You might also like
- Guest Cycle Video Script-FoDocument5 pagesGuest Cycle Video Script-Fovkook luv100% (2)
- Medical BillDocument8 pagesMedical Billsarveshfdk48No ratings yet
- Solina - 2ndyr - 1sttermDocument1 pageSolina - 2ndyr - 1sttermEduard Keandrei Yap SolinaNo ratings yet
- Generated Schedule and Assessment: Malayan Colleges LagunaDocument1 pageGenerated Schedule and Assessment: Malayan Colleges LagunaVince Alvin DaquizNo ratings yet
- 1Document1 page1Katleen Joy VillacinNo ratings yet
- Achmat Ripai MK Pengantar S & KBDocument1 pageAchmat Ripai MK Pengantar S & KBFrashaNo ratings yet
- Date Location KM Amount Off-Home 7 4.55 Off-Home 7 4.55 Off-Sjkt (M) - Off 12 7.8 Off-Home 7 4.55 Off-Home-Off 14 9.1 Off-Home 7 4.55Document5 pagesDate Location KM Amount Off-Home 7 4.55 Off-Home 7 4.55 Off-Sjkt (M) - Off 12 7.8 Off-Home 7 4.55 Off-Home-Off 14 9.1 Off-Home 7 4.55Santhiya PerisamyNo ratings yet
- Flight Tickets@NovFlnDocument2 pagesFlight Tickets@NovFlnBhavani reddyNo ratings yet
- Megawide GMR Construction JV, Inc.: Manpower Supply For Civil Structural WorksDocument1 pageMegawide GMR Construction JV, Inc.: Manpower Supply For Civil Structural WorksChristian Jay ValdezNo ratings yet
- Ease My Trip PDF Air TicketDocument3 pagesEase My Trip PDF Air TicketBhavani reddyNo ratings yet
- Adobe Scan 24 Jun 2023Document2 pagesAdobe Scan 24 Jun 2023sanilNo ratings yet
- Amara Raja Group of Companies: Vamsi Manoj Veerubhotla 3000893 Engineer Grade:M10 4AMDocument1 pageAmara Raja Group of Companies: Vamsi Manoj Veerubhotla 3000893 Engineer Grade:M10 4AMVamsi ManojNo ratings yet
- Creshella Mharee PDFDocument1 pageCreshella Mharee PDFMc ZapantaNo ratings yet
- Payroll: Informatic Computer Institute of Agusan Del SurDocument4 pagesPayroll: Informatic Computer Institute of Agusan Del SurJulius SalasNo ratings yet
- Fees PaidDocument3 pagesFees Paidunsocialized.psychopathNo ratings yet
- Luciano, Elmer O Payslip: Netpay 5,987.87Document1 pageLuciano, Elmer O Payslip: Netpay 5,987.87elmer lucianoNo ratings yet
- Nader Osman TicketDocument3 pagesNader Osman TicketJITHIN JAYARAMNo ratings yet
- University of Southern Mindanao: Pre-Registration/Assessment FormDocument1 pageUniversity of Southern Mindanao: Pre-Registration/Assessment Formlouise ann marie reyesNo ratings yet
- Jamshedpur ExpstmtDocument2 pagesJamshedpur ExpstmtRahul PalNo ratings yet
- Appendix A Blank 1Document3 pagesAppendix A Blank 1Zyrah HolandaNo ratings yet
- Republic of The Philippines Mariano Marcos State University Ilocos Norte Certificate of RegistrationDocument1 pageRepublic of The Philippines Mariano Marcos State University Ilocos Norte Certificate of RegistrationLovryan Tadena AmilingNo ratings yet
- Certificate of RegistrationDocument1 pageCertificate of RegistrationVan DagandalNo ratings yet
- TrabajoDocument1 pageTrabajodarylbocanegraNo ratings yet
- Mode of Payment: FULL Total Amount Due Today: 15,648.30: Our Lady of Perpetual Succor CollegeDocument1 pageMode of Payment: FULL Total Amount Due Today: 15,648.30: Our Lady of Perpetual Succor CollegeJoaquin LPNo ratings yet
- Ded Daha SelatanDocument25 pagesDed Daha Selatanindroarifianto_11871No ratings yet
- Employee ExpenseDocument2 pagesEmployee Expenseanon-465051100% (2)
- Salary Pay Slip - Aug23Document1 pageSalary Pay Slip - Aug23TENDER AWADH GROUPNo ratings yet
- Rivulis Irrigation India Private Limited Field Expenses StatementDocument2 pagesRivulis Irrigation India Private Limited Field Expenses StatementSayeed AhmadNo ratings yet
- Europe Itiv2Document42 pagesEurope Itiv2Wani FuziNo ratings yet
- Rumah t90Document1 pageRumah t90Danang DwinNo ratings yet
- Rundown Workshop Capital Allocation - OldDocument1 pageRundown Workshop Capital Allocation - Oldendro suendroNo ratings yet
- Pegalan, Jay Pactol (2014-104613) 2020-1SDocument1 pagePegalan, Jay Pactol (2014-104613) 2020-1SCj LlemosNo ratings yet
- Visayas State University: Certificate of RegistrationDocument1 pageVisayas State University: Certificate of RegistrationRamon Muscat Jr.No ratings yet
- ACCA CAT 2010 JanuaryDocument4 pagesACCA CAT 2010 JanuarycityproeducareNo ratings yet
- Site Plan: Property LineDocument3 pagesSite Plan: Property LinekarenNo ratings yet
- KoniaDocument2 pagesKoniaNguwruw Chungpha MoyonNo ratings yet
- Berthing Plan Chart (B. Timur) : BjtiportDocument3 pagesBerthing Plan Chart (B. Timur) : BjtiportAswinanda CKNo ratings yet
- Assessment Form: LGU SubsidyDocument1 pageAssessment Form: LGU SubsidyHhhhhNo ratings yet
- Assessment Form: LGU SubsidyDocument1 pageAssessment Form: LGU SubsidyHhhhhNo ratings yet
- Date Item Quantity Unit Price Remarks Bill Shop Name Descriptio N Total PriceDocument2 pagesDate Item Quantity Unit Price Remarks Bill Shop Name Descriptio N Total Priceelena estellaNo ratings yet
- CDR October 2018Document24 pagesCDR October 2018Marcy Delfino AcabNo ratings yet
- Assessment Form: LGU SubsidyDocument1 pageAssessment Form: LGU SubsidyHhhhhNo ratings yet
- SOR GCC SOR 1516 1 Catchpits CleaningDocument1 pageSOR GCC SOR 1516 1 Catchpits CleaningLift carry LapsittingNo ratings yet
- 2nd Year Registration FormDocument1 page2nd Year Registration FormLourie BaslotNo ratings yet
- Dheeraj Fee ReceiptDocument1 pageDheeraj Fee Receiptdepoortereeefje23No ratings yet
- Road,: LGG?L Tr4lrqfer 9areoDocument1 pageRoad,: LGG?L Tr4lrqfer 9areoSamith AnuruddhaNo ratings yet
- Course Flowchart: AssessmentDocument2 pagesCourse Flowchart: AssessmentJeasmine Andrea Diane PayumoNo ratings yet
- H.D.jain College, Ara, Bhojpur, Bihar SEM-4Document3 pagesH.D.jain College, Ara, Bhojpur, Bihar SEM-4Raj SinghNo ratings yet
- Bmi Expense Report (Mar. 02-07, 2020)Document1 pageBmi Expense Report (Mar. 02-07, 2020)Henzon Gregor TronoNo ratings yet
- Piccio, Charlaine Mae Gaoat (2014-101663) 2020-1SDocument1 pagePiccio, Charlaine Mae Gaoat (2014-101663) 2020-1SCj LlemosNo ratings yet
- Berthing Plan Chart (B. Timur) : BjtiportDocument3 pagesBerthing Plan Chart (B. Timur) : BjtiportAris FathoniNo ratings yet
- Republic of The Philippines Mariano Marcos State University Ilocos Norte Certificate of RegistrationDocument2 pagesRepublic of The Philippines Mariano Marcos State University Ilocos Norte Certificate of Registrationbarry alejandroNo ratings yet
- LIQUIDATIONDocument6 pagesLIQUIDATIONW-DASMARINAS PWR SALESNo ratings yet
- REVISED APP 2022 - Quarter 4Document3 pagesREVISED APP 2022 - Quarter 4EVELYN PASANANo ratings yet
- 1 10000Document1 page1 10000Dana Ștefania SmarandaNo ratings yet
- Expense Report of Tambuscio AlbertoDocument9 pagesExpense Report of Tambuscio AlbertoAlberto TambuscioNo ratings yet
- Yuran Program Master UNISHAMSDocument1 pageYuran Program Master UNISHAMSman_daineseNo ratings yet
- Amante, John Patrick Angulo (2014-104987) 2020-1SDocument1 pageAmante, John Patrick Angulo (2014-104987) 2020-1SCj LlemosNo ratings yet
- Mah State Sixth Pay CalculaterDocument4 pagesMah State Sixth Pay CalculaternitinyeshwantNo ratings yet
- Cost/pax (8 Paying Participants) 1,674.38: Projected Cost/Revenue DSB - Campuestohan - Ruins TourDocument1 pageCost/pax (8 Paying Participants) 1,674.38: Projected Cost/Revenue DSB - Campuestohan - Ruins TourJong PerrarenNo ratings yet
- MailerDocument140 pagesMailerlikeredd100% (1)
- TRAVELLINGDocument2 pagesTRAVELLINGSylwiaNo ratings yet
- Enchanting Himachal 06 Nights & 07 DaysDocument6 pagesEnchanting Himachal 06 Nights & 07 DaysTravis BickleNo ratings yet
- TM Elec 6-Module1Document55 pagesTM Elec 6-Module1Nimb MaximmNo ratings yet
- West CotDocument3 pagesWest Cotalbert DominguezNo ratings yet
- Louisiana Warn NoticeDocument8 pagesLouisiana Warn Noticethe kingfishNo ratings yet
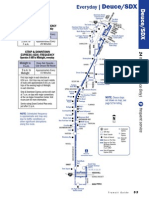
- 7 A.M. To 2 A.M. 2 A.M. To 7 A.m.: Deuce On The Strip Frequency Operates 24 Hours A Day, EverydayDocument2 pages7 A.M. To 2 A.M. 2 A.M. To 7 A.m.: Deuce On The Strip Frequency Operates 24 Hours A Day, EverydayTxavitoNo ratings yet
- UNIT 2 Mystery Box TemplateDocument77 pagesUNIT 2 Mystery Box TemplateĐỗ Ngọc Mỹ NhiNo ratings yet
- 00000053-Portofino Brochure (Compressed)Document27 pages00000053-Portofino Brochure (Compressed)Abed OsmanNo ratings yet
- Pagina 96Document3 pagesPagina 96registrosNo ratings yet
- Ramada Brand BookDocument9 pagesRamada Brand BookMX EARNNo ratings yet
- Research Methods For Architecture: Ar. Moncres TojeDocument32 pagesResearch Methods For Architecture: Ar. Moncres TojeRoseanne CarsolaNo ratings yet
- UntitledDocument12 pagesUntitledJabeth IbarraNo ratings yet
- Buisness Hotel at BKC, MumbaiDocument23 pagesBuisness Hotel at BKC, MumbaiSakhi BahetiNo ratings yet
- Hotel Voucher For Mr. Robin Resplandor & PtyDocument2 pagesHotel Voucher For Mr. Robin Resplandor & PtyPaul Kristian CanlasNo ratings yet
- Based On This Passage, What Would Most Likely Be True About "Snowbirds"?Document6 pagesBased On This Passage, What Would Most Likely Be True About "Snowbirds"?STEVENSNo ratings yet
- Chitral Tourism in 2019Document4 pagesChitral Tourism in 2019Kinza ZaheerNo ratings yet
- CHAPTERDocument74 pagesCHAPTERMazhar Hussain Ch.No ratings yet
- A Review of Indian Tourism Industry With Swot Analysis 2016Document4 pagesA Review of Indian Tourism Industry With Swot Analysis 2016avijitcu2007No ratings yet
- KZN Tourism 2010Document124 pagesKZN Tourism 2010BrabysNo ratings yet
- The Modal HotelDocument2 pagesThe Modal HotelCarlos AriasNo ratings yet
- Communication Case StudyDocument4 pagesCommunication Case StudySơn TràNo ratings yet
- Notes 2Document5 pagesNotes 2josueNo ratings yet
- Davao: By: Aira G. Calderon BSTM201ADocument8 pagesDavao: By: Aira G. Calderon BSTM201AAira CalderonNo ratings yet
- Reading Paper Part 1Document7 pagesReading Paper Part 1Atikah AmaranNo ratings yet
- BEIJING CHINA MAY 12-15, MAY 19-22, MAY 26-29 2023 FlyersDocument3 pagesBEIJING CHINA MAY 12-15, MAY 19-22, MAY 26-29 2023 FlyersGem HerreraNo ratings yet
- Accor Brand Portfolio Interactive Brochure August 22Document93 pagesAccor Brand Portfolio Interactive Brochure August 22Opeyemi TodowedeNo ratings yet
- Camping Trip: National Speech Competition PieceDocument4 pagesCamping Trip: National Speech Competition PieceBailey MurphyNo ratings yet
- Week 1macro Perspective in TourismDocument8 pagesWeek 1macro Perspective in TourismAngelica LozadaNo ratings yet