You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Surviving Sepsis Campaign International.21Document81 pagesSurviving Sepsis Campaign International.21jamesteryNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Dolor Torácico JACC 2021Document99 pagesDolor Torácico JACC 2021Ricardo CastañedaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Lista de Enfermedades Raras OrphanetDocument176 pagesLista de Enfermedades Raras OrphanetbrianNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Recording A 12-Lead Electrocardiogram (ECG)Document4 pagesRecording A 12-Lead Electrocardiogram (ECG)brianNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Osong Public Health and Research PerspectivesDocument6 pagesOsong Public Health and Research PerspectivesbrianNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- European Journal of Internal Medicine-1Document6 pagesEuropean Journal of Internal Medicine-1brianNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Ann Burns and Fire Disasters 26 12Document4 pagesAnn Burns and Fire Disasters 26 12brianNo ratings yet
- Suros PDFDocument1,163 pagesSuros PDFMiguel GonzálezNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- L60000984 Ficha PDFDocument1 pageL60000984 Ficha PDFbrianNo ratings yet
- A List of The Approved Journals PDFDocument672 pagesA List of The Approved Journals PDFNasser AmmarNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Prepared By:: Kezia Queen G. Espia RM, RPHDocument19 pagesPrepared By:: Kezia Queen G. Espia RM, RPHLuna ScorpiusNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Probiotik Clinical Applications in Gastrointestinal DiseaseDocument29 pagesProbiotik Clinical Applications in Gastrointestinal DiseaseDwi Feri HariyantoNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
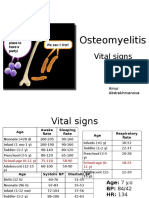
- PBL 2 - OsteomyelitisDocument10 pagesPBL 2 - OsteomyelitisAinur AbdrakhmanovaNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Early Diagnosis of Sepsis Using Serum Bio MarkersDocument5 pagesEarly Diagnosis of Sepsis Using Serum Bio Markersalemarques16No ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- A Thesis Submitted in Partial Fulfilment of The Requirements of Kingston University For The Degree of Doctor of PhilosophyDocument271 pagesA Thesis Submitted in Partial Fulfilment of The Requirements of Kingston University For The Degree of Doctor of PhilosophyArtemio Jr A LonzagaNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- AnthraxDocument2 pagesAnthraxAmon Jnr KamungarangaNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Pembuatan DMSODocument12 pagesPembuatan DMSORyan Heri GunawanNo ratings yet
- Nipah Virus Infection: ImportanceDocument9 pagesNipah Virus Infection: ImportanceSivaNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Microbiology and Immunology Pokhara University Syllabus NOCDocument2 pagesMicrobiology and Immunology Pokhara University Syllabus NOCDinesh SubediNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Mycoplasma Genitalium A4Document1 pageMycoplasma Genitalium A4Nauli NasirNo ratings yet
- Materi Bu CostiDocument36 pagesMateri Bu CostitriaNo ratings yet
- HEPADNAVIRIDAEDocument14 pagesHEPADNAVIRIDAEnur qistina humaira zulkarshamsiNo ratings yet
- Specimen Collection & ProcessingDocument23 pagesSpecimen Collection & ProcessingRobie LeañoNo ratings yet
- Lecture 3 Laboratory Diagnosis of Viral InfectionDocument85 pagesLecture 3 Laboratory Diagnosis of Viral InfectionNedhal Mahmoud KaleefahNo ratings yet
- (1980) Approved Lists of Bacterial NamesDocument196 pages(1980) Approved Lists of Bacterial NamesLeonardo LopesNo ratings yet
- Difference of Broad Spectrum & Narrow Spectrum AntibioticsDocument36 pagesDifference of Broad Spectrum & Narrow Spectrum AntibioticsAFTAB H. ABBASINo ratings yet
- Uji Total Plate Count TPC Bakteri Pada Minuman TehDocument8 pagesUji Total Plate Count TPC Bakteri Pada Minuman TehNanda Rizki UtamiNo ratings yet
- 1 Structure and Identification of Bacteria 2014 2 1 PDFDocument74 pages1 Structure and Identification of Bacteria 2014 2 1 PDFKaleem AfridiNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Tarun MeenaDocument59 pagesTarun Meenapiyushjakhar05No ratings yet
- Putting On and Removing Ppe Diagram - March 2020Document2 pagesPutting On and Removing Ppe Diagram - March 2020Perdana DialisisNo ratings yet
- Microbiology NotesDocument14 pagesMicrobiology Notesapi-264004571No ratings yet
- Adenovirus InfectionDocument2 pagesAdenovirus InfectionRoxanne HarmerNo ratings yet
- MCQS MMDocument45 pagesMCQS MMAyesha .No ratings yet
- A New Method For Determining The Minimum Inhibitory Concentration of Essential OilsDocument7 pagesA New Method For Determining The Minimum Inhibitory Concentration of Essential OilsKalpanaNo ratings yet
- Infection Control: The New York RequirementDocument3 pagesInfection Control: The New York RequirementLiezel100% (1)
- Management of Feline Idiopathic Cystitis (FIC) Using Probiotic Combination TreatmentDocument4 pagesManagement of Feline Idiopathic Cystitis (FIC) Using Probiotic Combination TreatmentMelita Nono LebangNo ratings yet
- Biology Ebola Virus Project ReportDocument19 pagesBiology Ebola Virus Project ReportChaitaneyMorNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormBabiejoy Beltran AceloNo ratings yet
- Medical Microbiology For GraduatesDocument64 pagesMedical Microbiology For Graduatestummalapalli venkateswara rao100% (1)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)