You might also like
- Entertainment Law Outline Winter 2008Document129 pagesEntertainment Law Outline Winter 2008downsowf100% (1)
- Guidebook On Life InsuranceDocument105 pagesGuidebook On Life InsuranceElearnmarketsNo ratings yet
- Exhibit - D - Sheriff Certificate of SaleDocument4 pagesExhibit - D - Sheriff Certificate of SaleCIARA MARIE DE LEONNo ratings yet
- INTERCHANGEDocument102 pagesINTERCHANGEDiego AvendañoNo ratings yet
- CIR v. Mirant PagbilaoDocument4 pagesCIR v. Mirant Pagbilaoamareia yap100% (1)
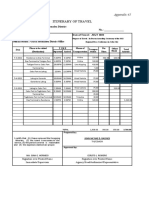
- Itinerary of Travel: Republic of The Philippines Ramon Magsaysay Technological University Iba, ZambalesDocument11 pagesItinerary of Travel: Republic of The Philippines Ramon Magsaysay Technological University Iba, ZambalesIndustrial TechnologyNo ratings yet
- FABM-2 LAS Quarter 3Document84 pagesFABM-2 LAS Quarter 3Rudelyn AlcantaraNo ratings yet
- Travel Logbook, Documents, & SuppliersDocument3 pagesTravel Logbook, Documents, & SuppliersJashley Cabazal BalatbatNo ratings yet
- Rtac IomDocument130 pagesRtac Iomfarshan296015No ratings yet
- Analyzing Common Business Transaction Using Debit and CreditDocument5 pagesAnalyzing Common Business Transaction Using Debit and CreditMarlyn Lotivio100% (1)
- Methods of Test For Petroleum and Its Products - BS 2000-476: Petroleum Liquids - Automatic Pipeline SamplingDocument62 pagesMethods of Test For Petroleum and Its Products - BS 2000-476: Petroleum Liquids - Automatic Pipeline SamplingTuesou Machere100% (3)
- Dealers Attitude QuestionnaireDocument3 pagesDealers Attitude QuestionnaireSUKUMAR80% (10)
- Criminal EtiologyDocument3 pagesCriminal EtiologyRonalyn PaunalNo ratings yet
- Pharmaceutical v. DOHDocument1 pagePharmaceutical v. DOHSean Hinolan100% (1)
- Blank Travel New ADocument1 pageBlank Travel New ABeverly Narvarte NavarroNo ratings yet
- Itinerary of TravelDocument2 pagesItinerary of TravelACENo ratings yet
- ItineraryoftravelDocument2 pagesItineraryoftravelACENo ratings yet
- Itinerary of Travel: Entity Name: Cagayan Valley Medical Center Fund Cluster: - No.Document2 pagesItinerary of Travel: Entity Name: Cagayan Valley Medical Center Fund Cluster: - No.Reia RuecoNo ratings yet
- Itinerary of Travel: Department of Justice Land Registration AuthorityDocument1 pageItinerary of Travel: Department of Justice Land Registration AuthorityOtenciano MautganonNo ratings yet
- Appendix 45 - Itinerary of Travel AttachmentDocument8 pagesAppendix 45 - Itinerary of Travel AttachmentregietubaNo ratings yet
- Itinerary of Travel: Appendix 45Document5 pagesItinerary of Travel: Appendix 45Claudine PuyaoNo ratings yet
- Travelling Expenses Itinenary Appendix A B 2023 Rfot RSPCDocument4 pagesTravelling Expenses Itinenary Appendix A B 2023 Rfot RSPCROSE ANN BALI-OSNo ratings yet
- Proposed Itinerary of Travel: National Defense College of The PhilippinesDocument1 pageProposed Itinerary of Travel: National Defense College of The PhilippinesDenize Nicole PaulinoNo ratings yet
- Proposed Itinerary of Travel: National Defense College of The PhilippinesDocument2 pagesProposed Itinerary of Travel: National Defense College of The PhilippinesDenize Nicole PaulinoNo ratings yet
- 8sci FM SpeedProbs-1358kwoDocument4 pages8sci FM SpeedProbs-1358kwoNico ImperialNo ratings yet
- Itinerary of Travel - Enumerators Jeanebarle JanDocument5 pagesItinerary of Travel - Enumerators Jeanebarle JancarlosNo ratings yet
- Arta Work OrientationDocument8 pagesArta Work OrientationJoseph Santos GacayanNo ratings yet
- 4.-ITINERARY-OF-TRAVEL-2-For ELNADocument2 pages4.-ITINERARY-OF-TRAVEL-2-For ELNAMylene Acluba LindoNo ratings yet
- Settlement of Travel ExpenseDocument1 pageSettlement of Travel ExpenselintangNo ratings yet
- Itinerary of Travel: Tagum Bus Terminal To Davaobus TerminDocument5 pagesItinerary of Travel: Tagum Bus Terminal To Davaobus TerminBennet James MenguitoNo ratings yet
- Disbursement Voucher: Provincial Agrarian Reform OfficeDocument30 pagesDisbursement Voucher: Provincial Agrarian Reform OfficeDIVINE JES ALFEREZNo ratings yet
- AppendixDocument8 pagesAppendixLileth Lastra QuiridoNo ratings yet
- 39 CenrDocument20 pages39 CenrMia Mamacotao-MasacalNo ratings yet
- Travel Events Request - Mohsin Arif RejaDocument1 pageTravel Events Request - Mohsin Arif RejaMohsin RejaNo ratings yet
- RSPC Awarding 2022 LiquidationDocument3 pagesRSPC Awarding 2022 LiquidationJOHN MC RAE RACINESNo ratings yet
- ROADSIDE OD SurveyDocument1 pageROADSIDE OD SurveyMeha NairNo ratings yet
- Itinerary of Travel: Philippine Statistics Authority - TarlacDocument1 pageItinerary of Travel: Philippine Statistics Authority - TarlacC'toik Y DweyNo ratings yet
- Itinerary of Travel SOCPEN MAY 2021Document19 pagesItinerary of Travel SOCPEN MAY 2021Arlene LuntokNo ratings yet
- Blank ItineraryDocument1 pageBlank ItinerarychristinemayfeliaNo ratings yet
- School Principal ItineraryDocument3 pagesSchool Principal ItineraryKaren S. RoblesNo ratings yet
- Unit13 Travel AgencyDocument13 pagesUnit13 Travel AgencyBea RomeroNo ratings yet
- FORM-Itinerary of TravelDocument96 pagesFORM-Itinerary of Travelshiena bignayNo ratings yet
- Itinerary of TravelDocument1 pageItinerary of Travelamelia fadriga100% (1)
- Appendix 45 IoTDocument1 pageAppendix 45 IoTBARANGAY LAMPAYAN100% (1)
- Travel Expenses Report V1.0Document2 pagesTravel Expenses Report V1.0EyeoSkyNo ratings yet
- Itinerary of Travel: Timamana National High SchoolDocument4 pagesItinerary of Travel: Timamana National High SchoolJULIETA DIWATANo ratings yet
- Unoffical Travel VoucherDocument1 pageUnoffical Travel VoucherLeracel ColladoNo ratings yet
- Travel Expenses Report: Type of Expense Description Advance Taken # Units RealizationDocument4 pagesTravel Expenses Report: Type of Expense Description Advance Taken # Units RealizationGomv ConsNo ratings yet
- National Institute of Technology-Andhra Pradesh: Travelling Allowance BillDocument2 pagesNational Institute of Technology-Andhra Pradesh: Travelling Allowance BillBabuRaoThellaNo ratings yet
- Itinerary-Of-Travel-Bsp Board MeetingDocument3 pagesItinerary-Of-Travel-Bsp Board Meetingjeffreylois.maestradoNo ratings yet
- Itenerary of TravelDocument2 pagesItenerary of TravelMae CieNo ratings yet
- 1A. Final Draft Survey Mv. Stellar RhapsodyDocument7 pages1A. Final Draft Survey Mv. Stellar RhapsodyDanangAjiNo ratings yet
- Travel Account EuroDocument2 pagesTravel Account EuroarekNo ratings yet
- Siddhath PaliDocument2 pagesSiddhath PaliSwarnendu DebNo ratings yet
- Authority To Travel REGINE A. PAGLINAWANDocument9 pagesAuthority To Travel REGINE A. PAGLINAWANChristian James ArenasNo ratings yet
- Disclosure VPFS 2019 03 DalgettyDocument25 pagesDisclosure VPFS 2019 03 Dalgettyaditya tripathiNo ratings yet
- LayoutsDocument3 pagesLayoutsSalman ahmadNo ratings yet
- Travel Authorization Form: To: Accounting & Finance DeptDocument4 pagesTravel Authorization Form: To: Accounting & Finance DeptSyabilah MarshandaNo ratings yet
- Airline Itinerary AL.2302104415508Document1 pageAirline Itinerary AL.2302104415508bartoabatuNo ratings yet
- Certification of Travel Completed: Entity Name: Tagulod High School Fund ClusterDocument3 pagesCertification of Travel Completed: Entity Name: Tagulod High School Fund ClusterloretaNo ratings yet
- Reservation Details: WdbikbDocument4 pagesReservation Details: WdbikbJulian FahiraNo ratings yet
- Career DevelopmentDocument5 pagesCareer Developmentjessie f. sernadillaNo ratings yet
- Travel ClaimDocument2 pagesTravel ClaimHailemariam FentawNo ratings yet
- Travel Expenses Non-Travel Expenses: Summary of ExpendituresDocument5 pagesTravel Expenses Non-Travel Expenses: Summary of Expendituresdanny leeNo ratings yet
- Certification of Travel Completed: Entity Name: SDO URDANETA Fund Cluster: - Tedie A. de VeraDocument7 pagesCertification of Travel Completed: Entity Name: SDO URDANETA Fund Cluster: - Tedie A. de VeraMark Jay BongolanNo ratings yet
- TEC - Nega Tewold - DakarDocument2 pagesTEC - Nega Tewold - DakarObo KeroNo ratings yet
- DV - TrainingDocument3 pagesDV - TrainingStacy Lactam SacopasoNo ratings yet
- Shipping Container Tracking and Tracing - MSCDocument2 pagesShipping Container Tracking and Tracing - MSCShiv KumarNo ratings yet
- Liquidation Report: Southern Leyte State University - Tomas OppusDocument1 pageLiquidation Report: Southern Leyte State University - Tomas OppusNeWo YanTotNo ratings yet
- Trav El Order: Philippine Red CrossDocument2 pagesTrav El Order: Philippine Red CrossJhoi ObiasNo ratings yet
- TEC ADD-NBO-ADD - EliasDocument2 pagesTEC ADD-NBO-ADD - EliasObo KeroNo ratings yet
- 02 Value Drivers - HWS2021Document38 pages02 Value Drivers - HWS2021Gonzalo De CorralNo ratings yet
- Competition Commission of IndiaDocument5 pagesCompetition Commission of IndiaMehak joshiNo ratings yet
- The South Butt Answer To The North Face ClaimDocument12 pagesThe South Butt Answer To The North Face ClaimleftwallNo ratings yet
- Spouses Rodrigo Imperial JRDocument3 pagesSpouses Rodrigo Imperial JRNoel Christopher G. BellezaNo ratings yet
- Ford Investment ThesisDocument7 pagesFord Investment Thesispatricialeatherbyelgin100% (1)
- SBD 99Document11 pagesSBD 99Mudasir Bashir KoulNo ratings yet
- Common GoodDocument13 pagesCommon GoodXyzzielleNo ratings yet
- Appresponse Xpert Administrator Guide.9.0.3.712 00195 02 - Rev 2 PDFDocument216 pagesAppresponse Xpert Administrator Guide.9.0.3.712 00195 02 - Rev 2 PDFEdwin Manolo Mendez SNo ratings yet
- DigestDocument12 pagesDigestPamela ParceNo ratings yet
- Configuration Guide For Carrying Vlan Ids in Packets Sent by The Web LCTDocument13 pagesConfiguration Guide For Carrying Vlan Ids in Packets Sent by The Web LCTJoshua Paz GalvezNo ratings yet
- Rainer Arms Agrees To Turnover Customer InformationDocument10 pagesRainer Arms Agrees To Turnover Customer InformationJohn CrumpNo ratings yet
- IAAF Competition Rules 2010-2011Document255 pagesIAAF Competition Rules 2010-2011affel_attaNo ratings yet
- LEA MER INDUSTRIES, INC., G.R. No. 161745 Petitioner,-Versus - MALAYAN INSURANCE CO., INC., Respondent. September 30, 2005 Panganiban, J.: FactsDocument4 pagesLEA MER INDUSTRIES, INC., G.R. No. 161745 Petitioner,-Versus - MALAYAN INSURANCE CO., INC., Respondent. September 30, 2005 Panganiban, J.: FactsKeir Joey Taleon CravajalNo ratings yet
- Philosophy Education Society IncDocument31 pagesPhilosophy Education Society IncAnonymous lVC1HGpHP3No ratings yet
- Chap 8 Distribution ManagementDocument30 pagesChap 8 Distribution ManagementThomas Niconar PalemNo ratings yet
- Induction For New Leaders and Managers: Human Resources and Organisational DevelopmentDocument18 pagesInduction For New Leaders and Managers: Human Resources and Organisational DevelopmentHemanshi BharmaniNo ratings yet
- Corporate Present Nov 09Document59 pagesCorporate Present Nov 09Amol GodboleNo ratings yet
- YFC HH Training ProgramDocument11 pagesYFC HH Training ProgramMay Angelie LopezNo ratings yet