You might also like
- Infusion Therapy: For Pain, Headache and Related ConditionsFrom EverandInfusion Therapy: For Pain, Headache and Related ConditionsAlaa Abd-ElsayedNo ratings yet
- Statins Nephroprotective EffectDocument5 pagesStatins Nephroprotective EffectGeorgiana FrăţilăNo ratings yet
- Antiplatelet Therapy in Older Adults With Non-ST-Segment Elevation Acute Coronary Syndrome: Considering Risks and BenefitsDocument6 pagesAntiplatelet Therapy in Older Adults With Non-ST-Segment Elevation Acute Coronary Syndrome: Considering Risks and BenefitsJicko Street HooligansNo ratings yet
- Lipid DisorderDocument5 pagesLipid DisorderZahida BashirNo ratings yet
- Hipertension Secundaria Drogas y ToxinasDocument8 pagesHipertension Secundaria Drogas y ToxinasResti SyafitriNo ratings yet
- PIIS0828282X13001530Document4 pagesPIIS0828282X13001530P DORANNo ratings yet
- Ya Qoub Et Al 2023 Upfront Combination of Statin and Ezetimibe For Patients With Acute Coronary Syndrome Time For A NewDocument3 pagesYa Qoub Et Al 2023 Upfront Combination of Statin and Ezetimibe For Patients With Acute Coronary Syndrome Time For A NewPPDS PDL JULI 23No ratings yet
- Antihypertensive Drugs: Re Jackson BSC MB CHB Frca and MC Bellamy MB BS MA FRCA FRCP (Edin) FficmDocument6 pagesAntihypertensive Drugs: Re Jackson BSC MB CHB Frca and MC Bellamy MB BS MA FRCA FRCP (Edin) FficmDwie SeptivianieNo ratings yet
- Less Is More: Catecholamine-Sparing Strategies in Septic ShockDocument3 pagesLess Is More: Catecholamine-Sparing Strategies in Septic Shockmariano villavicencioNo ratings yet
- Intensive Statin Therapy - A Sea Change in Cardiovascular PreventionDocument3 pagesIntensive Statin Therapy - A Sea Change in Cardiovascular Preventionsyaiful rinantoNo ratings yet
- New Drugs and Technologies: PrasugrelDocument10 pagesNew Drugs and Technologies: PrasugrelDewi FitrianaNo ratings yet
- Anaesthetic considerations for patients with advanced malignanciesDocument7 pagesAnaesthetic considerations for patients with advanced malignanciesIrsazulharto Mulana NasutionNo ratings yet
- Statin Treatment in Patients With Intracerebral Hemorrhage: Comments and OpinionsDocument8 pagesStatin Treatment in Patients With Intracerebral Hemorrhage: Comments and OpinionsReyhansyah RachmadhyanNo ratings yet
- Statins: A Review of Benefits and Risks.: Siobhra O'Sullivan, 4th Year MedicineDocument5 pagesStatins: A Review of Benefits and Risks.: Siobhra O'Sullivan, 4th Year MedicinesiddarthpharmaNo ratings yet
- New Insights Into The Statin-Cholesterol Controversy: Timothy M. Marshall, PH.DDocument5 pagesNew Insights Into The Statin-Cholesterol Controversy: Timothy M. Marshall, PH.DFathurrahman AndiyogaNo ratings yet
- Antihypertensive Drugs: Re Jackson BSC MB CHB Frca and MC Bellamy MB BS MA FRCA FRCP (Edin) FficmDocument15 pagesAntihypertensive Drugs: Re Jackson BSC MB CHB Frca and MC Bellamy MB BS MA FRCA FRCP (Edin) FficmAndreas SmfNo ratings yet
- Application of Pharmacognosy in Clinical Practice - Group 5Document26 pagesApplication of Pharmacognosy in Clinical Practice - Group 5Alyssa Nicole PadillaNo ratings yet
- Mycophenolate Mofetil Versus Azathioprine in The Maintenance Therapy of Lupus NephritisDocument6 pagesMycophenolate Mofetil Versus Azathioprine in The Maintenance Therapy of Lupus NephritisdkjoshiameNo ratings yet
- Overcoming Toxicity and Side-Effects of 2014Document14 pagesOvercoming Toxicity and Side-Effects of 2014Andi MuftyNo ratings yet
- Drug StudyDocument9 pagesDrug StudyComia AltheiaNo ratings yet
- Beta Blockers For Congestive Heart Failure: Daulat Manurung, Hana B. TrisnohadiDocument5 pagesBeta Blockers For Congestive Heart Failure: Daulat Manurung, Hana B. TrisnohadiDery ZhibharanyNo ratings yet
- Combination Treatment For HypertensionDocument4 pagesCombination Treatment For HypertensionDewiNo ratings yet
- Expert Opinion On Investigational Drugs: Pharmacology of IrbesartanDocument16 pagesExpert Opinion On Investigational Drugs: Pharmacology of IrbesartanILHAM 'K FOR ALLNo ratings yet
- Wa0067.Document8 pagesWa0067.Daniel FajardoNo ratings yet
- Are Statins Anti-Inflammatory?: Review Gavin J Blake and Paul M RidkerDocument5 pagesAre Statins Anti-Inflammatory?: Review Gavin J Blake and Paul M RidkerPicha PichiNo ratings yet
- Atorvastatin RaDocument2 pagesAtorvastatin RaNejra JonuzNo ratings yet
- Use of Statins in Patients With Chronic Liver Disease and CirrhosisDocument16 pagesUse of Statins in Patients With Chronic Liver Disease and Cirrhosisanindhita90No ratings yet
- Evaluate The Efficacy of Simvastatin and Fluvastatin in Patients With Hypercholesterolemia and Their Effect On Liver FunctionsDocument5 pagesEvaluate The Efficacy of Simvastatin and Fluvastatin in Patients With Hypercholesterolemia and Their Effect On Liver FunctionsfiqaalkasieNo ratings yet
- Update on Managing Oral Surgery Patients on CorticosteroidsDocument12 pagesUpdate on Managing Oral Surgery Patients on CorticosteroidsFadi Al HajjiNo ratings yet
- Methyl PrednisoloneDocument4 pagesMethyl PrednisoloneAnjar WijayadiNo ratings yet
- Clinical Pharamcology HeartDocument0 pagesClinical Pharamcology HeartMamy RafidinarivoNo ratings yet
- 0068C PDFDocument7 pages0068C PDFIntan Kusuma DewiNo ratings yet
- Side Effects of Approved AntidementivesDocument6 pagesSide Effects of Approved AntidementivesAlen BenNo ratings yet
- Statin Therapy, Review of Safety and Potential Side EffectsDocument9 pagesStatin Therapy, Review of Safety and Potential Side EffectsDhita Dwi NandaNo ratings yet
- Zomen in CKDDocument12 pagesZomen in CKDClaudiu BalabanNo ratings yet
- Opa 1Document7 pagesOpa 1Wakum LNo ratings yet
- CLC 4960230910Document7 pagesCLC 4960230910walnut21No ratings yet
- BMJ 2023 075837.fullDocument10 pagesBMJ 2023 075837.fullIgor KhedeNo ratings yet
- Robert ReviewDocument9 pagesRobert ReviewDeden Mulya PrayogaNo ratings yet
- Atorvastatin Improves Cardiac Function and Remodelling in Chronic NonDocument5 pagesAtorvastatin Improves Cardiac Function and Remodelling in Chronic NonRiski Bastanta GintingNo ratings yet
- Review: Jane ArmitageDocument10 pagesReview: Jane ArmitageShafira PutriantiNo ratings yet
- Effect of StatinDocument26 pagesEffect of StatinLaluMuhammadSabarSetiawanNo ratings yet
- Statin Toxicity: ReviewDocument23 pagesStatin Toxicity: ReviewRico AditamaNo ratings yet
- To Compare and Demonstrate The Safety and Efficacy of Antithrombotic Agents and Fibrinolytics in The Management of Acute Coronary SyndromeDocument6 pagesTo Compare and Demonstrate The Safety and Efficacy of Antithrombotic Agents and Fibrinolytics in The Management of Acute Coronary SyndromeInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Update On Management of The Oral and Maxillofacial Surgery Patient On CorticosteroidsDocument12 pagesUpdate On Management of The Oral and Maxillofacial Surgery Patient On Corticosteroidsconstanza gormazNo ratings yet
- Antihypertensives in HDDocument6 pagesAntihypertensives in HDamanyNo ratings yet
- Angio Poster Final 6-30Document6 pagesAngio Poster Final 6-30Alvy SyukrieNo ratings yet
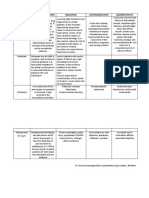
- Drugs Mechanism of Action Indication Contraindication Adverse EffectsDocument2 pagesDrugs Mechanism of Action Indication Contraindication Adverse Effectsisprikitik3No ratings yet
- Intoxicacion Por Betabloqueadores ToxicologyDocument42 pagesIntoxicacion Por Betabloqueadores ToxicologyIza ÁlvarezNo ratings yet
- Kidney News Article p20 7Document2 pagesKidney News Article p20 7ilgarciaNo ratings yet
- And Prevention of Thrombosis, 9th Ed: Antiplatelet Drugs: Antithrombotic TherapyDocument33 pagesAnd Prevention of Thrombosis, 9th Ed: Antiplatelet Drugs: Antithrombotic TherapyNube AzulNo ratings yet
- Pain Management Strategies for Patients With CirrhosisDocument6 pagesPain Management Strategies for Patients With CirrhosisAngélica Valenzuela AndrighiNo ratings yet
- Drug InteracttionDocument8 pagesDrug InteracttionMuh. AnugrawanNo ratings yet
- Trimetazidine ReviewDocument9 pagesTrimetazidine ReviewWasim ShaheenNo ratings yet
- Kristinelou Marie N. Reyna December 29, 2020 BSN 2-6 PharmacologyDocument6 pagesKristinelou Marie N. Reyna December 29, 2020 BSN 2-6 PharmacologyKristinelou Marie ReynaNo ratings yet
- Onsult: Ementia Reatment PdateDocument5 pagesOnsult: Ementia Reatment PdateAxel Robinson HerreraNo ratings yet
- CTTC Estatinas Lancet 2022Document14 pagesCTTC Estatinas Lancet 2022Silvia Montejo FareloNo ratings yet
- New Drugs ArtritisDocument13 pagesNew Drugs ArtritisqfecrespoNo ratings yet
- Efectos 2rios EstatinasDocument2 pagesEfectos 2rios EstatinasFranklin Flórez VidesNo ratings yet
- Novel-Antiplatelet Therapies For Atherothrombotic Diseases: K.malleswari, D.Rama Bramha Reddy, A.Karthikeya SharmaDocument8 pagesNovel-Antiplatelet Therapies For Atherothrombotic Diseases: K.malleswari, D.Rama Bramha Reddy, A.Karthikeya Sharma9493.karthikNo ratings yet
- Clinical Pathways for Acute AppendicitisDocument2 pagesClinical Pathways for Acute AppendicitisFathur RahmanNo ratings yet
- Pleiotropic Effects of StatinsDocument5 pagesPleiotropic Effects of StatinsFathur RahmanNo ratings yet
- JNC 8 Guideline Algorithm for Treating HypertensionDocument2 pagesJNC 8 Guideline Algorithm for Treating HypertensionTaradifaNurInsi0% (1)
- Sexual Disorders ExplainedDocument11 pagesSexual Disorders Explainedluckyswiss7776848No ratings yet
- CP Soft Tissue TumorDocument2 pagesCP Soft Tissue TumorFathur RahmanNo ratings yet
- Daftar Obat Sediaan CairDocument3 pagesDaftar Obat Sediaan CairFathur RahmanNo ratings yet
- Eritroderma DD ManagementDocument7 pagesEritroderma DD ManagementFathur RahmanNo ratings yet
- Anti Anxiety BookletDocument20 pagesAnti Anxiety BookletFathur RahmanNo ratings yet
- 99149246Document11 pages99149246Retma Rosela NurkayantyNo ratings yet
- Erythroderma: UCSF DermatologyDocument27 pagesErythroderma: UCSF DermatologyShida SebelasNo ratings yet
- CHF CpapDocument50 pagesCHF CpapFathur RahmanNo ratings yet
- WHO Manuals of Diagnostic Imaging - Radiographic Anatomy and Interpretation of The Musculoskeletal SystemDocument210 pagesWHO Manuals of Diagnostic Imaging - Radiographic Anatomy and Interpretation of The Musculoskeletal SystemIuliana NitaNo ratings yet
- Role of Renin-Angiotensin System in Endothelial DysfunctionDocument4 pagesRole of Renin-Angiotensin System in Endothelial DysfunctionFathur RahmanNo ratings yet
- Role of Colposcopy in Cervical ErosionDocument112 pagesRole of Colposcopy in Cervical Erosionravikiran1955No ratings yet
- Blue Book PDFDocument126 pagesBlue Book PDFgojo_11No ratings yet
- CancerEpi PDFDocument441 pagesCancerEpi PDFMark EbrahimNo ratings yet
- Schizophrenia NotesDocument8 pagesSchizophrenia NotesAdam WilsonNo ratings yet
- Functional Medicine OverviewDocument28 pagesFunctional Medicine Overviewmdesdoc50% (4)
- ImmunisasiDocument4 pagesImmunisasiJessica LawrenceNo ratings yet
- Prostate Cancer - Risk Stratification and Choice of Initial Treatment - UpToDateDocument30 pagesProstate Cancer - Risk Stratification and Choice of Initial Treatment - UpToDateVictoria KeitelNo ratings yet
- Basic Mycology: Deanna A. SuttonDocument14 pagesBasic Mycology: Deanna A. SuttonGURJEET SINGHNo ratings yet
- Haemostasis TutorialDocument5 pagesHaemostasis TutorialRonaldoNo ratings yet
- Effective Strategies for Stress Reduction in Regressive Autism with The SCIODocument14 pagesEffective Strategies for Stress Reduction in Regressive Autism with The SCIOnamkay_tenzynNo ratings yet
- Comparative - Study - of - The - Major - Component Indigofera PDFDocument9 pagesComparative - Study - of - The - Major - Component Indigofera PDFNur AishaNo ratings yet
- Challenges On Performing LAL Test in Oil Products - Paper No. 95.Document18 pagesChallenges On Performing LAL Test in Oil Products - Paper No. 95.Milan B. ArambasicNo ratings yet
- Disease Prevention Studies by Malaysian EcologistDocument3 pagesDisease Prevention Studies by Malaysian EcologistMohd Zaidi bin HarunNo ratings yet
- Anemia: Linda RottyDocument70 pagesAnemia: Linda RottyKaren MogiNo ratings yet
- Biology 2B - Specimen Paper - Mark SchemeDocument13 pagesBiology 2B - Specimen Paper - Mark Schemezahra zanhar60% (5)
- MomelotinibDocument6 pagesMomelotinibshahd ?No ratings yet
- Mini Nyelvvizsga British Children-AngolnyelvtanitashuDocument3 pagesMini Nyelvvizsga British Children-AngolnyelvtanitashuCsendes ZsófiNo ratings yet
- Tumor MarkersDocument14 pagesTumor MarkersPatrick LizarondoNo ratings yet
- Health and Illness Answer-8Document2 pagesHealth and Illness Answer-8June DumdumayaNo ratings yet
- AfpDocument17 pagesAfpHaris QurashiNo ratings yet
- Aplasia and Hypoplasia of The Radius Studies On 64 Cases and On Epiphyseal Transplantation in Rabbits With The Imitated DefectDocument154 pagesAplasia and Hypoplasia of The Radius Studies On 64 Cases and On Epiphyseal Transplantation in Rabbits With The Imitated DefectJunji Miller FukuyamaNo ratings yet
- Brochure Maxwell 16Document20 pagesBrochure Maxwell 16Linbert Simon CallataNo ratings yet
- Polyploid - WikipediaDocument10 pagesPolyploid - Wikipediaskline3No ratings yet
- Test Bank For Clinical Immunology and Serology A Laboratory Perspective 3rd Edition StevensDocument11 pagesTest Bank For Clinical Immunology and Serology A Laboratory Perspective 3rd Edition StevensWilbur Penny100% (35)
- Focus Life Sciences Grade 10 Exam Practice BookDocument32 pagesFocus Life Sciences Grade 10 Exam Practice BookStars232375% (12)
- Structure and Classification of Viruses ExplainedDocument15 pagesStructure and Classification of Viruses ExplainedMargasatuaNo ratings yet
- Clinical Cases: World Journal ofDocument16 pagesClinical Cases: World Journal ofRhotmy Raúl Escobar GuzmánNo ratings yet
- Benefits of CatnipDocument4 pagesBenefits of CatnipAnnisa SukmasariNo ratings yet
- Append I CitiesDocument12 pagesAppend I CitiesAnonymous lItN37No ratings yet
- Ca 19 9Document3 pagesCa 19 9डा. सत्यदेव त्यागी आर्यNo ratings yet