0% found this document useful (0 votes)
5K views3 pagesLocator Slip
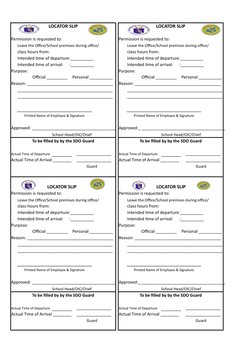
Locator's slips are used whenever a teacher/ deped employee wishes to go out for an personal/official purpose for a short period of time and has to go back to the station after transaction
Uploaded by
CynthiaCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as XLSX, PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
5K views3 pagesLocator Slip
Locator's slips are used whenever a teacher/ deped employee wishes to go out for an personal/official purpose for a short period of time and has to go back to the station after transaction
Uploaded by
CynthiaCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as XLSX, PDF, TXT or read online on Scribd