You might also like
- Family Names of DrugsDocument1 pageFamily Names of DrugsangelNo ratings yet
- Abdomen - FRCEM SuccessDocument275 pagesAbdomen - FRCEM SuccessAbin ThomasNo ratings yet
- Adrenergic Receptor ChartDocument1 pageAdrenergic Receptor ChartAnkit Mehta75% (4)
- EP - EngineDocument4 pagesEP - EngineAkhmad HasimNo ratings yet
- Guidelines Switching Antidepressants - A3 PDFDocument1 pageGuidelines Switching Antidepressants - A3 PDFP̷s̷ʏ̷ᴄ̷ʜ̷ᴏ̷ᴛ̷ɪ̷ᴄ̷ R̷ᴀ̷ɪ̷ɴ̷ʙ̷ᴏ̷ᴡ̷ᴢ̷50% (2)
- Veterinary Drugs - Usage, Dosage, Species, and More.Document15 pagesVeterinary Drugs - Usage, Dosage, Species, and More.cocopandanenakNo ratings yet
- Nclex Pharmacology (Drugs - Mostly Ask)Document4 pagesNclex Pharmacology (Drugs - Mostly Ask)KayayaDoclan100% (3)
- Mostly Ask Drugs On Nclex!Document4 pagesMostly Ask Drugs On Nclex!mjmm90No ratings yet
- 2 - Elements of Interior DesignDocument4 pages2 - Elements of Interior DesignYathaarth RastogiNo ratings yet
- Portfolio in Trainers Methodology (TM) Level 1: (Trainer/ Assessor)Document50 pagesPortfolio in Trainers Methodology (TM) Level 1: (Trainer/ Assessor)Shandz de RosasNo ratings yet
- Xii Neet Chemistry Mcqs PDFDocument30 pagesXii Neet Chemistry Mcqs PDFMarcus Rashford100% (3)
- Sradham ChecklistDocument9 pagesSradham ChecklistpswaminathanNo ratings yet
- Drug of ChoiceDocument43 pagesDrug of ChoiceJanna mae PatriarcaNo ratings yet
- Project On Stones & TilesDocument41 pagesProject On Stones & TilesMegha GolaNo ratings yet
- MS For Brick WorkDocument7 pagesMS For Brick WorkSumit OmarNo ratings yet
- Oncology Nursing HandoutsDocument7 pagesOncology Nursing HandoutsShandz de Rosas100% (1)
- Anticholinergics Study Drug ListDocument1 pageAnticholinergics Study Drug ListDrima Edi100% (1)
- Interactive Architecture Adaptive WorldDocument177 pagesInteractive Architecture Adaptive Worldhoma massihaNo ratings yet
- Communicable and Infectious Disease Nursing-NewDocument15 pagesCommunicable and Infectious Disease Nursing-NewShandz de RosasNo ratings yet
- FormulaDocument5 pagesFormulaShandz de RosasNo ratings yet
- Drugs World: Anti-PsychoticsDocument1 pageDrugs World: Anti-Psychoticsapi-26228251No ratings yet
- Pharm II Exam IDocument1 pagePharm II Exam IiburtenshawNo ratings yet
- SchizophreniaDocument1 pageSchizophreniaبراء طاهر حاتمNo ratings yet
- Addendum B: High Fall Risk MedicationsDocument3 pagesAddendum B: High Fall Risk MedicationspatientsafetyNo ratings yet
- Daftar ObatDocument1 pageDaftar ObatDhila ThasliyahNo ratings yet
- High Risk Medications ElderlyDocument2 pagesHigh Risk Medications ElderlyEman MohamedNo ratings yet
- Diploma Pembantu Perubatan: Tajuk: Antipsikotik & AntidepresiDocument3 pagesDiploma Pembantu Perubatan: Tajuk: Antipsikotik & AntidepresiazrulNo ratings yet
- Sedative-Hypnotic and Antipsychotic Drugs GuideDocument17 pagesSedative-Hypnotic and Antipsychotic Drugs GuideBijay Kumar MahatoNo ratings yet
- Manage Pain and Headaches in Cancer PatientsDocument12 pagesManage Pain and Headaches in Cancer PatientsMichiko_Lois_Tao_203No ratings yet
- Pharmacology NotesDocument9 pagesPharmacology NotesMayya FirdousNo ratings yet
- Warfarin Sodium: INR Levels 4.0 or Less Ok To Carry Out Procedure Test Atleast 72 Hrs Prior To ProcedureDocument6 pagesWarfarin Sodium: INR Levels 4.0 or Less Ok To Carry Out Procedure Test Atleast 72 Hrs Prior To ProcedureVimi GeorgeNo ratings yet
- Cytochrome P450 ChartDocument2 pagesCytochrome P450 ChartCristinaNo ratings yet
- Kelompok 2 - Tugas Obat PsikotropikaDocument11 pagesKelompok 2 - Tugas Obat Psikotropikamelin syafrianiNo ratings yet
- Commonly Prescribed Psychotropic Medications: Typical Antipsychotics TricyclicsDocument4 pagesCommonly Prescribed Psychotropic Medications: Typical Antipsychotics TricyclicssaraatifNo ratings yet
- PSYCHIATRIcsDocument11 pagesPSYCHIATRIcssaraNo ratings yet
- Daftar High Alert Dan LasaDocument6 pagesDaftar High Alert Dan LasaErin FatmawatiNo ratings yet
- Cytochrome P450 2D6 Known Drug Interaction Chart: Drugs Metabolized by CYP2D6 Enzyme Drug Inhibitors of CYP2D6 EnzymeDocument1 pageCytochrome P450 2D6 Known Drug Interaction Chart: Drugs Metabolized by CYP2D6 Enzyme Drug Inhibitors of CYP2D6 EnzymeSsNo ratings yet
- Benzodiazepine DatasheetDocument9 pagesBenzodiazepine DatasheetRico RodriguezNo ratings yet
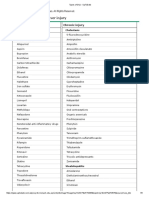
- Drugs Are Listed AlphabeticallyDocument17 pagesDrugs Are Listed AlphabeticallysyrieangelNo ratings yet
- PENGGOLONGAN OBAT PSIKOTROPIK DAN SEDIAAN OBAT ANTI-PSIKOSISDocument18 pagesPENGGOLONGAN OBAT PSIKOTROPIK DAN SEDIAAN OBAT ANTI-PSIKOSISMirzanNo ratings yet
- HW 2 Na 3Document7 pagesHW 2 Na 3Araw GabiNo ratings yet
- PSIKOFARMAKOLOGIDocument11 pagesPSIKOFARMAKOLOGIsayidaffanNo ratings yet
- Obat DepresiDocument14 pagesObat DepresiAnonymous 97fv5C0B7No ratings yet
- Bipolar MedicationsDocument1 pageBipolar Medicationsu8h99j80k9No ratings yet
- Long QT Drugs - Feb 22 2017 - AlternativesDocument2 pagesLong QT Drugs - Feb 22 2017 - Alternativesتوفيق البطرNo ratings yet
- Controlled Drugs: Schedules List (Updated November 2015) : Schedule 1Document3 pagesControlled Drugs: Schedules List (Updated November 2015) : Schedule 1RonfermNo ratings yet
- Formularium Obat RSDocument2 pagesFormularium Obat RSMyzard AriefNo ratings yet
- Formularium Obat RSDocument2 pagesFormularium Obat RSMyzard AriefNo ratings yet
- Copia Di Drugs That Cause or Prolong Delirium - UpToDateDocument2 pagesCopia Di Drugs That Cause or Prolong Delirium - UpToDateAFA.BLSNo ratings yet
- Types of DILI - Drug-Induced Liver InjuryDocument5 pagesTypes of DILI - Drug-Induced Liver InjuryDamian LiewNo ratings yet
- AnalgesicDocument2 pagesAnalgesicLA BriguelaNo ratings yet
- Effects of CYP450Document2 pagesEffects of CYP450CherylNo ratings yet
- Inhibitori, Inhibitorii Cresc: Substrat SubstraturileDocument4 pagesInhibitori, Inhibitorii Cresc: Substrat SubstraturileAlina CiugureanuNo ratings yet
- Label Nama Kotak ObatDocument3 pagesLabel Nama Kotak Obatkimia farma 14No ratings yet
- Mission & Vision: ProductsDocument5 pagesMission & Vision: Productsradheshyam882No ratings yet
- Cytochrome P450 3A Inhibitors and Inducers - UpToDateDocument2 pagesCytochrome P450 3A Inhibitors and Inducers - UpToDateioNo ratings yet
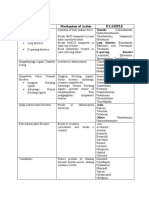
- Drug Class Mechanism of Action Example: ThiazideDocument2 pagesDrug Class Mechanism of Action Example: ThiazideLyod BalagasayNo ratings yet
- Commonly Prescribed Preferred Drugs: October 2015Document2 pagesCommonly Prescribed Preferred Drugs: October 2015iscariot02No ratings yet
- ตารางแสดงการแบ่งประเภท / Table of In Thailand: ว ัตถุออกฤทธิ์ Controlled Psychotropic SubstancesDocument1 pageตารางแสดงการแบ่งประเภท / Table of In Thailand: ว ัตถุออกฤทธิ์ Controlled Psychotropic SubstancesBeau PhatruetaiNo ratings yet
- Drugs That May Cause Mental ConfusionDocument2 pagesDrugs That May Cause Mental ConfusionohnoitsjohnnyNo ratings yet
- Pharmacology Classes MindMaps_230902_101709Document73 pagesPharmacology Classes MindMaps_230902_101709mouneeshkumar22No ratings yet
- Psychotherapeutic Drugs: Generic and Brand Names: Day 2 (Medication)Document3 pagesPsychotherapeutic Drugs: Generic and Brand Names: Day 2 (Medication)Ladybelle GototosNo ratings yet
- NCLEX Drugs 1 UpdatedDocument1 pageNCLEX Drugs 1 UpdatedSibel ErtuğrulNo ratings yet
- Common Drug Stems Cheat SheetDocument3 pagesCommon Drug Stems Cheat SheetRicky Vanguardia III100% (1)
- MECHANISM OF ACTION: ANTIDEPRESSANTS (Tricyclic Antidepressants)Document2 pagesMECHANISM OF ACTION: ANTIDEPRESSANTS (Tricyclic Antidepressants)ALIANA KIMBERLY MALQUESTONo ratings yet
- Psikotropika Obat Acuan PenggolonganDocument6 pagesPsikotropika Obat Acuan PenggolonganDwi PutriNo ratings yet
- FDA Pregnancy Category of Antidepressant MedicatioDocument2 pagesFDA Pregnancy Category of Antidepressant MedicatioJoshuaRobertoPratamaNo ratings yet
- 2 Pharma Drug ListsDocument5 pages2 Pharma Drug ListsDexie MaeNo ratings yet
- 2020 Safe List: Drugs That Are Considered To Be SAFE For Use in The Acute PorphyriasDocument2 pages2020 Safe List: Drugs That Are Considered To Be SAFE For Use in The Acute PorphyriasAlexandra LupuNo ratings yet
- Obat High Alert Kategori Resiko Tinggi: Rumah Sakit Aisyiyah ST - Khadijah Kabupaten PinrangDocument3 pagesObat High Alert Kategori Resiko Tinggi: Rumah Sakit Aisyiyah ST - Khadijah Kabupaten PinrangnadiraNo ratings yet
- Classification of Drugs Acting on the Autonomic Nervous System and CNSDocument15 pagesClassification of Drugs Acting on the Autonomic Nervous System and CNSAbdul SamadNo ratings yet
- Detecting Pressure Damage in People With Darkly Pigmented SkinDocument4 pagesDetecting Pressure Damage in People With Darkly Pigmented SkinShandz de RosasNo ratings yet
- How To Migrate To New Zeal LandDocument19 pagesHow To Migrate To New Zeal Landjoaf2003No ratings yet
- General InformationDocument5 pagesGeneral InformationShandz de RosasNo ratings yet
- ABG AnalysisDocument21 pagesABG Analysismrs_jrufusNo ratings yet
- Introduction to Palliative Care NursingDocument12 pagesIntroduction to Palliative Care NursingShandz de Rosas100% (1)
- NCM 103 Instructional PlanDocument5 pagesNCM 103 Instructional PlanShandz de Rosas100% (1)
- Cases Form 2007Document5 pagesCases Form 2007Shandz de RosasNo ratings yet
- Student Council Election Code (Final Copy)Document11 pagesStudent Council Election Code (Final Copy)Shandz de RosasNo ratings yet
- Introduction To Finite Element Methods (2001) (En) (489s)Document489 pagesIntroduction To Finite Element Methods (2001) (En) (489s)green77parkNo ratings yet
- Lesson 2 Socio Anthropological View of The SelfDocument12 pagesLesson 2 Socio Anthropological View of The SelfAilyn RamosNo ratings yet
- European GMP Annex 1 - 2008 Edition - 'Pmeasuring'Document3 pagesEuropean GMP Annex 1 - 2008 Edition - 'Pmeasuring'Khairul AnwarNo ratings yet
- Reinforced Concrete Beam DesignDocument13 pagesReinforced Concrete Beam Designmike smithNo ratings yet
- Detection and Attribution Methodologies Overview: Appendix CDocument9 pagesDetection and Attribution Methodologies Overview: Appendix CDinesh GaikwadNo ratings yet
- FP-XH PGRG eDocument936 pagesFP-XH PGRG ebvladimirov85No ratings yet
- Maureen L. Walsh - Re-Imagining Redemption. Universal Salvation in The Theology of Julian of NorwichDocument20 pagesMaureen L. Walsh - Re-Imagining Redemption. Universal Salvation in The Theology of Julian of NorwichAni LupascuNo ratings yet
- Troubleshooting Hydraulic Circuits: Fluid PowerDocument32 pagesTroubleshooting Hydraulic Circuits: Fluid PowerMi LuanaNo ratings yet
- Problem SolutionsDocument5 pagesProblem SolutionskkappaNo ratings yet
- Proceedings of The 16 TH WLCDocument640 pagesProceedings of The 16 TH WLCSabrinaNo ratings yet
- ROMUS 2012 Flooring CatalogueDocument20 pagesROMUS 2012 Flooring CatalogueDan George IIINo ratings yet
- Acuity Assessment in Obstetrical TriageDocument9 pagesAcuity Assessment in Obstetrical TriageFikriNo ratings yet
- F-16c.1 Ginkgo Ginkgolic AcidDocument2 pagesF-16c.1 Ginkgo Ginkgolic AcidNarongchai PongpanNo ratings yet
- Liquid Out, Temperature 25.5 °C Tube: M/gs P / WDocument7 pagesLiquid Out, Temperature 25.5 °C Tube: M/gs P / WGianra RadityaNo ratings yet
- JY Series Single-Phase Capacitor Induction MotorsDocument1 pageJY Series Single-Phase Capacitor Induction MotorsAditya PrasetyoNo ratings yet
- Life of A Landfill PumpDocument50 pagesLife of A Landfill PumpumidNo ratings yet
- Sap ThufingteDocument10 pagesSap ThufingtehangsinfNo ratings yet
- Fake News Poems by Martin Ott Book PreviewDocument21 pagesFake News Poems by Martin Ott Book PreviewBlazeVOX [books]No ratings yet
- Front Wheel Steering System With Movable Hedlights Ijariie5360Document6 pagesFront Wheel Steering System With Movable Hedlights Ijariie5360Ifra KhanNo ratings yet
- Lec9-Rock Cutting ToolsDocument35 pagesLec9-Rock Cutting ToolsAmraha NoorNo ratings yet
- IEQ CompleteDocument19 pagesIEQ Completeharshal patilNo ratings yet
- Pitch Manual SpecializedDocument20 pagesPitch Manual SpecializedRoberto Gomez100% (1)