You might also like
- Rabies Vaccines Its Role Challenges Considerationsand ImplicationsforDocument27 pagesRabies Vaccines Its Role Challenges Considerationsand ImplicationsforNimra Naveed ShaikhNo ratings yet
- Cuppa Wao Journal ProofsDocument22 pagesCuppa Wao Journal ProofsFajar SetiawanNo ratings yet
- The Science of Herbal Antivirals: Emerging Trends in Natural Viral Defense MechanismsFrom EverandThe Science of Herbal Antivirals: Emerging Trends in Natural Viral Defense MechanismsNo ratings yet
- Synthesis Paper Final DraftDocument16 pagesSynthesis Paper Final Draftapi-410826283No ratings yet
- Study Drug Resistance in Bacteria Using AntibioticsDocument17 pagesStudy Drug Resistance in Bacteria Using AntibioticsJagatha RaasmiNo ratings yet
- Project Micro BiologyDocument37 pagesProject Micro Biologyfawasadekunle111No ratings yet
- Application of Bacteriophages: April 2017Document5 pagesApplication of Bacteriophages: April 2017Ahmed AlbagerNo ratings yet
- Fdocuments - in Biology Investigatory Project 561e79b91f5a0Document18 pagesFdocuments - in Biology Investigatory Project 561e79b91f5a0ASHOKNo ratings yet
- Functionalized Nanomaterials for the Management of Microbial Infection: A Strategy to Address Microbial Drug ResistanceFrom EverandFunctionalized Nanomaterials for the Management of Microbial Infection: A Strategy to Address Microbial Drug ResistanceRabah BoukherroubNo ratings yet
- The Hidden Strength of Plant Antivirals: Revolutionizing Health with Nature's PharmacyFrom EverandThe Hidden Strength of Plant Antivirals: Revolutionizing Health with Nature's PharmacyNo ratings yet
- Chapter 1Document7 pagesChapter 1Edwin DatanNo ratings yet
- Biology Final Paper 2Document6 pagesBiology Final Paper 2Shawn Inglis-McInnisNo ratings yet
- A Century of Clinical Use of Phages A Literature RDocument23 pagesA Century of Clinical Use of Phages A Literature RIsidora NikolicNo ratings yet
- Pet-to-Man Travelling Staphylococci: A World in ProgressFrom EverandPet-to-Man Travelling Staphylococci: A World in ProgressVincenzo SaviniNo ratings yet
- Thought Leaders: Bacteriophage Therapy: An Alternative To Antibiotics? An Interview Professor ClokieDocument17 pagesThought Leaders: Bacteriophage Therapy: An Alternative To Antibiotics? An Interview Professor ClokieJeri BerongoyNo ratings yet
- Study On Emergence of MDR Pathogen and Its Microbiological StudyDocument9 pagesStudy On Emergence of MDR Pathogen and Its Microbiological StudyIJAR JOURNALNo ratings yet
- Antibiotics Produced by Streptomyces PDFDocument7 pagesAntibiotics Produced by Streptomyces PDFRosyiDa Ismi BarrorohNo ratings yet
- Effects of Antibiotics on MicroorganismsDocument13 pagesEffects of Antibiotics on MicroorganismsSamanwitha SharmaNo ratings yet
- BacteriaDocument15 pagesBacteriaLara AhmedNo ratings yet
- Bacteriological Profile and Antibiotic Sensitivity Patterns in Clinical Isolates From The Out-Patient Departments of A Tertiary Hospital in NigeriaDocument9 pagesBacteriological Profile and Antibiotic Sensitivity Patterns in Clinical Isolates From The Out-Patient Departments of A Tertiary Hospital in NigeriaAtul Kumar GoyalNo ratings yet
- Antibiotic Resistant Bacteria Research PaperDocument8 pagesAntibiotic Resistant Bacteria Research Paperafmcueagg100% (1)
- Nature's Answer to Viral Threats: Understanding the Potency of Plant-Based AntiviralsFrom EverandNature's Answer to Viral Threats: Understanding the Potency of Plant-Based AntiviralsNo ratings yet
- Assignment 1 BI 602Document6 pagesAssignment 1 BI 602Eneah NaicavacavaNo ratings yet
- Investigating Human Diseases with the Microbiome: Metagenomics Bench to BedsideFrom EverandInvestigating Human Diseases with the Microbiome: Metagenomics Bench to BedsideNo ratings yet
- Probiotics, Prebiotics and The Microbiome PDFDocument10 pagesProbiotics, Prebiotics and The Microbiome PDFkuldeep sainiNo ratings yet
- Amphioxus Immunity: Tracing the Origins of Human ImmunityFrom EverandAmphioxus Immunity: Tracing the Origins of Human ImmunityAn-Long XuNo ratings yet
- Last Help: Phage Therapy?: For 100 Years, a Successful Alternative to Conventional Antibiotic TreatmentsFrom EverandLast Help: Phage Therapy?: For 100 Years, a Successful Alternative to Conventional Antibiotic TreatmentsNo ratings yet
- Exploring the World of Herbal Antivirals: Ancient Wisdom and Modern Science in Viral ProtectionFrom EverandExploring the World of Herbal Antivirals: Ancient Wisdom and Modern Science in Viral ProtectionNo ratings yet
- Antifungal Compounds Discovery: Natural and Synthetic ApproachesFrom EverandAntifungal Compounds Discovery: Natural and Synthetic ApproachesNo ratings yet
- Antibiotics 10 00124Document32 pagesAntibiotics 10 00124Mariyum SanaNo ratings yet
- Antibiotic Resistance Cure with BacteriophagesDocument3 pagesAntibiotic Resistance Cure with BacteriophagesHinggil NugrohoNo ratings yet
- Antimicrobial Peptide - New Frontiers in The Therapy InfecctionsDocument41 pagesAntimicrobial Peptide - New Frontiers in The Therapy InfecctionsIsidora CastroNo ratings yet
- Biology Investigatory Project (Advanced)Document27 pagesBiology Investigatory Project (Advanced)Yogi Arya75% (4)
- Thesis Topics About BacteriaDocument4 pagesThesis Topics About BacteriaWriteMyPaperOneDayHartford100% (2)
- Báo-Agriculture and Food Animals As A Source of Antimicrobial-Resistant BacteriaDocument14 pagesBáo-Agriculture and Food Animals As A Source of Antimicrobial-Resistant BacteriaYến LinhNo ratings yet
- Isolation Identification and Functional CharacteriDocument9 pagesIsolation Identification and Functional CharacteriJ BNo ratings yet
- The Use of Bacteriophages To Treat Bacterial InfectionsDocument8 pagesThe Use of Bacteriophages To Treat Bacterial InfectionsMugambi OliverNo ratings yet
- Nonclinical Development of Novel Biologics, Biosimilars, Vaccines and Specialty BiologicsFrom EverandNonclinical Development of Novel Biologics, Biosimilars, Vaccines and Specialty BiologicsLisa PlitnickNo ratings yet
- PHD Thesis Antibiotic ResistanceDocument6 pagesPHD Thesis Antibiotic ResistancePayingSomeoneToWriteAPaperLubbock100% (2)
- Medical Microbiology Research Paper TopicsDocument6 pagesMedical Microbiology Research Paper Topicsafeaoebid100% (1)
- Nanoparticles and the Immune System: Safety and EffectsFrom EverandNanoparticles and the Immune System: Safety and EffectsDiana BoraschiNo ratings yet
- Studying Drug Resistance in Bacteria Using AntibioticsDocument6 pagesStudying Drug Resistance in Bacteria Using AntibioticsAyush YadavNo ratings yet
- JmcjmsDocument11 pagesJmcjmsADELUWOYE-AJAYI OLATEMI AMOSNo ratings yet
- Salcedo, Eastern Samar 6807 Eastern Samar, PhilippinesDocument7 pagesSalcedo, Eastern Samar 6807 Eastern Samar, PhilippinesJenny PartozaNo ratings yet
- 16Document15 pages16KIU PUBLICATION AND EXTENSIONNo ratings yet
- Antibiotic Resistance Microbe StudyDocument20 pagesAntibiotic Resistance Microbe StudySneha BagulNo ratings yet
- Review 65 AntibioticsDocument10 pagesReview 65 AntibioticsR GajendranNo ratings yet
- Atlas of Oral Microbiology: From Healthy Microflora to DiseaseFrom EverandAtlas of Oral Microbiology: From Healthy Microflora to DiseaseXuedong ZhouRating: 4.5 out of 5 stars4.5/5 (2)
- Example of A Research Paper On Microbiology TopicsDocument8 pagesExample of A Research Paper On Microbiology TopicszxnrvkrifNo ratings yet
- 273 Easy & Intermediate Piano Pieces PDFDocument401 pages273 Easy & Intermediate Piano Pieces PDFLuis Alcaraz100% (35)
- 273 Easy & Intermediate Piano Pieces PDFDocument401 pages273 Easy & Intermediate Piano Pieces PDFLuis Alcaraz100% (35)
- GXL3000 Sheet InfoDocument1 pageGXL3000 Sheet InfoLuis AlcarazNo ratings yet
- Ludovico Einaudi - ElementsDocument98 pagesLudovico Einaudi - ElementsJuanVenegas22No ratings yet
- Chlorine and Alternative Disinfectants 2005 PDFDocument117 pagesChlorine and Alternative Disinfectants 2005 PDFLuis AlcarazNo ratings yet
- A Century of Bacteriophage Research PDFDocument21 pagesA Century of Bacteriophage Research PDFLuis AlcarazNo ratings yet
- Bacteriophages Clinical ApplicationsDocument11 pagesBacteriophages Clinical ApplicationsLuis AlcarazNo ratings yet
- A Century of Bacteriophage Research PDFDocument21 pagesA Century of Bacteriophage Research PDFLuis AlcarazNo ratings yet
- Bacteriophages As Promising Tools 2016Document9 pagesBacteriophages As Promising Tools 2016Luis AlcarazNo ratings yet
- Bacteriophages and Their Applications PDFDocument12 pagesBacteriophages and Their Applications PDFLuis AlcarazNo ratings yet
- Choir Training Based On Voice Production Fotoc PDFDocument64 pagesChoir Training Based On Voice Production Fotoc PDFLuis Alcaraz100% (1)
- Bacteriophages and Their Applications PDFDocument12 pagesBacteriophages and Their Applications PDFLuis AlcarazNo ratings yet
- My First Piano - Saeed YahyazadehDocument14 pagesMy First Piano - Saeed YahyazadehSaeed Yahyazadeh93% (29)
- Acordes en A4Document1 pageAcordes en A4Luis AlcarazNo ratings yet
- Self-Help in Piano Study - Brower 1920Document256 pagesSelf-Help in Piano Study - Brower 1920Luis AlcarazNo ratings yet
- Behringer Nu3000 More InfoDocument14 pagesBehringer Nu3000 More InfoPuican IulianNo ratings yet
- Hiv and Aids in Children3Document25 pagesHiv and Aids in Children3Kazau FwalangaNo ratings yet
- BUCCAL FAT PAD FLAP REPAIRS SMALL ORAL DEFECTSDocument4 pagesBUCCAL FAT PAD FLAP REPAIRS SMALL ORAL DEFECTSAlex OprisanNo ratings yet
- Toxicological and Pharmacokinetic Properties of Sucralose 6 Acetate and Its Parent Sucralose in Vitro Screening AssaysDocument36 pagesToxicological and Pharmacokinetic Properties of Sucralose 6 Acetate and Its Parent Sucralose in Vitro Screening AssayswipiriNo ratings yet
- Radiotherapy and Oncology: Karen Wong, Geoff P. Delaney, Michael B. BartonDocument5 pagesRadiotherapy and Oncology: Karen Wong, Geoff P. Delaney, Michael B. BartonFrançois IdjiwoleNo ratings yet
- Defibrillator: DR Sumanth ReddyDocument39 pagesDefibrillator: DR Sumanth Reddyrohith100% (1)
- The Liver Is An Incredibly Hard Working Organ. Every Day, It Performs Hundreds of Critical Functions That Keep Your Body HealthyDocument27 pagesThe Liver Is An Incredibly Hard Working Organ. Every Day, It Performs Hundreds of Critical Functions That Keep Your Body HealthyHafiz Mat JizatNo ratings yet
- Anesthesiology GuideDocument4 pagesAnesthesiology GuideGeorge Wang100% (1)
- Antibiotics ResistanceDocument8 pagesAntibiotics ResistanceboredtarteelNo ratings yet
- Common Abdominal IncisionsDocument3 pagesCommon Abdominal IncisionsMarynel Dixie Izon BraoNo ratings yet
- Types of Medications Used After SurgeryDocument9 pagesTypes of Medications Used After SurgeryRegine VillanuevaNo ratings yet
- Macrocytic anemia causes and treatmentDocument2 pagesMacrocytic anemia causes and treatmentLefteris ChatzidoukasNo ratings yet
- NCP - Ineffective Breathing PatternDocument4 pagesNCP - Ineffective Breathing PatternPRINCESS KOBAYASHINo ratings yet
- Biocompatibility of Dental Materials and Related ResearchesDocument70 pagesBiocompatibility of Dental Materials and Related ResearchesSoumik KarmakarNo ratings yet
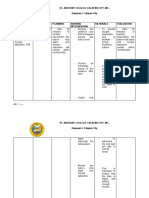
- St. Anthony College Calapan City, Inc. Bayanan I, Calapan CityDocument3 pagesSt. Anthony College Calapan City, Inc. Bayanan I, Calapan CityMike Faustino SolangonNo ratings yet
- Doh 1Document3 pagesDoh 1Fitz Dyan TorresNo ratings yet
- Identifying and Investigating OutbreaksDocument74 pagesIdentifying and Investigating OutbreaksCesarNo ratings yet
- W3health6 q1 Mod1of2 PersonalHealthIssuesSelf-MngtSkills v2-1Document22 pagesW3health6 q1 Mod1of2 PersonalHealthIssuesSelf-MngtSkills v2-1Rona DindangNo ratings yet
- Ketorolac (Drug Study)Document2 pagesKetorolac (Drug Study)Cassandra Grace Labial Paynter89% (18)
- MICROPARA LEC Chapter 14 ReviewerDocument11 pagesMICROPARA LEC Chapter 14 ReviewerRen “Shel” ManaloNo ratings yet
- Increased Intracranial Pressure NCLEX ReviewDocument8 pagesIncreased Intracranial Pressure NCLEX ReviewAnia JuanNo ratings yet
- Oral Field CancerizationDocument7 pagesOral Field CancerizationFarah UlyaNo ratings yet
- Cerebrovascular AccidentDocument62 pagesCerebrovascular AccidentJaydee DalayNo ratings yet
- Complete Small Med Surgery 2Document65 pagesComplete Small Med Surgery 2MelanieNo ratings yet
- What Are The Challenges of Working With Mentally Ill Mothers Jerina SpicerDocument19 pagesWhat Are The Challenges of Working With Mentally Ill Mothers Jerina Spicerjerina spicerNo ratings yet
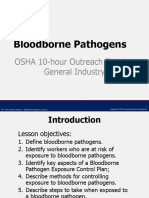
- Bloodborne Pathogens PPT v-03!01!17Document44 pagesBloodborne Pathogens PPT v-03!01!17kunalphalswal0005No ratings yet
- Flower EsscencesDocument2 pagesFlower EsscencesDivyajyoti DevaNo ratings yet
- Clinical Case NobelReplace Conical Connection Alessandro PozziDocument8 pagesClinical Case NobelReplace Conical Connection Alessandro PozziShyam BhatNo ratings yet
- Detecting Hemoperitoneum: Limitations of Repeat FAST ExamsDocument123 pagesDetecting Hemoperitoneum: Limitations of Repeat FAST ExamsSinisa Ristic50% (2)
- AS Biology F211 Animal Transport Workbooklet Answers p1-10Document11 pagesAS Biology F211 Animal Transport Workbooklet Answers p1-10T-Jay Ellis-DaleNo ratings yet
- Breast Cancer ScreeningDocument9 pagesBreast Cancer Screeningsorin.morosan64No ratings yet