You might also like
- IntffDocument2 pagesIntffLana AmerieNo ratings yet
- Viral Exanthems ReviewerDocument4 pagesViral Exanthems ReviewerNicole TorralbaNo ratings yet
- Module 6.4 ParasitesDocument6 pagesModule 6.4 ParasitesPNo ratings yet
- Tinywow Communicable-Diseases 48897647 12Document1 pageTinywow Communicable-Diseases 48897647 12JULIUS CEZAR QUINAYNo ratings yet
- Collection of Virology (Mansoura Dentistry)Document6 pagesCollection of Virology (Mansoura Dentistry)elsayed barhomeNo ratings yet
- Communicable Diseases 2.4-5.22Document9 pagesCommunicable Diseases 2.4-5.22Vhince PiscoNo ratings yet
- Female Genital TractDocument5 pagesFemale Genital Tractsarguss14100% (1)
- Microbiology PinkDocument3 pagesMicrobiology PinkBenjamin GaliaNo ratings yet
- 05.31.2 Pathology of The Female Reproductive System I FinalDocument80 pages05.31.2 Pathology of The Female Reproductive System I FinalCompucel IngenieriaNo ratings yet
- SubcutaneousDocument2 pagesSubcutaneousMary ChristelleNo ratings yet
- Arenavirus Bunyavirus FilovirusDocument5 pagesArenavirus Bunyavirus FilovirusRue VargasNo ratings yet
- Fungal InfectionDocument3 pagesFungal InfectionNicole TorralbaNo ratings yet
- Tinywow Communicable-Diseases 48897647 6Document1 pageTinywow Communicable-Diseases 48897647 6JULIUS CEZAR QUINAYNo ratings yet
- Integumentary Disoder: Nursing Care PlanDocument3 pagesIntegumentary Disoder: Nursing Care PlanFrancise Elyn OcubilloNo ratings yet
- Microbiology 19 PDFDocument6 pagesMicrobiology 19 PDFLyka Villagracia AsiloNo ratings yet
- Microbiology: Atypical Bacteria: Chlamydia, Mycoplasms, LegionellaDocument4 pagesMicrobiology: Atypical Bacteria: Chlamydia, Mycoplasms, LegionellaPatricia Mae de JesusNo ratings yet
- The Newborn at Risk of A Maternal Infection Opthalmia NeonatorumDocument2 pagesThe Newborn at Risk of A Maternal Infection Opthalmia NeonatorumIren Rose PañaNo ratings yet
- Microbiology: Parvovirus, Papillomavirus, and PolyomavirusDocument3 pagesMicrobiology: Parvovirus, Papillomavirus, and PolyomavirusJustin TayabanNo ratings yet
- Viral InfectionsDocument23 pagesViral InfectionsMiguel Cuevas DolotNo ratings yet
- DNA VIRUSES-handout PDFDocument11 pagesDNA VIRUSES-handout PDFROTHESSA MARY CARINGALNo ratings yet
- Bacteria Chart FINAL 3 2Document32 pagesBacteria Chart FINAL 3 2Йеша Маниш МираниNo ratings yet
- 6-wolde-VIRAL EXANTHEMS, Gaus Gangren & LeprosyDocument84 pages6-wolde-VIRAL EXANTHEMS, Gaus Gangren & LeprosykamaluNo ratings yet
- Common Exanthems PDFDocument4 pagesCommon Exanthems PDFKaren Ivy BacsainNo ratings yet
- Pharm205 Unit5Document6 pagesPharm205 Unit5Yssa CelzoNo ratings yet
- Prelim Myco Trans PPT BasedDocument98 pagesPrelim Myco Trans PPT BasedJohn Vincent TacalNo ratings yet
- Tables VirusesDocument9 pagesTables VirusesOmphile DansonNo ratings yet
- 2023 Surgery Trans14 TheSkinandSubcutaneousTissue-compressed-8-15Document8 pages2023 Surgery Trans14 TheSkinandSubcutaneousTissue-compressed-8-15Adrian CaballesNo ratings yet
- Herpesvirus: ClassificationDocument5 pagesHerpesvirus: Classificationحسين محمد مطرود كاظمNo ratings yet
- Suggested ResponsesDocument3 pagesSuggested ResponsesVrutika PatelNo ratings yet
- Most Common Complication: Sabay SilaDocument6 pagesMost Common Complication: Sabay SilaSheryl Layne Lao-SebrioNo ratings yet
- Tinywow Communicable-Diseases 48897647 18Document1 pageTinywow Communicable-Diseases 48897647 18JULIUS CEZAR QUINAYNo ratings yet
- 5 Systemic-MycosesDocument2 pages5 Systemic-MycosesMariz MartinezNo ratings yet
- Module 6.1 MicrobiologyDocument18 pagesModule 6.1 MicrobiologyPNo ratings yet
- Insignis Pedia MMRV LopezDocument7 pagesInsignis Pedia MMRV LopezChrisfernan MondragonNo ratings yet
- Del Rosario Ryan D. BSN 4C1-7 Mr. Daniel Mon Mamanao: Measles Pre-Eruptive StageDocument5 pagesDel Rosario Ryan D. BSN 4C1-7 Mr. Daniel Mon Mamanao: Measles Pre-Eruptive Stageryandelrosario9yahooNo ratings yet
- HIV, Varicella, Polio, and Hepes VirusDocument3 pagesHIV, Varicella, Polio, and Hepes VirusIrfan Adi SaputraNo ratings yet
- Savannah Whitington: Your Brain On DrugsDocument1 pageSavannah Whitington: Your Brain On DrugsMicroposterNo ratings yet
- Tinywow Communicable-Diseases 48897647 3Document1 pageTinywow Communicable-Diseases 48897647 3JULIUS CEZAR QUINAYNo ratings yet
- DiseaseDocument5 pagesDiseaseinzegi96No ratings yet
- MicrofinalDocument7 pagesMicrofinaljwanaNo ratings yet
- HepatitisDocument26 pagesHepatitiserynlacsa715No ratings yet
- Problem 3.01 Nervous System Study Guide 4Document3 pagesProblem 3.01 Nervous System Study Guide 4Monish NaiduNo ratings yet
- Micp Midterms ReviewerDocument7 pagesMicp Midterms ReviewerReichelle Anne QuibinNo ratings yet
- Gass DNA Viruses General Properties: NADocument10 pagesGass DNA Viruses General Properties: NAGianna SablanNo ratings yet
- Lesson 11 STIDocument6 pagesLesson 11 STIdaryl jan komowangNo ratings yet
- Bacte Lec 1Document11 pagesBacte Lec 12234382No ratings yet
- Block 4B 2023 Viral Exanthems Part 2Document29 pagesBlock 4B 2023 Viral Exanthems Part 2Sabelo VictorNo ratings yet
- Module 7 - Infectious DiseasesDocument28 pagesModule 7 - Infectious DiseasesTararith KaingNo ratings yet
- Entamoebae HistolyticaDocument4 pagesEntamoebae HistolyticaNashrah HusnaNo ratings yet
- Chlamydia and MycoplasmaDocument5 pagesChlamydia and MycoplasmaMico Jan GurionNo ratings yet
- PREFINALS HandoutsDocument82 pagesPREFINALS HandoutskrstnkyslNo ratings yet
- CNS InfectionDocument10 pagesCNS InfectionShunqing ZhangNo ratings yet
- Parasitology ReviewerDocument7 pagesParasitology ReviewerSandra Mhay RodilloNo ratings yet
- Herpes Simplex Virus: 2 SerotypesDocument18 pagesHerpes Simplex Virus: 2 Serotypespedia blue bookNo ratings yet
- Exercise12 PDFDocument17 pagesExercise12 PDFHayna RoseNo ratings yet
- Case Study of Black Death: Our Lady of Fatima UniversityDocument7 pagesCase Study of Black Death: Our Lady of Fatima UniversityJanna PimentelNo ratings yet
- Neuroscience Ii: Summary: Nationality (Will Tell You Incidence, For Example, AsiansDocument29 pagesNeuroscience Ii: Summary: Nationality (Will Tell You Incidence, For Example, AsiansAngelaTrinidad100% (2)
- HIVDocument5 pagesHIVsarguss14100% (1)
- Truelearn Stuff PDFDocument16 pagesTruelearn Stuff PDFLanaAmerieNo ratings yet
- SLE SketchyDocument2 pagesSLE SketchyLanaAmerieNo ratings yet
- Macules Macules and Papules Papules VesiclesDocument6 pagesMacules Macules and Papules Papules VesiclesLanaAmerieNo ratings yet
- Ah PDFDocument134 pagesAh PDFLanaAmerieNo ratings yet
- Table 1: Infective Endocarditis Non Infective Myocarditis Myocardidits PericarditisDocument3 pagesTable 1: Infective Endocarditis Non Infective Myocarditis Myocardidits PericarditisLanaAmerieNo ratings yet
- Congenital Anomalies of Kidney and Lowe Urinary TractDocument2 pagesCongenital Anomalies of Kidney and Lowe Urinary TractLanaAmerieNo ratings yet
- RNL DruDocument1 pageRNL DruLanaAmerieNo ratings yet
- Skin PDFDocument13 pagesSkin PDFLanaAmerieNo ratings yet
- Integumentary Lec 1: Overview of The Integument: A-Integumentary (Skin) SystemDocument6 pagesIntegumentary Lec 1: Overview of The Integument: A-Integumentary (Skin) SystemLanaAmerieNo ratings yet
- OPP - Lab - Counterstrain - Ribs, Anterior, PosteriorDocument1 pageOPP - Lab - Counterstrain - Ribs, Anterior, PosteriorLanaAmerieNo ratings yet
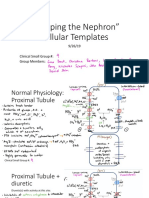
- "Mapping The Nephron" Cellular Templates: Gina Bartoni Lana Daniel ShinDocument11 pages"Mapping The Nephron" Cellular Templates: Gina Bartoni Lana Daniel ShinLanaAmerieNo ratings yet
- Urinery IncontinsetenceDocument1 pageUrinery IncontinsetenceLanaAmerieNo ratings yet
- Modelo de Evaluación Senior 6 AACIDocument5 pagesModelo de Evaluación Senior 6 AACINCNo ratings yet
- M Gen 000102Document15 pagesM Gen 000102miaNo ratings yet
- CCGL 9061 PosterDocument1 pageCCGL 9061 Posterchunpan tsangNo ratings yet
- MCI Sep, 10 QnsDocument27 pagesMCI Sep, 10 QnsdrmeenupNo ratings yet
- BMI Classification WhoDocument2 pagesBMI Classification WhoMuhammad AkrimNo ratings yet
- Europass CVDocument2 pagesEuropass CVKHALID SAMRATNo ratings yet
- Environmental Health Hazards: CPH Instructors Medical Laboratory Science Department San Pedro CollegeDocument56 pagesEnvironmental Health Hazards: CPH Instructors Medical Laboratory Science Department San Pedro CollegePatricia Nicole BaisNo ratings yet
- Tuberculous MeningitisDocument11 pagesTuberculous MeningitiszuhriNo ratings yet
- Central - Venous - Catheters Insertion Assisting 1073 PDFDocument6 pagesCentral - Venous - Catheters Insertion Assisting 1073 PDFMeejah HajeemNo ratings yet
- LiverultrasoundDocument62 pagesLiverultrasoundiuliia94No ratings yet
- Prophetic MedicineDocument6 pagesProphetic MedicineSiti Norakmal AkmaNo ratings yet
- Parasite Infestation Tungiasis (Parasitologi)Document17 pagesParasite Infestation Tungiasis (Parasitologi)Aditya NobelNo ratings yet
- A Case of Paediatric CholelithiasisDocument4 pagesA Case of Paediatric CholelithiasisHomoeopathic PulseNo ratings yet
- Actinomycetes: Click To Edit Master Subtitle StyleDocument37 pagesActinomycetes: Click To Edit Master Subtitle StyleHarsh Rajvanshi100% (1)
- Acute Articular RheumatismDocument3 pagesAcute Articular RheumatismcristinamihaNo ratings yet
- NALA Annual Report PDFDocument18 pagesNALA Annual Report PDFAnonymous nzFQfUAUNo ratings yet
- Portfolio Clinical Case Study 3 Lymphoma FinalDocument27 pagesPortfolio Clinical Case Study 3 Lymphoma Finalapi-277136509No ratings yet
- Hiluf: EthiopiaDocument17 pagesHiluf: EthiopiaNewborn2013No ratings yet
- Neurotrophic Keratopathy: BackgroundDocument2 pagesNeurotrophic Keratopathy: BackgroundkykyriskyNo ratings yet
- Common Eye Problems: NtroductionDocument14 pagesCommon Eye Problems: NtroductionFunky DestinationNo ratings yet
- ENGLISH 8 - 1st Quarter ExamDocument3 pagesENGLISH 8 - 1st Quarter ExamChrizzavilla VallejoNo ratings yet
- Haematology Physical AssessmentDocument26 pagesHaematology Physical AssessmentMarium Mohamed Ali100% (1)
- StomatitisDocument74 pagesStomatitisZahoor ZaidiNo ratings yet
- ASA Physical Status Classification System PDFDocument6 pagesASA Physical Status Classification System PDFfbihansipNo ratings yet
- Students' Reflections On "A Day in My Life During Covid-19 - United StatesDocument2 pagesStudents' Reflections On "A Day in My Life During Covid-19 - United StatespaleizenNo ratings yet
- Disease ProjectDocument2 pagesDisease Projectsacann100% (1)
- Varney - Wet Smear SlideDocument2 pagesVarney - Wet Smear SlideevillanuevaNo ratings yet
- Dengue Fever and Other Hemorrhagic Viruses (Deadly Diseases and Epidemics) - T. Chakraborty (Chelsea House, 2008) WW PDFDocument103 pagesDengue Fever and Other Hemorrhagic Viruses (Deadly Diseases and Epidemics) - T. Chakraborty (Chelsea House, 2008) WW PDFLavinia GeorgianaNo ratings yet
- 27 Questions For COVID and HIVDocument8 pages27 Questions For COVID and HIVterenlihNo ratings yet
- Icd 10Document11 pagesIcd 10Mitrasehat YkNo ratings yet