You might also like
- Emcee King & QueenDocument8 pagesEmcee King & QueenMaryHazelClaveBeniga100% (10)
- Harvard Case Study - AccountingDocument3 pagesHarvard Case Study - AccountingSuman Saurabh MohantyNo ratings yet
- Applying Lean and Six Sigma To Your Dermatology PracticeDocument7 pagesApplying Lean and Six Sigma To Your Dermatology PracticedrustagiNo ratings yet
- Kaizen Continuous ImprovementDocument4 pagesKaizen Continuous ImprovementPradeep NarendiranNo ratings yet
- Quality Circles and Teams-Tqm NotesDocument8 pagesQuality Circles and Teams-Tqm NotesStanley Cheruiyot100% (1)
- Lean Done Right: Achieve and Maintain Reform in Your Healthcare OrganizationFrom EverandLean Done Right: Achieve and Maintain Reform in Your Healthcare OrganizationNo ratings yet
- The Tracking Shot in Kapo Serge Daney Senses of CinemaDocument22 pagesThe Tracking Shot in Kapo Serge Daney Senses of CinemaMarcos GonzálezNo ratings yet
- Blooms Taxonomy and Costas Level of QuestioningDocument6 pagesBlooms Taxonomy and Costas Level of QuestioningChris Tine100% (1)
- October 2016 Practice PerfectDocument2 pagesOctober 2016 Practice PerfectNaresh SapoliaNo ratings yet
- 196-1584526128 LeanhospitalDocument8 pages196-1584526128 LeanhospitalDharm Veer RathoreNo ratings yet
- Social Science & Medicine: Zoe J. Radnor, Matthias Holweg, Justin WaringDocument8 pagesSocial Science & Medicine: Zoe J. Radnor, Matthias Holweg, Justin WaringOrfani Valencia MenaNo ratings yet
- Lean Principles in Healthcare: An Overview of Challenges and ImprovementsDocument6 pagesLean Principles in Healthcare: An Overview of Challenges and ImprovementsJULIANANo ratings yet
- Core ConceptsDocument6 pagesCore Conceptsnagendra_6391No ratings yet
- Lean Healthcare: Enhancing the Patient Care Process while Eliminating Waste and Lowering CostsFrom EverandLean Healthcare: Enhancing the Patient Care Process while Eliminating Waste and Lowering CostsRating: 5 out of 5 stars5/5 (2)
- Lean ManagmentDocument20 pagesLean Managmentفيصل الاعرجNo ratings yet
- CMA Projet Report Group5Document14 pagesCMA Projet Report Group5anon_218438845No ratings yet
- The Application of Lean in Healthcare: Exploratory PaperDocument40 pagesThe Application of Lean in Healthcare: Exploratory PaperSaraNo ratings yet
- 7 Wastes of Lean in HealthcareDocument5 pages7 Wastes of Lean in HealthcarerheaNo ratings yet
- Quality Control and The Practice of ClinDocument7 pagesQuality Control and The Practice of ClinfranciscoNo ratings yet
- Quality Gurus and Their ContributionDocument17 pagesQuality Gurus and Their ContributionFayis FYSNo ratings yet
- Production and Operation ManagementDocument49 pagesProduction and Operation ManagementIrem AàmarNo ratings yet
- MQA Lab CepDocument19 pagesMQA Lab CepShaffan AbbasiNo ratings yet
- Process Improvement in A Radiology Department: Hatice Camgoz-Akdag and Tu Ğçe BeldekDocument12 pagesProcess Improvement in A Radiology Department: Hatice Camgoz-Akdag and Tu Ğçe BeldekAditya ShuklaNo ratings yet
- Lean Dan 5S Pada Bidang Jasa (Healthcare) PDFDocument9 pagesLean Dan 5S Pada Bidang Jasa (Healthcare) PDFNisaa RahmiNo ratings yet
- TQM Goals and ConceptsDocument5 pagesTQM Goals and ConceptsXavier Scarlet IVNo ratings yet
- Lean Thinking NHSDocument28 pagesLean Thinking NHSHarish VenkatasubramanianNo ratings yet
- Value Stream Mapping CaseDocument13 pagesValue Stream Mapping Casesteve.steinNo ratings yet
- All-Wharton-2009-Rethinking Lean Beyond The Shop Floor PDFDocument18 pagesAll-Wharton-2009-Rethinking Lean Beyond The Shop Floor PDFVishnupriya SharmaNo ratings yet
- Kaizen PDFDocument3 pagesKaizen PDFcs_harsha274280No ratings yet
- Introduction To Total Quality Management: Who Is A Quality Guru?Document9 pagesIntroduction To Total Quality Management: Who Is A Quality Guru?Vaishnavi VaishuNo ratings yet
- Continuous Improvement Strategy: A Learning ApproachDocument11 pagesContinuous Improvement Strategy: A Learning ApproachAdas PapartisNo ratings yet
- Articulo Valido - Principios LEAN LABDocument18 pagesArticulo Valido - Principios LEAN LABFernando Berrospi GarayNo ratings yet
- Effects of Lean Six Sigma in HealthcareDocument6 pagesEffects of Lean Six Sigma in HealthcareYou YouNo ratings yet
- Lean Abstract PDFDocument19 pagesLean Abstract PDFmammutbalajiNo ratings yet
- Uva-Dare (Digital Academic Repository) : Lean Six SigmaDocument9 pagesUva-Dare (Digital Academic Repository) : Lean Six SigmaLuisGutierrezNo ratings yet
- Mistake Proofing HealthcareDocument8 pagesMistake Proofing HealthcareLuis Luchini FernandezNo ratings yet
- Lean Manufacturing Literature ReviewDocument8 pagesLean Manufacturing Literature Reviewea86yezd100% (1)
- Chapter 20Document41 pagesChapter 20Amer RahmahNo ratings yet
- Lean Briefing1912007311331Document13 pagesLean Briefing1912007311331Jorge CardosoNo ratings yet
- 10 - Chapter 3 PDFDocument70 pages10 - Chapter 3 PDFRaghuram Vadiboyena VNo ratings yet
- QI and PDSA Self Learning Packet PA PDFDocument44 pagesQI and PDSA Self Learning Packet PA PDFReli GiusmanNo ratings yet
- Mas YAF (1) TranslationDocument8 pagesMas YAF (1) Translationsaladass 2No ratings yet
- Al Araidah2010Document8 pagesAl Araidah2010jf.leungyanNo ratings yet
- Resumo Alargado Sofia CarvalhoDocument10 pagesResumo Alargado Sofia CarvalhoPatricio Arancibia OrellanaNo ratings yet
- What Is QualityDocument8 pagesWhat Is QualitydzulkormNo ratings yet
- Task#20Document3 pagesTask#20ouia iooNo ratings yet
- Principles and Philosophies of Quality Management: Deming'S Contributions BiographicalDocument15 pagesPrinciples and Philosophies of Quality Management: Deming'S Contributions BiographicalAlbert MervinNo ratings yet
- Lecture 2 Quality AdvocatesDocument71 pagesLecture 2 Quality AdvocatesDOn Ad0% (1)
- Lean Six SigmaDocument8 pagesLean Six Sigma_srobert_No ratings yet
- A Comparative Analysis of Lean Practices and Performance in TheDocument17 pagesA Comparative Analysis of Lean Practices and Performance in TheDanilo Martin Tuppia ReyesNo ratings yet
- Agile Development As A Change Management Approach in Healthcare Innovation ProjectsDocument16 pagesAgile Development As A Change Management Approach in Healthcare Innovation ProjectsAmR ZakiNo ratings yet
- AdvancedTopic OECDocument13 pagesAdvancedTopic OECNoureddine ait el hajNo ratings yet
- Total Quality ImprovementDocument21 pagesTotal Quality ImprovementMar DiyanNo ratings yet
- Kaizen - The Many Ways For Getting BetterDocument6 pagesKaizen - The Many Ways For Getting Betterfahrie_manNo ratings yet
- How Lean Can improve Healthcare? A Brief Guide on Eliminating Waste and Identifying Areas for Improvement: Toyota Production System ConceptsFrom EverandHow Lean Can improve Healthcare? A Brief Guide on Eliminating Waste and Identifying Areas for Improvement: Toyota Production System ConceptsRating: 5 out of 5 stars5/5 (1)
- TQM Legacy of Quality Gurus and Their Theoretical ContributionsDocument18 pagesTQM Legacy of Quality Gurus and Their Theoretical ContributionsAhmadTalibNo ratings yet
- Implementation of The Lean Six Sigma Framework in Non-Profit Organisations A Case StudyDocument18 pagesImplementation of The Lean Six Sigma Framework in Non-Profit Organisations A Case StudyYolandaNo ratings yet
- Total Quality Management PhilosophyDocument34 pagesTotal Quality Management PhilosophyAtharva GuptaNo ratings yet
- A3 Process - A Pragmatic Problem-Solving Technique For Process Improvement in Health CareDocument11 pagesA3 Process - A Pragmatic Problem-Solving Technique For Process Improvement in Health CareNoé HumbertoNo ratings yet
- TQM Assignment 1Document4 pagesTQM Assignment 1hg plNo ratings yet
- Managing in Reverse: The 8 Steps to Optimizing Performance for LeadersFrom EverandManaging in Reverse: The 8 Steps to Optimizing Performance for LeadersNo ratings yet
- How to Manage Future Costs and Risks Using Costing and MethodsFrom EverandHow to Manage Future Costs and Risks Using Costing and MethodsNo ratings yet
- FSnotes 13 To 16Document11 pagesFSnotes 13 To 16Suman Saurabh MohantyNo ratings yet
- Financial Services NotesDocument16 pagesFinancial Services NotesSuman Saurabh MohantyNo ratings yet
- What Is Sustainable DevelopmentDocument14 pagesWhat Is Sustainable Developmentmaverick987No ratings yet
- Driving Indian ConsumptionDocument28 pagesDriving Indian ConsumptionSuman Saurabh MohantyNo ratings yet
- PCLN - Priceline Group Stock Interactive Chart PDFDocument1 pagePCLN - Priceline Group Stock Interactive Chart PDFSuman Saurabh MohantyNo ratings yet
- ETHICS IN PRACTICE: Parable of the SadhuDocument3 pagesETHICS IN PRACTICE: Parable of the SadhuSuman Saurabh MohantyNo ratings yet
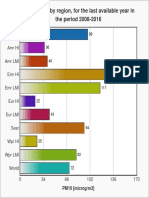
- PM10 air pollution levels by global region 2008-2016Document1 pagePM10 air pollution levels by global region 2008-2016Suman Saurabh MohantyNo ratings yet
- GoingLeaninHealthCareWhitePaper 3 PDFDocument24 pagesGoingLeaninHealthCareWhitePaper 3 PDFyaswanthbhuNo ratings yet
- Project Planning and SchedulingDocument52 pagesProject Planning and SchedulingBatkhishig100% (1)
- Titan Company (TITIND) : Jewellery Segment Growth Expected To SustainDocument11 pagesTitan Company (TITIND) : Jewellery Segment Growth Expected To SustainSuman Saurabh MohantyNo ratings yet
- Introductory MacroeconomicsDocument106 pagesIntroductory MacroeconomicsHardik Gupta50% (4)
- Pricing PredicamentDocument3 pagesPricing PredicamentSuman Saurabh MohantyNo ratings yet
- Exercise 1: Simple I/O Using Keil SimulatorDocument3 pagesExercise 1: Simple I/O Using Keil SimulatorSuman Saurabh MohantyNo ratings yet
- Online Banking Application FormDocument2 pagesOnline Banking Application FormAnkit SahuNo ratings yet
- EMR SchemeDocument44 pagesEMR SchemeSuman Saurabh MohantyNo ratings yet
- Open Banking'S Next Wave: Perspectives From Three Fintech CeosDocument12 pagesOpen Banking'S Next Wave: Perspectives From Three Fintech CeosSuman Saurabh MohantyNo ratings yet
- Hilton CH 10 Select SolutionsDocument25 pagesHilton CH 10 Select Solutionsmanthana9950% (2)
- Embedded Systems - ARM Programming TechniquesDocument258 pagesEmbedded Systems - ARM Programming TechniquesSamir KhNo ratings yet
- Exercise 2: Observing Mode Switching Using A Software InterruptDocument3 pagesExercise 2: Observing Mode Switching Using A Software InterruptSuman Saurabh MohantyNo ratings yet
- LP DegeneracyDocument2 pagesLP DegeneracySuborno AdityaNo ratings yet
- 10 1 1 69Document42 pages10 1 1 69Suman Saurabh MohantyNo ratings yet
- Aichi Biodiversity TargetsDocument3 pagesAichi Biodiversity TargetsSuman Saurabh MohantyNo ratings yet
- L 293 DDocument6 pagesL 293 DSuman Saurabh MohantyNo ratings yet
- VCO1Document3 pagesVCO1Suman Saurabh MohantyNo ratings yet
- 01225959Document6 pages01225959Suman Saurabh MohantyNo ratings yet
- Analysis of Field Programmable Gate Array-Based Kalman Filter ArcDocument123 pagesAnalysis of Field Programmable Gate Array-Based Kalman Filter ArcSuman Saurabh MohantyNo ratings yet
- Ued 495-496 Kelley Shelby Personal Teaching PhilosophyDocument6 pagesUed 495-496 Kelley Shelby Personal Teaching Philosophyapi-295041917No ratings yet
- Core 13 UcspDocument3 pagesCore 13 UcspJanice DomingoNo ratings yet
- Kolkata Thika Tenancy ActDocument15 pagesKolkata Thika Tenancy Actadv123No ratings yet
- 6000 EN 00 04 Friction PDFDocument30 pages6000 EN 00 04 Friction PDFM Ferry AnwarNo ratings yet
- Suretyship and Guaranty CasesDocument47 pagesSuretyship and Guaranty CasesFatima SladjannaNo ratings yet
- Music in The United KingdomDocument33 pagesMusic in The United KingdomIonut PetreNo ratings yet
- Reading Comprehension StrategiesDocument67 pagesReading Comprehension StrategiesKumar ChetanNo ratings yet
- ISO 9001:2015 certified Fargo Courier with over 100 branchesDocument1 pageISO 9001:2015 certified Fargo Courier with over 100 branchesMuchiri NahashonNo ratings yet
- Meaning and Nature of MathematicsDocument3 pagesMeaning and Nature of MathematicsCyril KiranNo ratings yet
- 21st Century Literature Grade 11 21st Century Literature Grade 11 21st Century Literature Grade 11 CompressDocument75 pages21st Century Literature Grade 11 21st Century Literature Grade 11 21st Century Literature Grade 11 Compressdesly jane sianoNo ratings yet
- Sacred SpaceDocument440 pagesSacred SpaceAbdiel Cervantes HernandezNo ratings yet
- Tañada v. Angara Case DigestDocument12 pagesTañada v. Angara Case DigestKatrina PerezNo ratings yet
- UNIT 1 - Revision: HFFFFFDocument3 pagesUNIT 1 - Revision: HFFFFFRedDinoandbluebird ChannelTMNo ratings yet
- 3 Week Lit 121Document48 pages3 Week Lit 121Cassandra Dianne Ferolino MacadoNo ratings yet
- Partition SuitDocument2 pagesPartition SuitJyoti ChaudharyNo ratings yet
- EBM CasesDocument1 pageEBM CasesdnaritaNo ratings yet
- GEO123 Worksheet 8Document4 pagesGEO123 Worksheet 8Hilmi HusinNo ratings yet
- Book Review of Conceptualising Integration in CLIL and Multilingual EducationDocument5 pagesBook Review of Conceptualising Integration in CLIL and Multilingual EducationAigul AitbaevaNo ratings yet
- MC Sampler Pack PDFDocument195 pagesMC Sampler Pack PDFVedaste Ndayishimiye100% (2)
- Gr.8 Ch.5 Chapter Review AnswerDocument10 pagesGr.8 Ch.5 Chapter Review Answerson GokuNo ratings yet
- American Ceramic: SocietyDocument8 pagesAmerican Ceramic: SocietyPhi TiêuNo ratings yet
- Edu 233Document147 pagesEdu 233Abdul Ola IBNo ratings yet
- St. John, Isaac Newton and Prediction of MedicanesDocument6 pagesSt. John, Isaac Newton and Prediction of MedicanesMarthaNo ratings yet
- Whats New SAP HANA Platform Release Notes enDocument66 pagesWhats New SAP HANA Platform Release Notes enJohn Derteano0% (1)
- Theories of StressDocument15 pagesTheories of Stressyared desta100% (1)
- Mock Test 2Document8 pagesMock Test 2Niranjan BeheraNo ratings yet
- Philippine Cartoons: Political Caricatures of the American EraDocument27 pagesPhilippine Cartoons: Political Caricatures of the American EraAun eeNo ratings yet