You might also like
- A Simple Guide to Skin Fungal Infections, (Updated 2023) Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Skin Fungal Infections, (Updated 2023) Diagnosis, Treatment and Related ConditionsRating: 5 out of 5 stars5/5 (2)
- Dermatophytosis: EtiologyDocument6 pagesDermatophytosis: EtiologyTheresia FalentinaNo ratings yet
- Cutaneous Mycoses MikologiDocument10 pagesCutaneous Mycoses MikologisherinaNo ratings yet
- Tinea Corporis Pedia-1Document11 pagesTinea Corporis Pedia-1Denso Antonius LimNo ratings yet
- Fungal Infection of The SkinDocument74 pagesFungal Infection of The Skinary_puraNo ratings yet
- Cutaneous Mycoses Guide: Classification, Agents and Clinical ManifestationsDocument56 pagesCutaneous Mycoses Guide: Classification, Agents and Clinical ManifestationsHafsa ImranNo ratings yet
- Fungal Pathogens GroupingsDocument25 pagesFungal Pathogens GroupingsJhade Rio GadinganNo ratings yet
- Dermatophytes - Medical Research Institute - Alexandria UniversityDocument129 pagesDermatophytes - Medical Research Institute - Alexandria Universityማላያላም ማላያላምNo ratings yet
- DermatophyteDocument8 pagesDermatophyteBhuvana RajNo ratings yet
- Diagnosis and Management of Common Tinea InfectionsDocument23 pagesDiagnosis and Management of Common Tinea InfectionsGiovanni AnggastaNo ratings yet
- Fungi of Medical ImportanceDocument11 pagesFungi of Medical ImportanceRi FitrianaNo ratings yet
- Dermatophytosis: LectureDocument35 pagesDermatophytosis: LectureGideon MukalaziNo ratings yet
- Pharmaceutical Microbiology and Parasitology (PHMP211)Document59 pagesPharmaceutical Microbiology and Parasitology (PHMP211)Crisamor Rose Pareja ClarisaNo ratings yet
- Bab IDocument24 pagesBab ISinta Rahmah SariNo ratings yet
- Severe DermatoDocument13 pagesSevere DermatoadriantiariNo ratings yet
- Myco - 05 - Dermatophyte & AsperagillusDocument92 pagesMyco - 05 - Dermatophyte & AsperagillusesraaNo ratings yet
- DermatomycosesDocument32 pagesDermatomycosesp6hccq6jd7No ratings yet
- AdrianDocument3 pagesAdrianJohn David ZabalaNo ratings yet
- MycologyyyyyyyyyyyyyyDocument12 pagesMycologyyyyyyyyyyyyyyNyxa AbdullaNo ratings yet
- Guide to Fungal Skin Infections (DermatomycosisDocument128 pagesGuide to Fungal Skin Infections (DermatomycosisDevy KurniawatiNo ratings yet
- DERMATOPHYTOSES: LAB DIAGNOSIS AND CLASSIFICATIONDocument34 pagesDERMATOPHYTOSES: LAB DIAGNOSIS AND CLASSIFICATIONKana FajarNo ratings yet
- Tinea InfectionDocument3 pagesTinea InfectionlkokodkodNo ratings yet
- Antifungal Therapy for Fungal InfectionsDocument186 pagesAntifungal Therapy for Fungal InfectionsRizweta DestinNo ratings yet
- MCB 409 Pathogenic Mycology(1)Document49 pagesMCB 409 Pathogenic Mycology(1)ejohn8340No ratings yet
- Cutaneous Larva MigransDocument4 pagesCutaneous Larva MigransanissabilfaqihNo ratings yet
- DermatophytesDocument10 pagesDermatophytesRaunaNo ratings yet
- DermatomycosesDocument2 pagesDermatomycosesRay CullenNo ratings yet
- Guide to Dermatomycoses: Fungal Infections of the Skin, Hair and NailsDocument73 pagesGuide to Dermatomycoses: Fungal Infections of the Skin, Hair and NailssnylstlNo ratings yet
- Epidemiological Trends in Skin Mycoses Worldwide: Blanka Havlickova, Viktor A. Czaika and Markus FriedrichDocument14 pagesEpidemiological Trends in Skin Mycoses Worldwide: Blanka Havlickova, Viktor A. Czaika and Markus FriedrichRS Tk IV PekanbaruNo ratings yet
- DermatophytosisDocument5 pagesDermatophytosisRadovan Miki RadovanovicNo ratings yet
- Tinea Corporis, Tinea Cruris, Tinea Nigra, and Piedra: Dermatologic Clinics August 2003Document7 pagesTinea Corporis, Tinea Cruris, Tinea Nigra, and Piedra: Dermatologic Clinics August 2003Dicky KurniawanNo ratings yet
- Tinea Capitis Q & ADocument2 pagesTinea Capitis Q & Aandre yuindartantoNo ratings yet
- Tinea Capitis: Fungal Infection of the ScalpDocument16 pagesTinea Capitis: Fungal Infection of the ScalpIkram IkramNo ratings yet
- Mikosis Superfisial: Penyebab, Gejala, Diagnosis dan PengobatanDocument46 pagesMikosis Superfisial: Penyebab, Gejala, Diagnosis dan PengobatanAdipuraAtmadjaEgokNo ratings yet
- Dermatophyte Infections: Types, Causes, Symptoms and TreatmentDocument59 pagesDermatophyte Infections: Types, Causes, Symptoms and Treatmentحسين طاهر حاتم طاهرNo ratings yet
- Topical Treatment of Common Superficial Tinea InfectionsDocument8 pagesTopical Treatment of Common Superficial Tinea InfectionsColate LocoNo ratings yet
- Chemotherapy of Fungal DiseasesDocument51 pagesChemotherapy of Fungal DiseasesSalmaan KhanNo ratings yet
- 4 DermatomycosesDocument96 pages4 DermatomycosesShany SchwarzwaldNo ratings yet
- BAHAN Tinea CapitisDocument28 pagesBAHAN Tinea CapitisYorika HafelaniNo ratings yet
- Fungi & Systemic MycosesDocument42 pagesFungi & Systemic MycosesariffdrNo ratings yet
- Medical MycologyDocument14 pagesMedical Mycologyhawkar omerNo ratings yet
- Ringworm Infection in Dogs and Cats: In: Recent Advances in Canine Infectious Diseases, L. Carmichael (Ed.)Document7 pagesRingworm Infection in Dogs and Cats: In: Recent Advances in Canine Infectious Diseases, L. Carmichael (Ed.)Auni IbrahimNo ratings yet
- Lesson 2 Superficial Cutaneous Mycosis HandoutsDocument8 pagesLesson 2 Superficial Cutaneous Mycosis HandoutsKhay Mae DonascoNo ratings yet
- Fungal InfectionsDocument9 pagesFungal InfectionsCoral Srinivasa RamaluNo ratings yet
- Dermatology Resident NotesDocument37 pagesDermatology Resident Notesedgar mandengNo ratings yet
- Antifungal DrugsDocument16 pagesAntifungal DrugsAmrinder SagguNo ratings yet
- Mikosis Superfisialis Parasit UKRIDADocument76 pagesMikosis Superfisialis Parasit UKRIDASamdiSutantoNo ratings yet
- Dermatofitosis 2011 1Document35 pagesDermatofitosis 2011 1Carmen Cajina Doña MamiNo ratings yet
- Medically Important FungihandoutDocument55 pagesMedically Important FungihandoutHervis FantiniNo ratings yet
- Dermatofitosis: Penyakit Jamur Kulit yang Disebabkan DermatofitaDocument84 pagesDermatofitosis: Penyakit Jamur Kulit yang Disebabkan Dermatofitadesak 102018084No ratings yet
- DERMATOPHYTOSIS IN CATS ABCD Guidelines On Prevention and ManagementDocument8 pagesDERMATOPHYTOSIS IN CATS ABCD Guidelines On Prevention and Managementmariaisabelgomez26No ratings yet
- Hubungan Wilayah Kerja Terhadap Kejadian Jamur Pada Karyawan PT - Perkebunan Nusantara ViiDocument7 pagesHubungan Wilayah Kerja Terhadap Kejadian Jamur Pada Karyawan PT - Perkebunan Nusantara ViiLedya Esya HestariNo ratings yet
- Itchy Rash on Feet: Tinea PedisDocument9 pagesItchy Rash on Feet: Tinea PedisKevaughn HenryNo ratings yet
- Subcutaneous MycosesDocument3 pagesSubcutaneous MycosesiwennieNo ratings yet
- Classification of Fungal InfectionsDocument26 pagesClassification of Fungal Infectionstev26No ratings yet
- Tinea Corporis, Tinea Cruris, Tinea Nigra, and PiedraDocument6 pagesTinea Corporis, Tinea Cruris, Tinea Nigra, and PiedraIsni KhoirunisaNo ratings yet
- Fungal Diseases of the Skin: Types, Causes and TreatmentsDocument6 pagesFungal Diseases of the Skin: Types, Causes and TreatmentsputraimanullahNo ratings yet
- Superficial & Cutaneous MycosesDocument42 pagesSuperficial & Cutaneous Mycosesdawam986142No ratings yet
- Fungal Infections of the Skin and NailsDocument22 pagesFungal Infections of the Skin and NailsDragon Gie30No ratings yet
- Superficial and Cutaneous MycosesDocument10 pagesSuperficial and Cutaneous MycosesCIRILO MABBORANGNo ratings yet
- Humic Substances As Electron Acceptor For Microbial RespirationDocument4 pagesHumic Substances As Electron Acceptor For Microbial RespirationNed FlandersNo ratings yet
- Barbecue Sauce HomadeDocument22 pagesBarbecue Sauce HomadeLiza NasrNo ratings yet
- Drug study on TegretolDocument2 pagesDrug study on TegretolSophia Kaye AguinaldoNo ratings yet
- Moisture Sorption Isotherms Characteristics of Food ProductsDocument10 pagesMoisture Sorption Isotherms Characteristics of Food ProductsMustapha Bello50% (2)
- Practicum HandbookDocument12 pagesPracticum HandbookChikezie NwankworNo ratings yet
- SC upholds reclusion perpetua for statutory rape within the familyDocument9 pagesSC upholds reclusion perpetua for statutory rape within the familymrvirginesNo ratings yet
- Chapter 5 Integumentary Study GuideDocument3 pagesChapter 5 Integumentary Study GuideSuperjunior8No ratings yet
- The Secret of Eternal Youth PDFDocument36 pagesThe Secret of Eternal Youth PDFArunesh A Chand100% (4)
- With Reference To Relief, Drainage and Economic Importance, Explain The Differences Between The Northern Mountains and Western MountainsDocument3 pagesWith Reference To Relief, Drainage and Economic Importance, Explain The Differences Between The Northern Mountains and Western Mountainshajra chatthaNo ratings yet
- Traits and BehaviorDocument8 pagesTraits and BehaviorNorwafa Cariga EspinosaNo ratings yet
- Chapter 8-Mental Health and Well-Being in Middle and LateDocument15 pagesChapter 8-Mental Health and Well-Being in Middle and LateCathleen Beth100% (2)
- HN E-Catalog CableDocument36 pagesHN E-Catalog CableMin Min AungNo ratings yet
- 2requirements Permit PDFDocument1 page2requirements Permit PDFHazel CorralNo ratings yet
- Diseases That Cause HypoproteinemiaDocument12 pagesDiseases That Cause HypoproteinemiaRachel Marie M. GaniaNo ratings yet
- Jurnal Dermatitis AtopikDocument20 pagesJurnal Dermatitis AtopikchintyaNo ratings yet
- Arya Steels Ratings Remain StableDocument4 pagesArya Steels Ratings Remain StableData CentrumNo ratings yet
- Personal LetterDocument4 pagesPersonal LetterAskme AzmyNo ratings yet
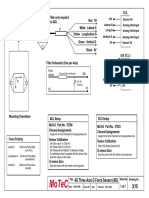
- Filter and wiring schematic for 3-axis ADL G-force sensorDocument1 pageFilter and wiring schematic for 3-axis ADL G-force sensorJuan Ramón Pérez LorenzoNo ratings yet
- Worlds Healthiest Super Food - SpirulinaDocument16 pagesWorlds Healthiest Super Food - SpirulinaBhadra BasumataryNo ratings yet
- Passenger Ship SubdivisionDocument6 pagesPassenger Ship SubdivisionPunit Pandey100% (2)
- Working Length Determination in RCTDocument38 pagesWorking Length Determination in RCTDidar Sadiq Kwekha100% (1)
- Section - A: Holiday Homework For Grade XiDocument7 pagesSection - A: Holiday Homework For Grade XiGM Ali KawsarNo ratings yet
- ZinkPower Batam - Company BrochureDocument6 pagesZinkPower Batam - Company BrochureansarALLAAHNo ratings yet
- Online Medicine Industry Competitor AnalysisDocument14 pagesOnline Medicine Industry Competitor Analysispawangadiya1210No ratings yet
- Sarah Fahy CV College PDFDocument4 pagesSarah Fahy CV College PDFapi-487352339No ratings yet
- Basic Principles of Growth DevelopmentDocument19 pagesBasic Principles of Growth DevelopmentMikz Chua100% (1)
- 20090716FoxReiki PDFDocument40 pages20090716FoxReiki PDFAgustina RomeroNo ratings yet
- Chapter 11 Post-Emulsified Fluorescent (Hydrophilic & Lipophilic)Document13 pagesChapter 11 Post-Emulsified Fluorescent (Hydrophilic & Lipophilic)maxpan maxNo ratings yet
- ASME B16.5 Flange Rating CalculatorDocument10 pagesASME B16.5 Flange Rating Calculatorfaizal100% (2)
- Structural Notes and Specifications for ConcreteDocument1 pageStructural Notes and Specifications for Concreteroger100% (2)
- Summary of Mary Claire Haver's The Galveston DietFrom EverandSummary of Mary Claire Haver's The Galveston DietRating: 5 out of 5 stars5/5 (1)
- Forever Strong: A New, Science-Based Strategy for Aging WellFrom EverandForever Strong: A New, Science-Based Strategy for Aging WellNo ratings yet
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookFrom EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookRating: 3.5 out of 5 stars3.5/5 (2)
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyFrom EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyRating: 5 out of 5 stars5/5 (1)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeFrom EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeNo ratings yet
- The Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonFrom EverandThe Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonRating: 3.5 out of 5 stars3.5/5 (33)
- The Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingFrom EverandThe Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingRating: 4 out of 5 stars4/5 (3)
- The Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyFrom EverandThe Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyNo ratings yet
- Secrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainFrom EverandSecrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainRating: 3.5 out of 5 stars3.5/5 (38)
- Body Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomFrom EverandBody Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomRating: 4 out of 5 stars4/5 (1)
- The Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodFrom EverandThe Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodNo ratings yet
- Sugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthFrom EverandSugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthRating: 4 out of 5 stars4/5 (6)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisFrom EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisRating: 3 out of 5 stars3/5 (2)
- Keto Friendly Recipes: Easy Keto For Busy PeopleFrom EverandKeto Friendly Recipes: Easy Keto For Busy PeopleRating: 3.5 out of 5 stars3.5/5 (2)
- Glucose Revolution: The Life-Changing Power of Balancing Your Blood SugarFrom EverandGlucose Revolution: The Life-Changing Power of Balancing Your Blood SugarRating: 5 out of 5 stars5/5 (350)
- The Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsFrom EverandThe Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsRating: 4 out of 5 stars4/5 (49)
- Allen Carr's Easy Way for Women to Lose Weight: The original Easyway methodFrom EverandAllen Carr's Easy Way for Women to Lose Weight: The original Easyway methodRating: 4.5 out of 5 stars4.5/5 (18)
- Happy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainFrom EverandHappy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainRating: 3.5 out of 5 stars3.5/5 (6)
- Grit & Grace: Train the Mind, Train the Body, Own Your LifeFrom EverandGrit & Grace: Train the Mind, Train the Body, Own Your LifeRating: 4 out of 5 stars4/5 (3)
- Find Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeFrom EverandFind Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeRating: 4 out of 5 stars4/5 (3)
- Rapid Weight Loss Hypnosis: Deep Sleep Your Way to Rapid Weight Loss, Healing Your Body and Self Esteem with Guided Meditations and Positive AffirmationsFrom EverandRapid Weight Loss Hypnosis: Deep Sleep Your Way to Rapid Weight Loss, Healing Your Body and Self Esteem with Guided Meditations and Positive AffirmationsRating: 5 out of 5 stars5/5 (7)
- The Whole Body Reset: Your Weight-Loss Plan for a Flat Belly, Optimum Health & a Body You'll Love at Midlife and BeyondFrom EverandThe Whole Body Reset: Your Weight-Loss Plan for a Flat Belly, Optimum Health & a Body You'll Love at Midlife and BeyondRating: 4.5 out of 5 stars4.5/5 (28)
- Glucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingFrom EverandGlucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingRating: 5 out of 5 stars5/5 (60)
- Rapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreFrom EverandRapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreRating: 5 out of 5 stars5/5 (17)
- Eat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouFrom EverandEat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouNo ratings yet
- How to Be Well: The 6 Keys to a Happy and Healthy LifeFrom EverandHow to Be Well: The 6 Keys to a Happy and Healthy LifeRating: 5 out of 5 stars5/5 (1)