You might also like
- Under the Medical Gaze: Facts and Fictions of Chronic PainFrom EverandUnder the Medical Gaze: Facts and Fictions of Chronic PainNo ratings yet
- The Politics of Pain Medicine: A Rhetorical-Ontological InquiryFrom EverandThe Politics of Pain Medicine: A Rhetorical-Ontological InquiryNo ratings yet
- The Story Within: Personal Essays on Genetics and IdentityFrom EverandThe Story Within: Personal Essays on Genetics and IdentityRating: 5 out of 5 stars5/5 (3)
- God's Laboratory: Assisted Reproduction in the AndesFrom EverandGod's Laboratory: Assisted Reproduction in the AndesNo ratings yet
- Joseph Kearney and the Hunt for Rommel: The Life of a Newfoundland CommandoFrom EverandJoseph Kearney and the Hunt for Rommel: The Life of a Newfoundland CommandoNo ratings yet
- (Exploring Psycho-Social Studies) Farhad Dalal - Thought Paralysis - The Virtues of Discrimination (2011, Karnac Books)Document271 pages(Exploring Psycho-Social Studies) Farhad Dalal - Thought Paralysis - The Virtues of Discrimination (2011, Karnac Books)Ivana ŠalinovićNo ratings yet
- Death and The InternetDocument563 pagesDeath and The Internetorj78No ratings yet
- Excoriation (Skin Picking Disorder or Dermatillomania) : Diagnostic Criteria According To DSM VDocument5 pagesExcoriation (Skin Picking Disorder or Dermatillomania) : Diagnostic Criteria According To DSM VZarghoona inayatNo ratings yet
- Schizoobsessive Spectrum Disorders An UpdateDocument15 pagesSchizoobsessive Spectrum Disorders An UpdateRubiNo ratings yet
- Finkelhor1986 Risk Factors Child Sexual Abuse-DikonversiDocument29 pagesFinkelhor1986 Risk Factors Child Sexual Abuse-DikonversinurindahNo ratings yet
- Philosophy of DisabilityDocument5 pagesPhilosophy of DisabilityJorge OrozcoNo ratings yet
- RD Laing QuotesDocument3 pagesRD Laing QuotesSergio S. DolcemascoloNo ratings yet
- Ace Inclusive Sex EdDocument2 pagesAce Inclusive Sex Ed- Zack -No ratings yet
- Phillip L. Hammack, Bertram J. Cohler - The Story of Sexual Identity - Narrative Perspectives On The Gay and Lesbian Life Course-Oxford University Press, USA (2009)Document497 pagesPhillip L. Hammack, Bertram J. Cohler - The Story of Sexual Identity - Narrative Perspectives On The Gay and Lesbian Life Course-Oxford University Press, USA (2009)Ildikó HomaNo ratings yet
- Disability PsychoanalysisDocument7 pagesDisability Psychoanalysisadheena simonNo ratings yet
- Neurotic Styles. David ShapiroDocument2 pagesNeurotic Styles. David ShapiroRaquel CadenasNo ratings yet
- Richard Feynman Physics QuotesDocument2 pagesRichard Feynman Physics QuotesSpam SpamNo ratings yet
- Zenana: Everyday Peace in A Karachi Apartment Building - Chapter 4Document26 pagesZenana: Everyday Peace in A Karachi Apartment Building - Chapter 4Voices and Visions ProjectNo ratings yet
- Medicine As An Institution of Social ControlDocument19 pagesMedicine As An Institution of Social ControlClaudio Gruber MannNo ratings yet
- Moving Beyond Cognitive Behaviour Therapy - The PsychologistDocument5 pagesMoving Beyond Cognitive Behaviour Therapy - The PsychologistVarsha VivekanandanNo ratings yet
- 03 Dryden & Branch CH 02Document20 pages03 Dryden & Branch CH 02gazellehouse8259100% (1)
- Therapist's Guide to Posttraumatic Stress Disorder InterventionFrom EverandTherapist's Guide to Posttraumatic Stress Disorder InterventionNo ratings yet
- Projective Psychology - Clinical Approaches To The Total PersonalityFrom EverandProjective Psychology - Clinical Approaches To The Total PersonalityNo ratings yet
- Third Wave Rise of Process Based CareDocument2 pagesThird Wave Rise of Process Based CareSidarta RodriguesNo ratings yet
- Science and Morality in Medicine: A Survey of Medical EducatorsFrom EverandScience and Morality in Medicine: A Survey of Medical EducatorsNo ratings yet
- Herbert y Gaudiano (2013) : The Importance of Theory in Cognitive Behavior Therapy: A Perspective of Contextual Behavioral ScienceDocument12 pagesHerbert y Gaudiano (2013) : The Importance of Theory in Cognitive Behavior Therapy: A Perspective of Contextual Behavioral SciencePablo Valencia MeléndezNo ratings yet
- One Problem, Two Solutions. A Comparison Between Cognitive-Behavioral Therapy and Psychoanalytic TherapyDocument6 pagesOne Problem, Two Solutions. A Comparison Between Cognitive-Behavioral Therapy and Psychoanalytic TherapyPablo SavinaNo ratings yet
- Clark PDFDocument8 pagesClark PDFEuge López RuizNo ratings yet
- Research in Psychotherapy and CounsellingFrom EverandResearch in Psychotherapy and CounsellingRating: 3 out of 5 stars3/5 (3)
- 1949 Eysenck - Training in Clinical Psychology An English Point ofDocument4 pages1949 Eysenck - Training in Clinical Psychology An English Point ofyolanda sanchezNo ratings yet
- Journal of Cognitive and Behavioral Psychotherapies Descarts Daniel David-With-Cover-Page-V2Document12 pagesJournal of Cognitive and Behavioral Psychotherapies Descarts Daniel David-With-Cover-Page-V2Anna Thallita AraujoNo ratings yet
- The Great Psychotherapy Debate PDFDocument223 pagesThe Great Psychotherapy Debate PDFJorge Rojas GNo ratings yet
- Hayes Et Al (2018) - Process-Based CBT.Document57 pagesHayes Et Al (2018) - Process-Based CBT.leidy7No ratings yet
- Brandon A. Gaudiano - Incorporating Acceptance and Mindfulness Into The Treatment of Psychosis - Current Trends and Future Directions (2015, Oxford University Press)Document305 pagesBrandon A. Gaudiano - Incorporating Acceptance and Mindfulness Into The Treatment of Psychosis - Current Trends and Future Directions (2015, Oxford University Press)Vartax100% (2)
- An Integrative Paradigm for Mental Health Care: Ideas and Methods Shaping the FutureFrom EverandAn Integrative Paradigm for Mental Health Care: Ideas and Methods Shaping the FutureNo ratings yet
- Reality Therapy: A New Approach to PsychiatryFrom EverandReality Therapy: A New Approach to PsychiatryRating: 3.5 out of 5 stars3.5/5 (31)
- Self System Therapy For Depression Therapist Guide 1St Edition Kari M Eddington Full Download ChapterDocument51 pagesSelf System Therapy For Depression Therapist Guide 1St Edition Kari M Eddington Full Download Chapterolive.phelps477100% (12)
- Troubled Bodies: Critical Perspectives on Postmodernism, Medical Ethics, and the BodyFrom EverandTroubled Bodies: Critical Perspectives on Postmodernism, Medical Ethics, and the BodyNo ratings yet
- The Great Psychotherapy Debate PDFDocument223 pagesThe Great Psychotherapy Debate PDFCasey Lewis100% (9)
- Blackledge - Linking Basic To Applied PsychoterapeuticDocument33 pagesBlackledge - Linking Basic To Applied Psychoterapeuticpalomazul007No ratings yet
- An Introduction To Cognitive Behavioural Therapy Skills and Applications David Westbrook Helen Kennerley and Joan Kirk London Sage Publications 2007 PP 296 1999 PB Isbn 141290840xDocument3 pagesAn Introduction To Cognitive Behavioural Therapy Skills and Applications David Westbrook Helen Kennerley and Joan Kirk London Sage Publications 2007 PP 296 1999 PB Isbn 141290840xDini Fajariani0% (1)
- Why Cognitive Behavioral Therapy - Dah Highlight PDFDocument2 pagesWhy Cognitive Behavioral Therapy - Dah Highlight PDFthepanicdollsNo ratings yet
- Psychology Worlds Issue 13: CBT For Anxiety A Clinical Psychology Introduction To Cognitive Behavioural Therapy For Anxiety Disorders: Psychology Worlds, #13From EverandPsychology Worlds Issue 13: CBT For Anxiety A Clinical Psychology Introduction To Cognitive Behavioural Therapy For Anxiety Disorders: Psychology Worlds, #13No ratings yet
- Speed Et Al-2017-Clinical Psychology Science and PracticeDocument20 pagesSpeed Et Al-2017-Clinical Psychology Science and PracticeN SINDHU 2237406No ratings yet
- Mental Health, Psychiatric Disorders, and the Implications of Long COVID-19: A View of Traditional Chinese MedicineFrom EverandMental Health, Psychiatric Disorders, and the Implications of Long COVID-19: A View of Traditional Chinese MedicineNo ratings yet
- Living Systems Information Therapy LSIT: Introduction to Quantum MedicineFrom EverandLiving Systems Information Therapy LSIT: Introduction to Quantum MedicineNo ratings yet
- What Do Others Think The Why When and How of Using Surveys in CBTDocument11 pagesWhat Do Others Think The Why When and How of Using Surveys in CBTANGELICANo ratings yet
- Behavior EpigeneticsDocument10 pagesBehavior EpigeneticsVinicius SiqueiraNo ratings yet
- Sample Chapter of THE WORLD OF PSYCHOLOGYDocument45 pagesSample Chapter of THE WORLD OF PSYCHOLOGYVinicius SiqueiraNo ratings yet
- Vulnerablility CycleDocument21 pagesVulnerablility CycleVinicius SiqueiraNo ratings yet
- Rethinking Autism - From Social Awkwardness To Social Creativity - Behavioral ScientistDocument6 pagesRethinking Autism - From Social Awkwardness To Social Creativity - Behavioral ScientistVinicius Siqueira100% (1)
- Richards (1974) The Integration of A Child Into A Social World PDFDocument336 pagesRichards (1974) The Integration of A Child Into A Social World PDFVinicius SiqueiraNo ratings yet
- We Have But One LifeDocument10 pagesWe Have But One LifeVinicius SiqueiraNo ratings yet
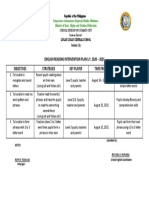
- English Reading Intervention Plan S.Y. 2020 - 2021 Objectives Strategies Key Player Time Frame Expected OutputDocument1 pageEnglish Reading Intervention Plan S.Y. 2020 - 2021 Objectives Strategies Key Player Time Frame Expected OutputMaribel A. BustilloNo ratings yet
- Test Paper: Put The Verbs in Brackets Into Present Perfect Simple Affirmative. (20p)Document2 pagesTest Paper: Put The Verbs in Brackets Into Present Perfect Simple Affirmative. (20p)Simona Elena MosinaNo ratings yet
- Comparative Adjectives - More Fewer and LessDocument5 pagesComparative Adjectives - More Fewer and LessSolange YánezNo ratings yet
- Communication Skills Class 9Document14 pagesCommunication Skills Class 9Aweaker Tangix100% (2)
- Past Progressive Tense: Corporación Colegio República Del Niño - Corporeni ProceedingDocument4 pagesPast Progressive Tense: Corporación Colegio República Del Niño - Corporeni ProceedingIván Darío Jáuregui DuránNo ratings yet
- Intrinsic Element of LiteratureDocument6 pagesIntrinsic Element of LiteratureYudhi Putrawan100% (1)
- Vocabulary Development 2Document21 pagesVocabulary Development 2Adila WaheedaNo ratings yet
- Week 6 - Interpersonal and Negotiation SkillsDocument25 pagesWeek 6 - Interpersonal and Negotiation SkillsIodanutzs UkNo ratings yet
- TP1 PDFDocument323 pagesTP1 PDFDragana ĆorićNo ratings yet
- Ea Rizki Function of Slang WordDocument78 pagesEa Rizki Function of Slang WordIntan MaharaniNo ratings yet
- Present SimpleDocument4 pagesPresent SimpleRonald Y. BarazarteNo ratings yet
- Romanian and The Balkans: Some Comparative PerspectivesDocument23 pagesRomanian and The Balkans: Some Comparative PerspectivesGeorge IonașcuNo ratings yet
- Top 3 Models of Semantic MemoryDocument7 pagesTop 3 Models of Semantic Memoryaaminafarooq321No ratings yet
- Lo5. Contribute To Workplace InnovationDocument6 pagesLo5. Contribute To Workplace Innovationrobelyn veranoNo ratings yet
- WalkerrDocument24 pagesWalkerrMercedes FerrandoNo ratings yet
- Worksheet 10Document18 pagesWorksheet 10Nurdiansyah Drinush AudacieuxNo ratings yet
- Book Effective Teaching and Learning English For Spesific PURPOSE - PDFDocument117 pagesBook Effective Teaching and Learning English For Spesific PURPOSE - PDFAbdulghafur HadengNo ratings yet
- Qdoc - Tips Lukejermay-VibrationspdfDocument116 pagesQdoc - Tips Lukejermay-VibrationspdfSunny Gujjar100% (4)
- Identification of Noun, Adjective, Verb, Adverb 2 For PDFDocument22 pagesIdentification of Noun, Adjective, Verb, Adverb 2 For PDFmukeshNo ratings yet
- Quotes of Einstein PDFDocument3 pagesQuotes of Einstein PDFjagdeep_sekhon100% (2)
- Principles of Management - Course OutlineDocument3 pagesPrinciples of Management - Course OutlineMuhammad Salman Rasheed100% (2)
- QFT Ideas From Google DocsDocument2 pagesQFT Ideas From Google Docsapi-137669263No ratings yet
- Psychoanalytic Process Research StrategiesDocument378 pagesPsychoanalytic Process Research StrategiesbrthstNo ratings yet
- DivergenceDocument320 pagesDivergenceSofia100% (1)
- YORUBA STUDYS - ch5 PDFDocument28 pagesYORUBA STUDYS - ch5 PDFAsogun Falcão T'ogúnNo ratings yet
- How To Write A ReportDocument6 pagesHow To Write A ReportDARIA DINCĂNo ratings yet
- Celpip Basic IntroductionDocument2 pagesCelpip Basic IntroductionDeepshikha GautamNo ratings yet
- HOUSEKEEPING - WEEK 1 UpdatedDocument5 pagesHOUSEKEEPING - WEEK 1 UpdatedMaria Rizza IlaganNo ratings yet
- Types of ListeningDocument2 pagesTypes of ListeningShafira Vidiastri100% (1)