You might also like
- Tinea Corporis, Tinea Cruris, Tinea Nigra, and PiedraDocument6 pagesTinea Corporis, Tinea Cruris, Tinea Nigra, and PiedraIsni KhoirunisaNo ratings yet
- Antifungal Therapy for Fungal InfectionsDocument186 pagesAntifungal Therapy for Fungal InfectionsRizweta DestinNo ratings yet
- S0733 8635 2803 2900032 920160621 22881 1su0moo With Cover Page v2Document33 pagesS0733 8635 2803 2900032 920160621 22881 1su0moo With Cover Page v2Alfian DjaafaraNo ratings yet
- Severe DermatoDocument13 pagesSevere DermatoadriantiariNo ratings yet
- Topical Treatment of Common Superficial Tinea InfectionsDocument8 pagesTopical Treatment of Common Superficial Tinea InfectionsColate LocoNo ratings yet
- Management of Tinea Corporis, Tinea Cruris, and Tinea Pedis: A Comprehensive ReviewDocument19 pagesManagement of Tinea Corporis, Tinea Cruris, and Tinea Pedis: A Comprehensive ReviewYovitaNo ratings yet
- PDF DocumentDocument4 pagesPDF DocumentAditya Yudha PratamaNo ratings yet
- Medical MycologyDocument14 pagesMedical Mycologyhawkar omerNo ratings yet
- Tinea Capitis: Fungal Infection of the ScalpDocument16 pagesTinea Capitis: Fungal Infection of the ScalpIkram IkramNo ratings yet
- Pharmaceutical Microbiology and Parasitology (PHMP211)Document59 pagesPharmaceutical Microbiology and Parasitology (PHMP211)Crisamor Rose Pareja ClarisaNo ratings yet
- BAHAN Tinea CapitisDocument28 pagesBAHAN Tinea CapitisYorika HafelaniNo ratings yet
- Acral Manifestations of Fungal InfectionsDocument21 pagesAcral Manifestations of Fungal InfectionsanwarNo ratings yet
- M13 - Dermatology - Chapter 5Document11 pagesM13 - Dermatology - Chapter 5Idham BaharudinNo ratings yet
- Cutaneous Mycoses MikologiDocument10 pagesCutaneous Mycoses MikologisherinaNo ratings yet
- Tinea Capitis in AdultsDocument7 pagesTinea Capitis in Adultsdimasarya671No ratings yet
- Tinea Kruris BahanDocument11 pagesTinea Kruris BahanFebridayanti Nur FitriannisaNo ratings yet
- Hubungan Wilayah Kerja Terhadap Kejadian Jamur Pada Karyawan PT - Perkebunan Nusantara ViiDocument7 pagesHubungan Wilayah Kerja Terhadap Kejadian Jamur Pada Karyawan PT - Perkebunan Nusantara ViiLedya Esya HestariNo ratings yet
- Antifungal DrugsDocument16 pagesAntifungal DrugsAmrinder SagguNo ratings yet
- Defi Nition and NomenclatureDocument4 pagesDefi Nition and NomenclatureintanphNo ratings yet
- Super Ficial Fungal Infections: Key PointsDocument4 pagesSuper Ficial Fungal Infections: Key PointsBagus Putra KurniawanNo ratings yet
- Fungal Infection of The SkinDocument74 pagesFungal Infection of The Skinary_puraNo ratings yet
- Cutaneous Fungal InfectionsDocument8 pagesCutaneous Fungal InfectionsJudith GraalNo ratings yet
- Bab IDocument24 pagesBab ISinta Rahmah SariNo ratings yet
- Cutaneous Larva MigransDocument4 pagesCutaneous Larva MigransanissabilfaqihNo ratings yet
- The Kerion An Angry Tinea Capitis PBDocument7 pagesThe Kerion An Angry Tinea Capitis PBprajnamitaNo ratings yet
- Tinea Pedis An UpdateDocument5 pagesTinea Pedis An UpdateRahmat MuliaNo ratings yet
- Tinea Capitis: Current Review of The Literature: EpidemiologyDocument7 pagesTinea Capitis: Current Review of The Literature: EpidemiologyameliaNo ratings yet
- Tinea Pedis - An Update: September 2011Document6 pagesTinea Pedis - An Update: September 2011Disty Aldilla WicaksonoNo ratings yet
- Tinea pedis: More than just athlete's footDocument6 pagesTinea pedis: More than just athlete's footNyoman Arya Adi WangsaNo ratings yet
- AdrianDocument3 pagesAdrianJohn David ZabalaNo ratings yet
- Dermatophytosis: EtiologyDocument6 pagesDermatophytosis: EtiologyTheresia FalentinaNo ratings yet
- Intertrigo and Secondary Skin InfectionsDocument5 pagesIntertrigo and Secondary Skin Infectionskhalizamaulina100% (1)
- An Overview of Fungal Infections: Gary GarberDocument2 pagesAn Overview of Fungal Infections: Gary GarberSUBHADIPNo ratings yet
- Managing Athlete's FootDocument5 pagesManaging Athlete's FootCharlesMahonoNo ratings yet
- Tinea Corporis Pedia-1Document11 pagesTinea Corporis Pedia-1Denso Antonius LimNo ratings yet
- Fungal Skin Infections GuideDocument12 pagesFungal Skin Infections GuideHassan kamalNo ratings yet
- E Tra: Diagnosis and Management of Cutaneous Tinea InfectionsDocument8 pagesE Tra: Diagnosis and Management of Cutaneous Tinea InfectionsFuad hadyanNo ratings yet
- MycosisDocument3 pagesMycosisMartin Ponce de León100% (1)
- Chemotherapy of Fungal DiseasesDocument51 pagesChemotherapy of Fungal DiseasesSalmaan KhanNo ratings yet
- Fungal InfectionsDocument9 pagesFungal InfectionsCoral Srinivasa RamaluNo ratings yet
- Tinea Infections: Changing Face or Neglected?: Laura Atzori, Laura Pizzatti and Monica PauDocument7 pagesTinea Infections: Changing Face or Neglected?: Laura Atzori, Laura Pizzatti and Monica PauRisma AnjelinaNo ratings yet
- Dermatomikosis JurnalDocument6 pagesDermatomikosis JurnalNuciana Siti Andrianti100% (1)
- Chronic DermatophytosisDocument4 pagesChronic DermatophytosisLiana BegNo ratings yet
- Dermatophyte Infections: Types, Causes, Symptoms and TreatmentDocument59 pagesDermatophyte Infections: Types, Causes, Symptoms and Treatmentحسين طاهر حاتم طاهرNo ratings yet
- What Are CutaneDocument6 pagesWhat Are CutaneTayech TilahunNo ratings yet
- Ccid 11 175Document11 pagesCcid 11 175Remo Alnovryanda PutraNo ratings yet
- Tinea FasialisDocument8 pagesTinea FasialisFelix Tortora SekaiNo ratings yet
- DermatophytesDocument10 pagesDermatophytesRaunaNo ratings yet
- Tinea Pedis1Document7 pagesTinea Pedis1Ryan ChambersNo ratings yet
- Ringworm Infection in Dogs and Cats: In: Recent Advances in Canine Infectious Diseases, L. Carmichael (Ed.)Document7 pagesRingworm Infection in Dogs and Cats: In: Recent Advances in Canine Infectious Diseases, L. Carmichael (Ed.)Auni IbrahimNo ratings yet
- Tinea Corporis, Caused by Microsporum Canis - A Case Report From KosovoDocument2 pagesTinea Corporis, Caused by Microsporum Canis - A Case Report From KosovoAsterlita RyaneNo ratings yet
- Scabies: Signs and SymptomsDocument5 pagesScabies: Signs and Symptomsputri intanNo ratings yet
- Chapter 42: Fungal Skin Infections: Handbook of Nonprescription Drugs: An Interactive Approach To Self-Care, 20th EditionDocument22 pagesChapter 42: Fungal Skin Infections: Handbook of Nonprescription Drugs: An Interactive Approach To Self-Care, 20th EditionOmnia El HossienyNo ratings yet
- Cutaneous Fungal Infections MechanismDocument50 pagesCutaneous Fungal Infections MechanismBenediktus BayuNo ratings yet
- Tinea corporis and tinea cruris case caused by Trichophyton mentagrophytes type granularDocument8 pagesTinea corporis and tinea cruris case caused by Trichophyton mentagrophytes type granularMaisura RaRaNo ratings yet
- Diagnosis and Management of Common Tinea InfectionsDocument23 pagesDiagnosis and Management of Common Tinea InfectionsGiovanni AnggastaNo ratings yet
- Superficial Fungal Infections: Auroba K. Abbas, PH.D., Zahraa A. Mohammed, M.SC., Imad S. Mahmoud, PH.DDocument3 pagesSuperficial Fungal Infections: Auroba K. Abbas, PH.D., Zahraa A. Mohammed, M.SC., Imad S. Mahmoud, PH.DAnonymous zNUqQaNo ratings yet
- 1f97 PDFDocument8 pages1f97 PDFIqbal AbdillahNo ratings yet
- A Simple Guide to Skin Fungal Infections, (Updated 2023) Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Skin Fungal Infections, (Updated 2023) Diagnosis, Treatment and Related ConditionsRating: 5 out of 5 stars5/5 (2)
- Cervical CancerDocument60 pagesCervical CancerNova Yuli PrasetyoNo ratings yet
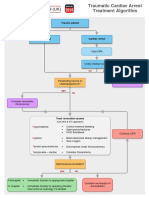
- G2015 Traumatic Cardiac Arrest TreatmentDocument1 pageG2015 Traumatic Cardiac Arrest TreatmentDicky KurniawanNo ratings yet
- PCR & TCM Patklin PDFDocument25 pagesPCR & TCM Patklin PDFA.B. Saleem VinZuelaNo ratings yet
- Pentabio PDFDocument7 pagesPentabio PDFDicky KurniawanNo ratings yet
- General Aspects On Post Partum Care of Laparoschisis in NewbornsDocument8 pagesGeneral Aspects On Post Partum Care of Laparoschisis in NewbornsErica DagdagNo ratings yet
- METHOD Gotz Bothe TermorregulacionDocument22 pagesMETHOD Gotz Bothe TermorregulacionLindolfo Euqueres100% (1)
- Dairy SheepDocument16 pagesDairy SheepsatrianasajaNo ratings yet
- Dermatology RevisionDocument7 pagesDermatology RevisionmksharmaaNo ratings yet
- Presented by DR - Asha V Sasi 2 MD CR DeptDocument32 pagesPresented by DR - Asha V Sasi 2 MD CR DeptSariIdaMihartiNo ratings yet
- The Contents of Anatomical Snuff Box AreDocument3 pagesThe Contents of Anatomical Snuff Box AreZimam ZamriNo ratings yet
- Vitamins and MineralsDocument25 pagesVitamins and MineralsFyan FiradyNo ratings yet
- Bosnian Fortune Telling in The Coffee CupDocument3 pagesBosnian Fortune Telling in The Coffee CupzemerijasNo ratings yet
- Anatomy of The Excretory SystemDocument6 pagesAnatomy of The Excretory SystemCherry Grace Articulo DabuconNo ratings yet
- Hepatitis ADocument1 pageHepatitis AGary Detman100% (1)
- Lesson 5 Connective TissueDocument5 pagesLesson 5 Connective Tissueshairene PiaNo ratings yet
- A Review of The Relationship Between Hoof Trimming and Dairy Cattle WelfareDocument11 pagesA Review of The Relationship Between Hoof Trimming and Dairy Cattle WelfareguadialvarezNo ratings yet
- Understanding AnovulationDocument207 pagesUnderstanding AnovulationRosu George100% (2)
- Mendelian Genetics and ExtensionsDocument39 pagesMendelian Genetics and ExtensionskcqywNo ratings yet
- Simon'S Cookery Course: The Alternative Guide To Cooking - Survival or OtherwiseDocument32 pagesSimon'S Cookery Course: The Alternative Guide To Cooking - Survival or OtherwiseAengus RyanNo ratings yet
- Anatomy Large IntestineDocument4 pagesAnatomy Large IntestinetristineNo ratings yet
- Bombay CatDocument2 pagesBombay CatprosvetiteljNo ratings yet
- Fish Physiology and Biochemistry MFSC SyllabusDocument19 pagesFish Physiology and Biochemistry MFSC SyllabusngonguyenminhtuanNo ratings yet
- Food Sources: PlantsDocument10 pagesFood Sources: PlantsGreBaptistChristianPre-SchoolNo ratings yet
- @santoselizabeth 96Document2 pages@santoselizabeth 96ZabNo ratings yet
- Daftar Pustaka Lo SK 4 KardioDocument3 pagesDaftar Pustaka Lo SK 4 KardioGraceNo ratings yet
- HSC Zoology Board Paper 2013Document2 pagesHSC Zoology Board Paper 2013Sachin DedhiaNo ratings yet
- The Physiological Changes of PregnancyDocument16 pagesThe Physiological Changes of PregnancycchaitukNo ratings yet
- Collective NounsDocument11 pagesCollective NounsphumpherNo ratings yet
- DR - Majid NotesDocument16 pagesDR - Majid NotesSandeep Sasidharan100% (1)
- Breathing Secrets v1-2Document34 pagesBreathing Secrets v1-2Eduardo100% (4)
- Recording Structure of MammalsDocument334 pagesRecording Structure of Mammalsfransiskus.rada24No ratings yet
- Seminar Presentation Plus Ultra 10%Document10 pagesSeminar Presentation Plus Ultra 10%Adaeze Ezem-NjokuNo ratings yet
- Mechanisms of Pain MUIRDocument11 pagesMechanisms of Pain MUIRLorena B-iNo ratings yet
- Philippines Tuberculosis ProfileDocument4 pagesPhilippines Tuberculosis ProfileElica Bolhano NarcisoNo ratings yet