You might also like
- Inner Yoga: 23 Simple Self-Care Tools for Peace, Healing, and Authentic EmpowermentFrom EverandInner Yoga: 23 Simple Self-Care Tools for Peace, Healing, and Authentic EmpowermentNo ratings yet
- Mind your Zen. A Beginner's Guide to Daily Mindfulness: to calm your mind and reduce stress & anxiety: Health & Wellbeing, #1From EverandMind your Zen. A Beginner's Guide to Daily Mindfulness: to calm your mind and reduce stress & anxiety: Health & Wellbeing, #1No ratings yet
- Pals CardDocument12 pagesPals CardSara KhanNo ratings yet
- BLS - CPRDocument42 pagesBLS - CPREdzelDawnGarciaDayritNo ratings yet
- 2010 Bls Study Guide PDFDocument1 page2010 Bls Study Guide PDFMarieNo ratings yet
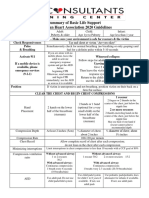
- Basic Life Support Protocol MatrixDocument1 pageBasic Life Support Protocol MatrixAleksandar PetrovicNo ratings yet
- 2016bls Pop Quiz AnswersDocument2 pages2016bls Pop Quiz AnswersAhmed AlkhaqaniNo ratings yet
- 2005 Aha Bls and Acls SummaryDocument3 pages2005 Aha Bls and Acls SummarypauerishNo ratings yet
- BLS KeypointsDocument34 pagesBLS KeypointsTompomNo ratings yet
- Ncma217rle Newborn AssessmentDocument5 pagesNcma217rle Newborn AssessmentJerica Mae VenoyaNo ratings yet
- CPR Key NumbersDocument1 pageCPR Key NumbersPaul ShanamanNo ratings yet
- Normal Vital Signs Guidelines For EmsDocument4 pagesNormal Vital Signs Guidelines For EmsJonathan delos ReyesNo ratings yet
- BLSDocument53 pagesBLSBingbing LaguaNo ratings yet
- HA2Document3 pagesHA2nezukonez81No ratings yet
- 2020 BLS SummaryDocument1 page2020 BLS SummaryAnshika yadavNo ratings yet
- BLS For Healthcare Provider - STUDY GUIDE: The CPR Hero Training Center 2010 AHA GuidelinesDocument1 pageBLS For Healthcare Provider - STUDY GUIDE: The CPR Hero Training Center 2010 AHA GuidelinesUser 1No ratings yet
- Newborn Vital Signs Vital Sign Normal Nursing Implications RespirationsDocument2 pagesNewborn Vital Signs Vital Sign Normal Nursing Implications RespirationsManuela GutiérrezNo ratings yet
- Basic Life SupportDocument22 pagesBasic Life SupportMYRA ASEGURADONo ratings yet
- Symptom/Care Adult Child Infant: (Puberty Onset and Older) (Prepubescent) (Approximately Less Than 1 Year Old)Document9 pagesSymptom/Care Adult Child Infant: (Puberty Onset and Older) (Prepubescent) (Approximately Less Than 1 Year Old)Aleksandar PetrovicNo ratings yet
- BLS-non NursingDocument24 pagesBLS-non NursingDr Puteri Nur Sabrina Binti Mohd HanapiNo ratings yet
- Summary of CPR Steps 2016Document1 pageSummary of CPR Steps 2016Katerina TsNo ratings yet
- Abdulfattah Alhazmi Ayhazmi@uqu - Edu.saDocument18 pagesAbdulfattah Alhazmi Ayhazmi@uqu - Edu.saعبدالرحمن الحربيNo ratings yet
- AmeriMed CPR CABs For BLS For Healthcare ProfessionalsDocument1 pageAmeriMed CPR CABs For BLS For Healthcare Professionalsimran shabbirNo ratings yet
- Caring For Cardiac Arrest: CPR and AED - Children and InfantsDocument2 pagesCaring For Cardiac Arrest: CPR and AED - Children and InfantsMike SchermNo ratings yet
- CPR According To Age (BSN1114-2010-2011 FEU-INSTITUTE OF NURSING)Document1 pageCPR According To Age (BSN1114-2010-2011 FEU-INSTITUTE OF NURSING)merryechevarriaNo ratings yet
- FON Information موشتاقDocument3 pagesFON Information موشتاقzaetwnnawzad2004No ratings yet
- 04 - 3.2 - Pediatric EmergenciesDocument149 pages04 - 3.2 - Pediatric EmergenciesISFAHAN MASULOTNo ratings yet
- COMFORT ScaleDocument7 pagesCOMFORT ScaleALDO STEFANUZ (STIK)No ratings yet
- 2021 BLS Study GuideDocument2 pages2021 BLS Study GuideShane Brown100% (2)
- Summary of High-Quality CPR Components For BLS ProvidersDocument1 pageSummary of High-Quality CPR Components For BLS ProvidersPhilippe Ceasar C. BascoNo ratings yet
- Healthcare Provider CAB of CPR Helpful HintsDocument2 pagesHealthcare Provider CAB of CPR Helpful HintsDarrell BrightNo ratings yet
- Bls Study GuideDocument2 pagesBls Study GuideJohnNo ratings yet
- Konsep Resusitasi Jantung Paru: BY: Ns. Anita Dwi Ariyani, S.Kep,.M.KepDocument31 pagesKonsep Resusitasi Jantung Paru: BY: Ns. Anita Dwi Ariyani, S.Kep,.M.KepFa An RaNo ratings yet
- Summary of High-Quality CPR Components For BLS Providers: Component Adults and Adolescents Children InfantsDocument1 pageSummary of High-Quality CPR Components For BLS Providers: Component Adults and Adolescents Children InfantsAlfonso Tuñoque Chavez0% (1)
- 2005 CPR and AED Guidelines For Lay RescuersDocument2 pages2005 CPR and AED Guidelines For Lay RescuersIne Marthia DanieNo ratings yet
- Pain ManagementDocument27 pagesPain ManagementMartha Sasmitha NingrumNo ratings yet
- Healthcare CPR Cheat Sheet: Check The SceneDocument2 pagesHealthcare CPR Cheat Sheet: Check The SceneRocel Marie SullestaNo ratings yet
- Guide For History Taking, Physical Exam and Diagnosis of Pediatric PatientsDocument19 pagesGuide For History Taking, Physical Exam and Diagnosis of Pediatric PatientsKendall Marie BuenavistaNo ratings yet
- BLS PDFDocument6 pagesBLS PDFAyesha Jadoon80% (5)
- Manajemen Nyeri RS Jantung Har KitDocument18 pagesManajemen Nyeri RS Jantung Har KitYuniNo ratings yet
- B 04 Paediatric DefibrillationDocument10 pagesB 04 Paediatric DefibrillationIndri AbdulNo ratings yet
- BLS Book (New)Document7 pagesBLS Book (New)Saman FirdousNo ratings yet
- Wheeze in Children: Asthma Clinical Pathway: Departments of Emergency Medicine and PaediatricsDocument4 pagesWheeze in Children: Asthma Clinical Pathway: Departments of Emergency Medicine and Paediatricsscanutd100% (1)
- 19penyusunnan Dan Kegunaan LksDocument1 page19penyusunnan Dan Kegunaan LksImam HakamNo ratings yet
- Healthcare Provider Summary of Steps of CPR For Adults, Children and InfantsDocument2 pagesHealthcare Provider Summary of Steps of CPR For Adults, Children and InfantsMARK LENAND ESPIRITUNo ratings yet
- My DiaryDocument91 pagesMy DiarydrtgodeNo ratings yet
- Acute Care 30: Glasgow Coma Scale-Adult, Pediatric, Infant: Eye OpeningDocument2 pagesAcute Care 30: Glasgow Coma Scale-Adult, Pediatric, Infant: Eye OpeningOkdiantoRahmanGastiNo ratings yet
- 1 AlgorithmsDocument19 pages1 AlgorithmsRiya Sood100% (1)
- ER Additional ReqsDocument3 pagesER Additional ReqsSaidimar Caramijan SalimNo ratings yet
- Head To Toe Assessment Guide ToolDocument3 pagesHead To Toe Assessment Guide Toolkezia_lillyNo ratings yet
- Presentation TOT KDM Pend. Khas - 22 April 2015Document4 pagesPresentation TOT KDM Pend. Khas - 22 April 2015Jocelyn WongNo ratings yet
- Holy Infant College Tacloban City NSTP - Cwts Unit First AidDocument40 pagesHoly Infant College Tacloban City NSTP - Cwts Unit First AidWinsley RazNo ratings yet
- Basic Life Support Lecture PresentationDocument38 pagesBasic Life Support Lecture PresentationAlsaud BansilNo ratings yet
- BLS Study Guide and PretestDocument47 pagesBLS Study Guide and PretestRicha AbcedeNo ratings yet
- Basic Nursing Knowledge and SkillsDocument10 pagesBasic Nursing Knowledge and SkillsFatima CorpuzNo ratings yet
- Nilai Normal Tanda Vital Pada Anak: PediatriDocument9 pagesNilai Normal Tanda Vital Pada Anak: PediatriGursal Raigandra SiregarNo ratings yet
- Formal Evaluation of Asthma Exacerbation Severity in The Urgent or Emergency CarDocument3 pagesFormal Evaluation of Asthma Exacerbation Severity in The Urgent or Emergency Carمعاذ الشريفNo ratings yet
- Apgar Scoring: Birth To Ascertain The Need For Immediate CareDocument3 pagesApgar Scoring: Birth To Ascertain The Need For Immediate CarejeromeNo ratings yet
- 667f3b52-4eee-4365-a03c-925ad2d8fec6Document18 pages667f3b52-4eee-4365-a03c-925ad2d8fec6YuniNo ratings yet
- BLS MODULE For Students 2020 Guidelines UpdateDocument19 pagesBLS MODULE For Students 2020 Guidelines Updatemarina valdez de castroNo ratings yet
- Measure, Determine, Check: For Accuracy, Please Ensure That PDF Is Printed at 100%Document1 pageMeasure, Determine, Check: For Accuracy, Please Ensure That PDF Is Printed at 100%twizas3926No ratings yet
- Algo ArrestDocument2 pagesAlgo ArrestLocomotorica FK UkiNo ratings yet
- ATLS Practice Test 1: Other ThanDocument11 pagesATLS Practice Test 1: Other ThanGarcia Rosa75% (8)
- Algo ArrestDocument2 pagesAlgo ArrestLocomotorica FK UkiNo ratings yet
- Eye Spontaneous Spontaneous 4 OpeningDocument10 pagesEye Spontaneous Spontaneous 4 OpeningandiyanimalikNo ratings yet
- Eye Spontaneous Spontaneous 4 OpeningDocument10 pagesEye Spontaneous Spontaneous 4 OpeningandiyanimalikNo ratings yet
- Shock: Shout For Help/Activate Emergency ResponseDocument6 pagesShock: Shout For Help/Activate Emergency ResponseandiyanimalikNo ratings yet
- Medical Dokumen WewDocument3 pagesMedical Dokumen WewandiyanimalikNo ratings yet
- Algo Postarrest PDFDocument1 pageAlgo Postarrest PDFdewita wahyu kemalasariNo ratings yet
- Siloam Hospital Group EMT Course Practical Examination Spinal Immobilization (Seated Patient)Document2 pagesSiloam Hospital Group EMT Course Practical Examination Spinal Immobilization (Seated Patient)andiyanimalikNo ratings yet
- Siloam Hospital Group EMT Course Practical Examination Intravenous TherapyDocument3 pagesSiloam Hospital Group EMT Course Practical Examination Intravenous TherapyandiyanimalikNo ratings yet
- Dual Lumen AirwayDocument2 pagesDual Lumen AirwayandiyanimalikNo ratings yet
- Advanced and Paramedic Practial ExamDocument3 pagesAdvanced and Paramedic Practial ExamandiyanimalikNo ratings yet
- Adult VentilationDocument3 pagesAdult VentilationandiyanimalikNo ratings yet
- Drug Study SulodexideDocument2 pagesDrug Study SulodexideAkiraMamoNo ratings yet
- CBDepot - Eu Product SpecificationDocument16 pagesCBDepot - Eu Product SpecificationMichal TőzsérNo ratings yet
- Diabetesmeds AcceptablecombDocument2 pagesDiabetesmeds AcceptablecombCotton LogicNo ratings yet
- Sma18 4742Document24 pagesSma18 4742WDIV/ClickOnDetroitNo ratings yet
- Contrast Reaction Card LandscapeDocument2 pagesContrast Reaction Card LandscapecornealenutaNo ratings yet
- General AnestheticsDocument38 pagesGeneral AnestheticsAnonymous iG0DCOfNo ratings yet
- Merchant Shipping (Medicines, Medical Stores and Appliances) Rules, 1994Document18 pagesMerchant Shipping (Medicines, Medical Stores and Appliances) Rules, 1994pravenNo ratings yet
- Imunisasi Record - KennyDocument1 pageImunisasi Record - KennyrifiNo ratings yet
- Eye Docs Pharmacology & TherapeuticsDocument72 pagesEye Docs Pharmacology & TherapeuticsMuhammed Abdulmajeed100% (1)
- Make Better Decisions - ShareDocument161 pagesMake Better Decisions - ShareDuyLENguyenHoangNo ratings yet
- Non-Steroidal Anti-Inflammatory Drugs (Nsaids) : Dr. Nishant B. BhansaliDocument24 pagesNon-Steroidal Anti-Inflammatory Drugs (Nsaids) : Dr. Nishant B. Bhansaliankit ahirNo ratings yet
- Race Cadot RilDocument2 pagesRace Cadot RilFebson Lee MathewNo ratings yet
- Illegal DrugsDocument37 pagesIllegal Drugsangker arnelNo ratings yet
- Anxiolytic DrugsDocument8 pagesAnxiolytic DrugsTony DawaNo ratings yet
- Swot MerckDocument3 pagesSwot Mercktomassetya0% (1)
- 508-Prowell-Final Slides5Document25 pages508-Prowell-Final Slides5dfsdjgflksjgnawNo ratings yet
- Chapter Vi DrugsDocument4 pagesChapter Vi DrugsSheryl TapayanNo ratings yet
- RecallsDocument111 pagesRecallsDrSamia El Wakil100% (2)
- 成大常見藥物泡法Document3 pages成大常見藥物泡法吳任爵No ratings yet
- High Alert Medications 2018Document30 pagesHigh Alert Medications 2018Eman MohamedNo ratings yet
- LETAK HPV-Sanevax Hrvatska VerzijaDocument2 pagesLETAK HPV-Sanevax Hrvatska VerzijaNikola IvankovicNo ratings yet
- Primer of Drug Action 12th Edition Julien Test BankDocument11 pagesPrimer of Drug Action 12th Edition Julien Test BankMelanieWarddsbim100% (16)
- Drug Study Rle Final 1Document18 pagesDrug Study Rle Final 1YBH Construction SupplyNo ratings yet
- Pharmacotherapeutics in ObstetricsDocument103 pagesPharmacotherapeutics in Obstetricssanthanalakshmi100% (4)
- Doctor ExhibitDocument110 pagesDoctor ExhibitKFORNo ratings yet
- OBATDocument10 pagesOBATDeiLa SariNo ratings yet
- Therapeutic Classifications of DrugsDocument125 pagesTherapeutic Classifications of DrugsAbhishek Singh100% (1)
- Cough N Cold Medicine List PDFDocument7 pagesCough N Cold Medicine List PDFDonna DominnoNo ratings yet
- Drug Discovery Complete NotesDocument5 pagesDrug Discovery Complete NotesSadiqa ForensicNo ratings yet
- Synthetic Cannabinoid Fact Sheet PDFDocument4 pagesSynthetic Cannabinoid Fact Sheet PDFwebmaster@drugpolicy.orgNo ratings yet