You might also like
- Oral Wound Healing: Cell Biology and Clinical ManagementFrom EverandOral Wound Healing: Cell Biology and Clinical ManagementHannu LarjavaNo ratings yet
- Orthodontic Treatment Needs in Adolescents Aged 13-15 Years Using Orthodontic Treatment Needs IndicatorsDocument7 pagesOrthodontic Treatment Needs in Adolescents Aged 13-15 Years Using Orthodontic Treatment Needs IndicatorsTitis NlgNo ratings yet
- Pit & Fissure Sealant Power PointDocument40 pagesPit & Fissure Sealant Power PointDianita Rahma100% (1)
- Management of Pericoronitis of Newly-Erupted Permanent Tooth Using ElectrosurgeryDocument4 pagesManagement of Pericoronitis of Newly-Erupted Permanent Tooth Using ElectrosurgeryLatifa Hanif ZuhriNo ratings yet
- Vascular Anomalies PresentationDocument45 pagesVascular Anomalies PresentationMhinory OctNo ratings yet
- Penatalaksanaan Epulis Fibromatosa Dengan: ElectrosurgeryDocument5 pagesPenatalaksanaan Epulis Fibromatosa Dengan: ElectrosurgeryNada Syafa TitaniaNo ratings yet
- Pre-Prosthetic Alveoloplasty in A Diabetic Patient A CaseDocument3 pagesPre-Prosthetic Alveoloplasty in A Diabetic Patient A CaseMaria JabbarNo ratings yet
- Kista Rongga MulutDocument89 pagesKista Rongga MulutM Tauhid LestarioNo ratings yet
- Smoking Habits and Alcohol Consumption in Patients Diagnosed With Oral Lichen Planus: A Case ReportDocument17 pagesSmoking Habits and Alcohol Consumption in Patients Diagnosed With Oral Lichen Planus: A Case ReportkuntumNo ratings yet
- Tabel IotnDocument3 pagesTabel IotnPuspita PutriNo ratings yet
- Perawatan Saluran AkarDocument19 pagesPerawatan Saluran AkarBunga Erlita RosaliaNo ratings yet
- Clinical Applications of Biodentine in Pediatric Dentistry A Review Ofliterature 2332 0702 1000179 PDFDocument6 pagesClinical Applications of Biodentine in Pediatric Dentistry A Review Ofliterature 2332 0702 1000179 PDFZita AprilliaNo ratings yet
- Om Fix 2019Document281 pagesOm Fix 2019Sinta Gayatri100% (1)
- Identifikasi Bakteri Dental Plak Melalui Morfologi Koloni Dan PengecatanDocument19 pagesIdentifikasi Bakteri Dental Plak Melalui Morfologi Koloni Dan PengecatanfadilazahraNo ratings yet
- Geriatri EndodontikDocument4 pagesGeriatri EndodontikMeidi KurniaNo ratings yet
- Comparison of Two Treatment Modalities Operculectomy Vs Thirdmolar Removal For Management of PericoronitisDocument4 pagesComparison of Two Treatment Modalities Operculectomy Vs Thirdmolar Removal For Management of PericoronitisghinaNo ratings yet
- 1.1 Endodontik: HealingDocument52 pages1.1 Endodontik: HealingARINA KHAQ100% (1)
- Materi Tutor in EnglishDocument7 pagesMateri Tutor in EnglishDea RachnadewiNo ratings yet
- Keilitis Eksfoliatif JurnalDocument8 pagesKeilitis Eksfoliatif JurnalIbnu MuttaqinNo ratings yet
- Coronoplasty 2Document4 pagesCoronoplasty 2Befalia Aisarahmadani100% (1)
- 2019 Risk Factors For Caries Development in Primary Sjogren SyndromeDocument6 pages2019 Risk Factors For Caries Development in Primary Sjogren SyndromemrsilNo ratings yet
- Periodontics: Treatment Planning For Patients With Periodontal DiseasesDocument17 pagesPeriodontics: Treatment Planning For Patients With Periodontal Diseasesفاطمة فالح ضايف مزعلNo ratings yet
- Radiografi Fraktur Kedokteran GigiDocument16 pagesRadiografi Fraktur Kedokteran GigiFatimah Az-ZahrahNo ratings yet
- Bagi '18211 - Scenario in Englis3.docx'Document6 pagesBagi '18211 - Scenario in Englis3.docx'ithanur316No ratings yet
- Periodontal Charting and WorksheetDocument11 pagesPeriodontal Charting and Worksheetapi-3861216100% (6)
- TUTORIAL IN ENGLISH Blok 12Document7 pagesTUTORIAL IN ENGLISH Blok 12Ifata RDNo ratings yet
- Epulis FissuratumDocument9 pagesEpulis FissuratumDilaC.FareshaNo ratings yet
- Pdi Partial EdentulismDocument67 pagesPdi Partial EdentulismAnkeeta ShuklaNo ratings yet
- Brochure-Gc Fuji ViiDocument16 pagesBrochure-Gc Fuji ViiZulfahmi NurdinNo ratings yet
- 6 Daftar PustakaDocument1 page6 Daftar PustakaMaluvi KholilNo ratings yet
- Fissure TongueDocument2 pagesFissure Tonguebundahara zoomNo ratings yet
- Tes TLMDocument16 pagesTes TLMAmelia RosyidaNo ratings yet
- JurnalDocument10 pagesJurnalFranciscoXavierNo ratings yet
- Pengaruh Aplikasi Topical Dengan Larutan NaF Dan SnF2 Dalam Pencegahan Karies Ni Made Sirat JKG DenpasarDocument11 pagesPengaruh Aplikasi Topical Dengan Larutan NaF Dan SnF2 Dalam Pencegahan Karies Ni Made Sirat JKG DenpasarZaenuriNo ratings yet
- Erosive Lichen Planus of The Oral Cavity: A CaseDocument5 pagesErosive Lichen Planus of The Oral Cavity: A CaseFuad HasanNo ratings yet
- Tumor Rongga MulutDocument35 pagesTumor Rongga MulutMike DwitasariNo ratings yet
- Esthetic Restorative Treatment For Carious Anterior Teeth by GiomerDocument7 pagesEsthetic Restorative Treatment For Carious Anterior Teeth by GiomerFoysal Sirazee100% (1)
- Hidden CariesDocument10 pagesHidden Cariesyenni_windasariNo ratings yet
- Hasil Praktikum Saliva Dan OMR by L86Document16 pagesHasil Praktikum Saliva Dan OMR by L86Dewi Ni'maNo ratings yet
- SOCA Blok 12Document21 pagesSOCA Blok 12safiraNo ratings yet
- Pengaruh Aplikasi Topical Dengan Larutan NaF Dan SnF2 Dalam Pencegahan Karies Ni Made Sirat JKG Denpasar PDFDocument11 pagesPengaruh Aplikasi Topical Dengan Larutan NaF Dan SnF2 Dalam Pencegahan Karies Ni Made Sirat JKG Denpasar PDFZaenuriNo ratings yet
- Imunologi Jar Perio, Blok 9Document46 pagesImunologi Jar Perio, Blok 9Naviatul UlfaNo ratings yet
- Jurnal Amalgam TatoDocument2 pagesJurnal Amalgam TatoLu'luatul WidadNo ratings yet
- A Physiologic Impression Technique For Resorbed Mandibular Ridges PDFDocument3 pagesA Physiologic Impression Technique For Resorbed Mandibular Ridges PDFJyoti VermaNo ratings yet
- Extrinsic Stains and Deposits On TeethDocument9 pagesExtrinsic Stains and Deposits On TeethFredie Jun Onio100% (1)
- Crenated Tongue 2Document5 pagesCrenated Tongue 2Utami MayasariNo ratings yet
- CBL English Blok 7Document7 pagesCBL English Blok 7Ifata RDNo ratings yet
- Orthodontic PDFDocument40 pagesOrthodontic PDFOkyWndNo ratings yet
- 40 130 1 PBDocument4 pages40 130 1 PBrinaaa2000No ratings yet
- 1.dental CariesDocument12 pages1.dental CariesMatt NooriNo ratings yet
- Classification System For Full EdentulismDocument4 pagesClassification System For Full EdentulismmandakinimohanNo ratings yet
- Caustinerf Forte PDFDocument5 pagesCaustinerf Forte PDFLjubomirErdoglijaNo ratings yet
- Generalized Aggressive Periodontitis in Preschoolers: Report of A Case in A 3-1/2 Year OldDocument6 pagesGeneralized Aggressive Periodontitis in Preschoolers: Report of A Case in A 3-1/2 Year OldDyah Wulan RamadhaniNo ratings yet
- Abses IntraoralDocument19 pagesAbses IntraoralTitis LaraswatiNo ratings yet
- Amelogenesis ImperfectaDocument16 pagesAmelogenesis ImperfectaRajat Kansal100% (1)
- Penggunaan Polyethylene Fiber-Reinforced Composite Resin Sebagai Short Post Dan Inti Pada Gigi Anterior Sulung Dengan Karies Yang Luas Laporan KasusDocument14 pagesPenggunaan Polyethylene Fiber-Reinforced Composite Resin Sebagai Short Post Dan Inti Pada Gigi Anterior Sulung Dengan Karies Yang Luas Laporan Kasusfebriani serojaNo ratings yet
- Mucocele 8Document3 pagesMucocele 8Devi AlfianiNo ratings yet
- Lobular Capillary Hemangioma An Extremely Rare Entity in The Retromolar Region Case ReportDocument5 pagesLobular Capillary Hemangioma An Extremely Rare Entity in The Retromolar Region Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- V 7 Aop 191Document3 pagesV 7 Aop 191Sekar EkaperdanaNo ratings yet
- Retracted Oral HaemangiomaDocument5 pagesRetracted Oral Haemangiomaaulia lubisNo ratings yet
- Gingival Epulis: Report of Two Cases.: Dr. Praful Choudhari, Dr. Praneeta KambleDocument5 pagesGingival Epulis: Report of Two Cases.: Dr. Praful Choudhari, Dr. Praneeta KambleAnandNo ratings yet
- Cetak 4Document11 pagesCetak 4Rina NovitrianiNo ratings yet
- Cetak 3Document7 pagesCetak 3Rina NovitrianiNo ratings yet
- Announcement IGES 20 Juli-1 PDFDocument22 pagesAnnouncement IGES 20 Juli-1 PDFRina NovitrianiNo ratings yet
- Clinical Neurology and NeurosurgeryDocument5 pagesClinical Neurology and NeurosurgeryRina NovitrianiNo ratings yet
- Central Hemangioma A Case Report and Review of Lit PDFDocument5 pagesCentral Hemangioma A Case Report and Review of Lit PDFHamba AllahNo ratings yet
- 2014 Musculoskeletal Tumors and DiseasesDocument102 pages2014 Musculoskeletal Tumors and DiseasesNanda GemaNo ratings yet
- Choroidal HemangiomaDocument5 pagesChoroidal HemangiomaAgiu BogdanNo ratings yet
- Laryngeal Disorders: Julie G. Cebrian, MD, Dpbo-HnsDocument70 pagesLaryngeal Disorders: Julie G. Cebrian, MD, Dpbo-HnsEnharmonic MelodiesNo ratings yet
- Newborn Physical ExaminationDocument4 pagesNewborn Physical ExaminationastrikusumadewiNo ratings yet
- Walt-27 Years of Laser Treatment A Personal PerspectiveDocument18 pagesWalt-27 Years of Laser Treatment A Personal PerspectivedenmasasinggihNo ratings yet
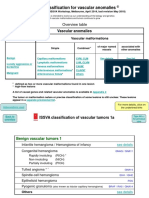
- ISSVA Classification 2018 PDFDocument20 pagesISSVA Classification 2018 PDFIgor YonekuraNo ratings yet
- Lasers Laser Like 2 PDFDocument14 pagesLasers Laser Like 2 PDFRidha Ramadina WidiatmaNo ratings yet
- Review Questions For SurgeryDocument32 pagesReview Questions For SurgeryNogra CarlNo ratings yet
- Journal Diagnosis and Management of A Tympanic Membrane HemangiomaDocument9 pagesJournal Diagnosis and Management of A Tympanic Membrane HemangiomaAndriyani YaniNo ratings yet
- Hemangioma Activity ScoreDocument6 pagesHemangioma Activity ScoreneonitesNo ratings yet
- Dermatofibroma: Aka Benign Fibrous HistiocytomaDocument4 pagesDermatofibroma: Aka Benign Fibrous HistiocytomafadoNo ratings yet
- PDF Lecture 9 Benign Soft Tissue TumorsDocument131 pagesPDF Lecture 9 Benign Soft Tissue TumorsMuhammad Rizqi100% (1)
- Liver Tumors - Epidemiology, Diagnosis, Prevention and Treatment (Helen Reeves)Document184 pagesLiver Tumors - Epidemiology, Diagnosis, Prevention and Treatment (Helen Reeves)JohnQNo ratings yet
- Hemangioma Propranolol GuidelineDocument2 pagesHemangioma Propranolol GuidelineSake Cinema21No ratings yet
- Issva Classification 2014 Final TrialDocument20 pagesIssva Classification 2014 Final TrialFrancis MunguíaNo ratings yet
- Liver MassDocument7 pagesLiver MassMarianne AlzagaNo ratings yet
- Review Article: The Spleen Revisited: An Overview On Magnetic Resonance ImagingDocument16 pagesReview Article: The Spleen Revisited: An Overview On Magnetic Resonance ImagingrusselioNo ratings yet
- 3a. Diseases of External NoseDocument90 pages3a. Diseases of External NoseKamal Saud100% (2)
- Birthmarks Identificationandmx201205ryanDocument4 pagesBirthmarks Identificationandmx201205ryanDanielcc LeeNo ratings yet
- Pathology of Blood VesselsDocument80 pagesPathology of Blood VesselsiqiqiqiqiqNo ratings yet
- Newborns Undergo Profound Physiologic Changes at The Moment of BirthDocument8 pagesNewborns Undergo Profound Physiologic Changes at The Moment of BirthUri ELNo ratings yet
- Benigntumorsofjaw2 130421054527 Phpapp01Document118 pagesBenigntumorsofjaw2 130421054527 Phpapp01orthomedNo ratings yet
- General Information: Signs/SymptomsDocument17 pagesGeneral Information: Signs/SymptomsColesniuc CostiNo ratings yet
- Daftar PustakaDocument5 pagesDaftar PustakaPramitha YustiaNo ratings yet
- Hemangioma - Google SearchDocument1 pageHemangioma - Google SearchhapidarrenNo ratings yet
- Benign Tumors of LarynxDocument48 pagesBenign Tumors of LarynxVilZan MominNo ratings yet
- Skin Nail HairDocument48 pagesSkin Nail HairkitsilcNo ratings yet
- Matary Clinical - 2013 (WWW - Afriqa Sat - Com)Document338 pagesMatary Clinical - 2013 (WWW - Afriqa Sat - Com)Ahmed Attia100% (1)