You might also like
- Reyes, Kay Ma. Pearl Serranilla, Denisa Louise Tan, Francisco III Shivpura Sonia MDocument50 pagesReyes, Kay Ma. Pearl Serranilla, Denisa Louise Tan, Francisco III Shivpura Sonia MGeraldine Marie Salvo100% (1)
- Core Concepts in Clinical Infectious Diseases (CCCID)From EverandCore Concepts in Clinical Infectious Diseases (CCCID)Rating: 5 out of 5 stars5/5 (2)
- BioassayDocument38 pagesBioassayMuhammad Masoom AkhtarNo ratings yet
- SAP FICO Resume - Exp - 3.5 YearsDocument3 pagesSAP FICO Resume - Exp - 3.5 Yearsranga67% (3)
- DENGUE HEMORRHAGIC FEVER-final N ToDocument52 pagesDENGUE HEMORRHAGIC FEVER-final N ToRachel Ann CorpuzNo ratings yet
- Characteristics of An Effective CounselorDocument5 pagesCharacteristics of An Effective CounselorAbbas KhanNo ratings yet
- MICEDocument37 pagesMICECeleste Torino DigalNo ratings yet
- DengueDocument99 pagesDengueJames DavidNo ratings yet
- Methods Used in EpidemologyDocument53 pagesMethods Used in EpidemologySameera banuNo ratings yet
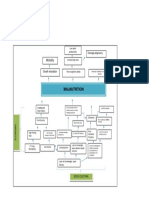
- Problem Tree Analysis MalnutritionDocument1 pageProblem Tree Analysis MalnutritionMho Dsb50% (6)
- Sell More, Serve BetterDocument39 pagesSell More, Serve BetterSalesMantra CRM100% (4)
- Pasyon and RevolutionDocument2 pagesPasyon and RevolutionBilly JoeNo ratings yet
- Epidemiology With Part 2 (Complete) 2Document59 pagesEpidemiology With Part 2 (Complete) 2nahNo ratings yet
- Bioentrepreneurship 2018 OBTL Course Plan (Rev)Document17 pagesBioentrepreneurship 2018 OBTL Course Plan (Rev)Ellah GutierrezNo ratings yet
- Lac Session For TeachersDocument1 pageLac Session For TeachersXer WinchesterNo ratings yet
- Dengue ThesisDocument5 pagesDengue ThesisPat Vierneza-Calalang100% (2)
- DEPED-INDIVIDUAL-WORKWEEK-ACCOMPLISHMENT-REPORT Rex JULYDocument5 pagesDEPED-INDIVIDUAL-WORKWEEK-ACCOMPLISHMENT-REPORT Rex JULYXer Winchester100% (1)
- Health Communication BJMCDocument42 pagesHealth Communication BJMCxyz_171274767100% (3)
- Yboa and Ladrague With Questionnaire On Knowledge and PracticeDocument6 pagesYboa and Ladrague With Questionnaire On Knowledge and PracticeXer WinchesterNo ratings yet
- The Problem and Its ScopeDocument59 pagesThe Problem and Its ScopeRochelle GallofinNo ratings yet
- Introduction of Research Paper About DengueDocument5 pagesIntroduction of Research Paper About Denguejhwmemrhf100% (1)
- Research Imd 21 Section A: Topic: Dengue FeverDocument15 pagesResearch Imd 21 Section A: Topic: Dengue FeverAayush KhanvilkarNo ratings yet
- Knowledge, Attitudes and Practices of Nursing Students on Dengue FeverDocument9 pagesKnowledge, Attitudes and Practices of Nursing Students on Dengue FeverElinNo ratings yet
- Example of Research Paper About Dengue FeverDocument5 pagesExample of Research Paper About Dengue Feverfysxfjac100% (1)
- Jose Research v2Document10 pagesJose Research v2Jose Emmanuel FranciaNo ratings yet
- Research Paper On Dengue VirusDocument6 pagesResearch Paper On Dengue Virusfvgy6fn3100% (1)
- Research Paper On Dengue FeverDocument5 pagesResearch Paper On Dengue Feverz1h1dalif0n3100% (1)
- WHO Dengue Bulletin Vol 24 Dec 2000Document3 pagesWHO Dengue Bulletin Vol 24 Dec 2000Tapojyoti DasNo ratings yet
- Research Papers Related To Dengue FeverDocument7 pagesResearch Papers Related To Dengue Feverc9rvz6mm100% (1)
- Term Paper EpidemiologyDocument8 pagesTerm Paper Epidemiologyc5m07hh9100% (1)
- Thesis EpidemiologyDocument6 pagesThesis Epidemiologykatieparkersaintpaul100% (3)
- Dịch Tễ HọcDocument4 pagesDịch Tễ HọcPhuong AnhNo ratings yet
- Mathematical Modeling of Hand-Foot-Mouth Disease: Quarantine As A Control MeasureDocument11 pagesMathematical Modeling of Hand-Foot-Mouth Disease: Quarantine As A Control MeasureAisah AisahNo ratings yet
- Epidemiological Risk Factors For Adult Dengue in Singapore: An 8-Year Nested Test Negative Case Control StudyDocument9 pagesEpidemiological Risk Factors For Adult Dengue in Singapore: An 8-Year Nested Test Negative Case Control StudydouwesdNo ratings yet
- A. Current Trends About The Disease ConditionDocument35 pagesA. Current Trends About The Disease ConditionVina LaurelNo ratings yet
- Leptospirosis CompiledDocument76 pagesLeptospirosis CompiledTine Mendoza100% (1)
- Dengue Infection in Children in Ratchaburi, Thailand: A Cohort Study. II. Clinical ManifestationsDocument11 pagesDengue Infection in Children in Ratchaburi, Thailand: A Cohort Study. II. Clinical ManifestationsMey KhNo ratings yet
- Tuberculosis Thesis IntroductionDocument8 pagesTuberculosis Thesis Introductionifywpqvcf100% (2)
- Epidemiology PHD Thesis PDFDocument6 pagesEpidemiology PHD Thesis PDFxnehytwff100% (1)
- Data Analysis Plan On The Association Between Socio Economic and Demographic Factors and Dengue Fever Infection PDFDocument8 pagesData Analysis Plan On The Association Between Socio Economic and Demographic Factors and Dengue Fever Infection PDFKeshab RijalNo ratings yet
- PHR211Public Health: EpidemiologyDocument59 pagesPHR211Public Health: EpidemiologyNuhu SibaNo ratings yet
- Epidemiology Thesis PDFDocument6 pagesEpidemiology Thesis PDFafknojbcf100% (2)
- Research Paper On Dengue Fever in PakistanDocument6 pagesResearch Paper On Dengue Fever in Pakistangvzz4v44100% (1)
- Tuberculosis Thesis TopicsDocument7 pagesTuberculosis Thesis Topicsstacyjohnsonreno100% (2)
- Group 1 ResearchDocument11 pagesGroup 1 ResearchFelix RemillosaNo ratings yet
- Dengue Fever Impact of Knowledge On Preventive PracticeDocument7 pagesDengue Fever Impact of Knowledge On Preventive PracticeteddyNo ratings yet
- Tidak Ada Kejadian Tifoid 3Document3 pagesTidak Ada Kejadian Tifoid 3ilhamNo ratings yet
- J Infect Dis.-2016-Dengue Vaccine The Need, The Challenges, and ProgressDocument3 pagesJ Infect Dis.-2016-Dengue Vaccine The Need, The Challenges, and ProgressRaja Ahmad Rusdan MusyawirNo ratings yet
- Review of Literature On Dengue Fever in IndiaDocument9 pagesReview of Literature On Dengue Fever in Indial1wot1j1fon3100% (1)
- NBHS2332 Learning KitDocument36 pagesNBHS2332 Learning Kitshinichi kudoNo ratings yet
- Awareness of Dengue and Practice of Dengue Control Among1Document6 pagesAwareness of Dengue and Practice of Dengue Control Among1rjohn 7No ratings yet
- Sample Research Paper On DengueDocument4 pagesSample Research Paper On Denguelyn0l1gamop2100% (3)
- Capitol University Case Study on Dengue SevereDocument67 pagesCapitol University Case Study on Dengue SevereTyron ChuaNo ratings yet
- Literature Review of Pneumonia Under Five YearDocument6 pagesLiterature Review of Pneumonia Under Five Yeare9xy1xsv100% (1)
- Literature Review On Typhoid FeverDocument4 pagesLiterature Review On Typhoid Feverc5h4drzjNo ratings yet
- Report On Pandemic InfluenzaDocument32 pagesReport On Pandemic InfluenzaFhan Sani SeowNo ratings yet
- Unit 1.1 - Introduction To EpidemiologiDocument21 pagesUnit 1.1 - Introduction To EpidemiologiBENNY BAKARNo ratings yet
- This Module: Covers The Knowledge, Skills and AttitudesDocument13 pagesThis Module: Covers The Knowledge, Skills and AttitudesmeysNo ratings yet
- STD Research Paper TopicsDocument7 pagesSTD Research Paper Topicsgz8pheje100% (1)
- Epi Descriptive Study DesignsDocument4 pagesEpi Descriptive Study DesignsAndrea BardalesNo ratings yet
- Tuberculosis Research Paper ExampleDocument4 pagesTuberculosis Research Paper Exampled1fytyt1man3100% (1)
- Level of Consciousness and Health Protocols at Home Among Students of Polytechnic College of BotolanDocument7 pagesLevel of Consciousness and Health Protocols at Home Among Students of Polytechnic College of BotolanAJHSSR JournalNo ratings yet
- Dengue Fever Journal 1Document10 pagesDengue Fever Journal 1aurazhavaNo ratings yet
- Epidemiology Thesis PaperDocument4 pagesEpidemiology Thesis Paperlindsayalstonatlanta100% (2)
- Tugas Ulang Metodologi PenelitianDocument55 pagesTugas Ulang Metodologi PenelitianMuhammad Candra R.ANo ratings yet
- Epidemiology Dissertation TopicsDocument4 pagesEpidemiology Dissertation TopicsHelpWritingCollegePapersDesMoines100% (1)
- Epidemiology Course WorkDocument4 pagesEpidemiology Course Workafjwdkwmdbqegq100% (2)
- EPI Lecture1Document43 pagesEPI Lecture1Margaret SannohNo ratings yet
- Tugas Merangkum Epidemiologi Safira M.20.02.050Document5 pagesTugas Merangkum Epidemiologi Safira M.20.02.050safira saalNo ratings yet
- CHN 2Document13 pagesCHN 2Claire Maurice JuaneroNo ratings yet
- Diagnosis and Treatment of Chronic CoughFrom EverandDiagnosis and Treatment of Chronic CoughSang Heon ChoNo ratings yet
- Republic of The Philippines Department of Education Region VI - Western Visayas Schools Division of Capiz Pob. Ilaya, Dao, CapizDocument1 pageRepublic of The Philippines Department of Education Region VI - Western Visayas Schools Division of Capiz Pob. Ilaya, Dao, CapizXer WinchesterNo ratings yet
- ACCOMPLISHMENT REPORT OCTOBER 3 COPIES - New FormatDocument4 pagesACCOMPLISHMENT REPORT OCTOBER 3 COPIES - New FormatXer WinchesterNo ratings yet
- Individual Daily Log and Accomplishment Report: Enclosure No. 3 To Deped Order No. 011, S. 2020Document1 pageIndividual Daily Log and Accomplishment Report: Enclosure No. 3 To Deped Order No. 011, S. 2020Xer WinchesterNo ratings yet
- Individual Daily Log and Accomplishment Report: Enclosure No. 3 To Deped Order No. 011, S. 2020Document2 pagesIndividual Daily Log and Accomplishment Report: Enclosure No. 3 To Deped Order No. 011, S. 2020Xer WinchesterNo ratings yet
- Individual Daily Log and Accomplishment Report: Enclosure No. 3 To Deped Order No. 011, S. 2020Document1 pageIndividual Daily Log and Accomplishment Report: Enclosure No. 3 To Deped Order No. 011, S. 2020Xer WinchesterNo ratings yet
- DepEd Capiz School Supervision ReportsDocument1 pageDepEd Capiz School Supervision ReportsXer WinchesterNo ratings yet
- Republic of The Philippines Department of Education Region VI - Western Visayas Schools Division of Capiz Pob. Ilaya, Dao, CapizDocument1 pageRepublic of The Philippines Department of Education Region VI - Western Visayas Schools Division of Capiz Pob. Ilaya, Dao, CapizXer WinchesterNo ratings yet
- Maindang National High School: Republic of The PhilippinesDocument1 pageMaindang National High School: Republic of The PhilippinesXer WinchesterNo ratings yet
- The Philippines Is Home To Many Endemic Species - and Many Endangered Ones. Learn More About Endangered Animals in The PhilippinesDocument4 pagesThe Philippines Is Home To Many Endemic Species - and Many Endangered Ones. Learn More About Endangered Animals in The PhilippinesXer WinchesterNo ratings yet
- DepEd Daily Log ReportDocument1 pageDepEd Daily Log ReportXer WinchesterNo ratings yet
- Environmental LawsDocument5 pagesEnvironmental LawsXer WinchesterNo ratings yet
- Individual Daily Log and Accomplishment Report: Enclosure No. 3 To Deped Order No. 011, S. 2020Document1 pageIndividual Daily Log and Accomplishment Report: Enclosure No. 3 To Deped Order No. 011, S. 2020Xer WinchesterNo ratings yet
- RM No. 127, s.2015 Unified SHS Schedule of SubjectsDocument3 pagesRM No. 127, s.2015 Unified SHS Schedule of SubjectsJennPete Refol100% (3)
- Individual Daily Log and Accomplishment Report: Enclosure No. 3 To Deped Order No. 011, S. 2020Document1 pageIndividual Daily Log and Accomplishment Report: Enclosure No. 3 To Deped Order No. 011, S. 2020Xer WinchesterNo ratings yet
- Individual Daily Log and Accomplishment Report: Enclosure No. 3 To Deped Order No. 011, S. 2020Document2 pagesIndividual Daily Log and Accomplishment Report: Enclosure No. 3 To Deped Order No. 011, S. 2020Xer WinchesterNo ratings yet
- Individual Daily Log and Accomplishment Report: Enclosure No. 3 To Deped Order No. 011, S. 2020Document1 pageIndividual Daily Log and Accomplishment Report: Enclosure No. 3 To Deped Order No. 011, S. 2020Xer WinchesterNo ratings yet
- Science Research ProposalDocument2 pagesScience Research ProposalXer WinchesterNo ratings yet
- Cover Title FINAL ORAL DEFENSEDocument1 pageCover Title FINAL ORAL DEFENSEXer WinchesterNo ratings yet
- History of MagnetismDocument1 pageHistory of MagnetismXer WinchesterNo ratings yet
- DepEd Daily Log ReportDocument2 pagesDepEd Daily Log ReportXer WinchesterNo ratings yet
- Table of ContentsDocument2 pagesTable of ContentsXer WinchesterNo ratings yet
- Z Scilympics GuidelinesDocument2 pagesZ Scilympics GuidelinesXer Winchester100% (2)
- Solar System Model Explains Day and NightDocument46 pagesSolar System Model Explains Day and NightXer WinchesterNo ratings yet
- Boys and Girls TarpDocument1 pageBoys and Girls TarpXer WinchesterNo ratings yet
- SchooldisciplinerulesofprocedureDocument41 pagesSchooldisciplinerulesofprocedureLexter Jimenez ResullarNo ratings yet
- Board WorkDocument2 pagesBoard WorkXer WinchesterNo ratings yet
- European Management Journal: Rainer Lueg, Ronny RadlachDocument14 pagesEuropean Management Journal: Rainer Lueg, Ronny RadlachPutri MutiraNo ratings yet
- Evangelion Cruel Angels Thesis - Moonbase AlphaDocument5 pagesEvangelion Cruel Angels Thesis - Moonbase Alphasionothewil1977100% (1)
- Ethics in BankingDocument8 pagesEthics in BankingMarwa AleiaiwiNo ratings yet
- Support Groups: Social NetworksDocument1 pageSupport Groups: Social NetworksSoulja boy BIG GUCCI DracoNo ratings yet
- Guía BaccettiDocument11 pagesGuía BaccettiPercy Andree Bayona GuillermoNo ratings yet
- The Lair of Arachas - A Mausritter AdventureDocument8 pagesThe Lair of Arachas - A Mausritter AdventureGladstone PinheiroNo ratings yet
- Unit 11 Multiple Correlation: StructureDocument18 pagesUnit 11 Multiple Correlation: StructurePranav ViswanathanNo ratings yet
- DinithDocument102 pagesDinithVishmi amashaNo ratings yet
- Emergency Mang TraumaDocument16 pagesEmergency Mang Traumaeliemaalouf4No ratings yet
- Pityriasis Versicolor: Avoiding Pitfalls in Disease Diagnosis and TherapyDocument3 pagesPityriasis Versicolor: Avoiding Pitfalls in Disease Diagnosis and TherapypanduNo ratings yet
- Dr. Kirti MatliwalaDocument6 pagesDr. Kirti MatliwalaKirti Dakshesh ThakarNo ratings yet
- Dokumen - Tips - Ielts and Toefl Made Easy George John Efc and Is The First Coherence PDFDocument2 pagesDokumen - Tips - Ielts and Toefl Made Easy George John Efc and Is The First Coherence PDFPayal SethiNo ratings yet
- Unit 5 Math-Parent Letter-4th GradeDocument4 pagesUnit 5 Math-Parent Letter-4th Gradeapi-346081420No ratings yet
- Department of Mathematics at Columbia University - Calculus II Sample Syllabus PDFDocument2 pagesDepartment of Mathematics at Columbia University - Calculus II Sample Syllabus PDFKaka AsefNo ratings yet
- Transits of The Year 2008: Text by Robert HandDocument27 pagesTransits of The Year 2008: Text by Robert HandjasminnexNo ratings yet
- Tle Fos 9 11 q1 WK 7 d1Document6 pagesTle Fos 9 11 q1 WK 7 d1REYMOND SUMAYLONo ratings yet
- Philippine Supreme Court Decisions on Constitutionality of LawsDocument64 pagesPhilippine Supreme Court Decisions on Constitutionality of Lawswesternwound82No ratings yet
- FORMS Transaction DisputeDocument1 pageFORMS Transaction DisputeKristine Cruz-MaltoNo ratings yet
- ReportDocument3 pagesReportPrecious Anne MacalinoNo ratings yet
- MA Urdu Revised Syllabus 2022-23Document35 pagesMA Urdu Revised Syllabus 2022-23Mazhar KhanNo ratings yet
- Ch1 - Part I - Meaning of ResearchDocument36 pagesCh1 - Part I - Meaning of ResearchKirubel MulugetaNo ratings yet