanVicky CeunfinNo ratings yet
- Fat in the Body Digestion, Mobilization and TransportDocument7 pagesFat in the Body Digestion, Mobilization and TransportSisfa ShabelaNo ratings yet
- ACTIVITY - Reflection (Guarino-BSN 101)Document3 pagesACTIVITY - Reflection (Guarino-BSN 101)Mikhaella GwenckyNo ratings yet
- IOSH MS 5.0 Risk Assessment Project PDFDocument2 pagesIOSH MS 5.0 Risk Assessment Project PDFHassan Ur RehmanNo ratings yet
- My Traning PlanDocument2 pagesMy Traning PlanHirohata AkiraNo ratings yet
- Matarese2012 PDFDocument11 pagesMatarese2012 PDFYacine Tarik AizelNo ratings yet
- The Extraordinary Importance of SleepDocument6 pagesThe Extraordinary Importance of SleepFaki D'pasnizerNo ratings yet
- Obesity Project 2021Document16 pagesObesity Project 2021JIESSNU A/L ANBARASU MoeNo ratings yet
- Pasquale Sodexo ResumeDocument2 pagesPasquale Sodexo Resumeapi-304808899No ratings yet
- Body CompositionDocument23 pagesBody CompositionGrantt ChristianNo ratings yet
- Chapter 1 - IntroductionDocument7 pagesChapter 1 - IntroductionWan Nur Nabilah100% (1)
- What Is A MetCon WorkoutDocument2 pagesWhat Is A MetCon WorkoutDaniyal YounasNo ratings yet
- Hiit. Hiit.: Natacha Océane Natacha Océane Natacha Océane Natacha OcéaneDocument27 pagesHiit. Hiit.: Natacha Océane Natacha Océane Natacha Océane Natacha Océanesoniprajna100% (1)
- PE7 Q2 M1 StrengthsandWeaknessesinSkills v2Document19 pagesPE7 Q2 M1 StrengthsandWeaknessesinSkills v2Jamie Fernandez100% (1)
- Insanity - Dig Deeper!: Week 1 6-Jan 7-Jan 8-JanDocument3 pagesInsanity - Dig Deeper!: Week 1 6-Jan 7-Jan 8-JanCarlos RodriguezNo ratings yet
- Guide To Greater Glutes UpdatedDocument64 pagesGuide To Greater Glutes UpdatedOdalis ChavezNo ratings yet
- Art of Barbell - Mindful Eating Journal - Mindful Eating Letter Navy PDFDocument1 pageArt of Barbell - Mindful Eating Journal - Mindful Eating Letter Navy PDFZack MorrisonNo ratings yet
- BTB WorkoutSystemDocument46 pagesBTB WorkoutSystemAhmad Adel El-Kilany100% (2)
- Module 1-Lesson 1: Optimize Energy System Through Dance: Pre-AssessmentDocument4 pagesModule 1-Lesson 1: Optimize Energy System Through Dance: Pre-AssessmentChum VergaraNo ratings yet
- AdolescenceDocument20 pagesAdolescenceRj SantiagoNo ratings yet
- Argument EssayDocument7 pagesArgument Essayapi-331361162No ratings yet
- Physical Fitness Test Template 2019Document2 pagesPhysical Fitness Test Template 2019toffy luckNo ratings yet
- Nursing Care Plan For Insufficient Breast Milk ProductionDocument4 pagesNursing Care Plan For Insufficient Breast Milk ProductionHina FatimaNo ratings yet
- Mike Mentzer's Real Workout Routine & Diet PlanDocument14 pagesMike Mentzer's Real Workout Routine & Diet PlanPat100% (1)
- Class 12 Physical Education Revision Notes For Sports and Nutrition of Chapter 2Document14 pagesClass 12 Physical Education Revision Notes For Sports and Nutrition of Chapter 2yatishkewalramani123No ratings yet
- Sno G D&C f001 HiradcDocument5 pagesSno G D&C f001 HiradcTri SubaktiNo ratings yet
- Vi. The Product/Service Offering: Description, Evolution, and JustificationDocument5 pagesVi. The Product/Service Offering: Description, Evolution, and JustificationAlyn Gail LaodenioNo ratings yet
- PCRMDietary GuidelinesDocument42 pagesPCRMDietary GuidelinesSatyawira Aryawan DengNo ratings yet