You might also like
- Dermatology Notes for Medical StudentsFrom EverandDermatology Notes for Medical StudentsRating: 4 out of 5 stars4/5 (5)
- Chest PainDocument24 pagesChest PainfatiniNo ratings yet
- Clinical Medicine Cheat Sheet Ebook PDFDocument18 pagesClinical Medicine Cheat Sheet Ebook PDFMokaNo ratings yet
- Handbook of Inpatient CardiologyFrom EverandHandbook of Inpatient CardiologyBryan J. WellsNo ratings yet
- Clinical MedicineDocument18 pagesClinical MedicineRishikesh AsthanaNo ratings yet
- DR Ali Qazaz HandoutsDocument103 pagesDR Ali Qazaz Handoutsf6bk6xnppyNo ratings yet
- Echocardiography For Systemic DiseaseDocument81 pagesEchocardiography For Systemic DiseaseSofia KusumadewiNo ratings yet
- CARDIAC TUMORS TransDocument12 pagesCARDIAC TUMORS TransjeccomNo ratings yet
- Mitral Valve ProlapseDocument2 pagesMitral Valve ProlapseAyumi StarNo ratings yet
- Atherosclerosis What and How?: Faris Basalamah, MD, FIHADocument24 pagesAtherosclerosis What and How?: Faris Basalamah, MD, FIHAfikriNo ratings yet
- Post-Strep Infxn Ddressler's Sydrome: Endocarditis Valvular Dse Pericarditis Cardiac TamponadeDocument5 pagesPost-Strep Infxn Ddressler's Sydrome: Endocarditis Valvular Dse Pericarditis Cardiac TamponadeEben Ezar Dela CruzNo ratings yet
- Medicine Cheat SheetsDocument16 pagesMedicine Cheat SheetsRisa Muthmainah100% (1)
- Lung CaDocument1 pageLung CaAqila MumtazNo ratings yet
- AAD BF Familial Cancer SyndromesDocument2 pagesAAD BF Familial Cancer Syndromeskahkashanahmed065No ratings yet
- Facts/Problems Hypotheses Need To Know Li'S: FFFFFFFFFFFFFFFFDocument3 pagesFacts/Problems Hypotheses Need To Know Li'S: FFFFFFFFFFFFFFFFDarrah KFNo ratings yet
- CARDIAC TUMORS Approach To ManagementDocument12 pagesCARDIAC TUMORS Approach To ManagementAnkit GulatiNo ratings yet
- Pericardial Diseases - Dr. BartolomeDocument8 pagesPericardial Diseases - Dr. BartolomeMedisina101No ratings yet
- Materi - Gagal Jantung NeonatusDocument36 pagesMateri - Gagal Jantung NeonatusPutra AchmadNo ratings yet
- CVS Short Cases: Yapa Wijeratne M/07/189Document2 pagesCVS Short Cases: Yapa Wijeratne M/07/189Li FaungNo ratings yet
- Cardio BootcampDocument9 pagesCardio BootcampMariam ShenoudaNo ratings yet
- Linician Pdate: Catheter Ablation of Ventricular TachycardiaDocument6 pagesLinician Pdate: Catheter Ablation of Ventricular TachycardiaSonia Rahma ANo ratings yet
- Blank MapDocument1 pageBlank Mapمحمد اياد حسن جاسمNo ratings yet
- Renal TumorsDocument1 pageRenal TumorsMohammad Moufaq El-BashabshehNo ratings yet
- Disturbances in CirculationDocument12 pagesDisturbances in CirculationJoei OcampoNo ratings yet
- Coronary Artery Diseases FullDocument3 pagesCoronary Artery Diseases FullGlare RhayneNo ratings yet
- Sickle Cell AnemiaDocument2 pagesSickle Cell AnemiaDonjeta AbaziNo ratings yet
- Week 2Document16 pagesWeek 2Lanz Andrei MatociñosNo ratings yet
- Infectious Diseases of The HeartDocument2 pagesInfectious Diseases of The HeartJulia Rae Delos SantosNo ratings yet
- Congenital Heart DefectsDocument7 pagesCongenital Heart DefectsJulia Rae Delos SantosNo ratings yet
- NCM 118 - Rle: College of Nursing 1 Semester AY 2021-2022Document4 pagesNCM 118 - Rle: College of Nursing 1 Semester AY 2021-2022cammel ramosNo ratings yet
- IM - Cardiomyopathy and MyocarditisDocument9 pagesIM - Cardiomyopathy and MyocarditisElisha BernabeNo ratings yet
- Acquired Heart ConditionsDocument9 pagesAcquired Heart ConditionsMaikka IlaganNo ratings yet
- Pa Tho Physiology of Spinal Cord InjuryDocument1 pagePa Tho Physiology of Spinal Cord InjuryGenel Joseph Jacildo Peñaflor100% (2)
- Tables NurologyDocument5 pagesTables NurologyRazan AlayedNo ratings yet
- Acute Biologic Crisis Quizlet 1Document4 pagesAcute Biologic Crisis Quizlet 1krissereiNo ratings yet
- MC Tumor MC Ca MC 1° Ca BrainDocument12 pagesMC Tumor MC Ca MC 1° Ca BrainRyan TurnerNo ratings yet
- Myocardial Concept MappingDocument34 pagesMyocardial Concept MappingTHIRD YEARNo ratings yet
- (02.19) SU Tumors of The Heart (TG3) - Final - Jan Matthew TolentinoDocument5 pages(02.19) SU Tumors of The Heart (TG3) - Final - Jan Matthew TolentinoMikmik DGNo ratings yet
- Aortic DissectionDocument2 pagesAortic DissectionTiffney NesakumarNo ratings yet
- IM Part 1 and 2 CombinedDocument100 pagesIM Part 1 and 2 CombinedsasghfdgNo ratings yet
- IM Part 1Document48 pagesIM Part 1sasghfdgNo ratings yet
- Oncologic EmergenciesDocument4 pagesOncologic EmergenciesJoharaNo ratings yet
- Week9-10 VistalDocument6 pagesWeek9-10 VistalKier Elizalde VistalNo ratings yet
- Week 11 - Cardiac Microbes, Tumors, Heart FailureDocument20 pagesWeek 11 - Cardiac Microbes, Tumors, Heart Failureshivani patelNo ratings yet
- Peripheral Vascular Medicine - Dr. Deduyo PDFDocument14 pagesPeripheral Vascular Medicine - Dr. Deduyo PDFMedisina101No ratings yet
- No L/R Ventricular HypertrophyDocument2 pagesNo L/R Ventricular HypertrophymcwnotesNo ratings yet
- Rapid Fire QuestionsDocument5 pagesRapid Fire QuestionsJovanNo ratings yet
- Cardio My Opa Thies ChartDocument2 pagesCardio My Opa Thies ChartSolomon Seth SallforsNo ratings yet
- Pathophysiology of Myocardial Infarction (STEMI)Document2 pagesPathophysiology of Myocardial Infarction (STEMI)michaela100% (3)
- Pheochromocytoma: PHEO - Dark CHROMO - Color CYT - Cell OMA - TumorDocument3 pagesPheochromocytoma: PHEO - Dark CHROMO - Color CYT - Cell OMA - TumorBiya MacunteNo ratings yet
- Disease/syndrome Inciting Incident Structures Affected PoliomyelitisDocument12 pagesDisease/syndrome Inciting Incident Structures Affected PoliomyelitismrhemmatNo ratings yet
- Red Vascular: Polygonal Cells Growing in Nests or Cords Lamellae of Dense CollagenDocument3 pagesRed Vascular: Polygonal Cells Growing in Nests or Cords Lamellae of Dense CollagenMaryam FadahNo ratings yet
- Pathophysiology of Congestive Heart FailureDocument2 pagesPathophysiology of Congestive Heart FailureAnonymous XvwKtnSrMR100% (10)
- Heart - PathophysiologyDocument60 pagesHeart - Pathophysiologyjmosser100% (3)
- Ajith Kumar P MPT Cardiopulmonary SciencesDocument30 pagesAjith Kumar P MPT Cardiopulmonary SciencesSuhana JahangeerNo ratings yet
- Types of TumorDocument16 pagesTypes of TumorCXT EnterpriseNo ratings yet
- Coronary Artery Disease: Dr. Sadewantoro, SP - JP, FIHA Fakultas Kedokteran Universitas Hang TuahDocument76 pagesCoronary Artery Disease: Dr. Sadewantoro, SP - JP, FIHA Fakultas Kedokteran Universitas Hang TuahDesti Ratna PutriNo ratings yet
- BKO BOOK CHAPTER CH 33 Approach To A Patient With HemiparesisDocument8 pagesBKO BOOK CHAPTER CH 33 Approach To A Patient With HemiparesisBal Krishna OjhaNo ratings yet
- Pathophysiology of Congestive Heart FailureDocument3 pagesPathophysiology of Congestive Heart FailureMel Izhra N. MargateNo ratings yet
- SLE SketchyDocument2 pagesSLE SketchyLanaAmerieNo ratings yet
- Ah PDFDocument134 pagesAh PDFLanaAmerieNo ratings yet
- Truelearn Stuff PDFDocument16 pagesTruelearn Stuff PDFLanaAmerieNo ratings yet
- Congenital Anomalies of Kidney and Lowe Urinary TractDocument2 pagesCongenital Anomalies of Kidney and Lowe Urinary TractLanaAmerieNo ratings yet
- Cluster of Lesions, PapularDocument3 pagesCluster of Lesions, PapularLanaAmerieNo ratings yet
- RNL DruDocument1 pageRNL DruLanaAmerieNo ratings yet
- Macules Macules and Papules Papules VesiclesDocument6 pagesMacules Macules and Papules Papules VesiclesLanaAmerieNo ratings yet
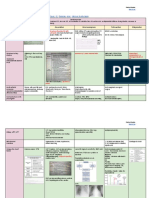
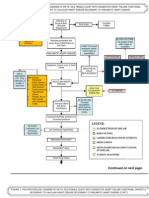
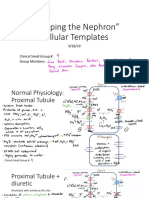
- "Mapping The Nephron" Cellular Templates: Gina Bartoni Lana Daniel ShinDocument11 pages"Mapping The Nephron" Cellular Templates: Gina Bartoni Lana Daniel ShinLanaAmerieNo ratings yet
- Integumentary Lec 1: Overview of The Integument: A-Integumentary (Skin) SystemDocument6 pagesIntegumentary Lec 1: Overview of The Integument: A-Integumentary (Skin) SystemLanaAmerieNo ratings yet
- Skin PDFDocument13 pagesSkin PDFLanaAmerieNo ratings yet
- OPP - Lab - Counterstrain - Ribs, Anterior, PosteriorDocument1 pageOPP - Lab - Counterstrain - Ribs, Anterior, PosteriorLanaAmerieNo ratings yet
- Urinery IncontinsetenceDocument1 pageUrinery IncontinsetenceLanaAmerieNo ratings yet
- Bowel Obstruction SurgeryDocument12 pagesBowel Obstruction SurgeryDivya JoyNo ratings yet
- CANINE-Medical Management of Chronic Otitis in DogsDocument11 pagesCANINE-Medical Management of Chronic Otitis in Dogstaner_soysuren100% (1)
- An Assessment of The Breastfeeding Practices and Knowledge Among Mothers in Barangay Camp One, Maramag, BukidnonDocument35 pagesAn Assessment of The Breastfeeding Practices and Knowledge Among Mothers in Barangay Camp One, Maramag, BukidnonKristine Baldoman CoquillaNo ratings yet
- Lesson 12 - Overview of The Wastewater Treatment ProcessDocument6 pagesLesson 12 - Overview of The Wastewater Treatment ProcessZar ChiNo ratings yet
- How To Cope With TransitionDocument4 pagesHow To Cope With Transitionmedia K2No ratings yet
- How To Have Good DreamsDocument12 pagesHow To Have Good DreamsZjuhaida IdaNo ratings yet
- Scaling Teeth TechniquesDocument12 pagesScaling Teeth TechniqueshanyNo ratings yet
- Studiu Spital Vanderbilt Study Article Winter 2013 PDFDocument2 pagesStudiu Spital Vanderbilt Study Article Winter 2013 PDFFlorinAndreiRomanNo ratings yet
- Medical Terminology A Programmed Approach 2nd Edition Bostwick Solutions Manual DownloadDocument7 pagesMedical Terminology A Programmed Approach 2nd Edition Bostwick Solutions Manual DownloadJason Appell100% (20)
- Dentoalveolar & ImplantsDocument10 pagesDentoalveolar & ImplantsabdullahNo ratings yet
- Vitamin EDocument11 pagesVitamin EErvan Apsara BismakaNo ratings yet
- Osteoporosis and Fragility Fractures Surgical PerpspectiveDocument54 pagesOsteoporosis and Fragility Fractures Surgical PerpspectiveSonal DudaniNo ratings yet
- Running Head: Client Teaching Wound Care 1Document3 pagesRunning Head: Client Teaching Wound Care 1Jerome Lazaro LumanogNo ratings yet
- Therapy - Case Study 2Document7 pagesTherapy - Case Study 2api-239581082100% (1)
- The Autism Spectrum Information Booklet: A Guide For Victorian FamiliesDocument24 pagesThe Autism Spectrum Information Booklet: A Guide For Victorian FamiliesAdriana KincsesNo ratings yet
- Ketoconazole PDFDocument7 pagesKetoconazole PDFparand2003No ratings yet
- ECOLOGIC MODEL - CholedocholithiasisDocument4 pagesECOLOGIC MODEL - CholedocholithiasisKristel PunoNo ratings yet
- Sewage Treatment PlantDocument12 pagesSewage Treatment Plantanuj dhavanNo ratings yet
- Facial Wound Assessment KitDocument9 pagesFacial Wound Assessment KitIJAR JOURNALNo ratings yet
- BPD Concept MapDocument3 pagesBPD Concept Mapsammillepointer86No ratings yet
- The Debut Olympia DietDocument13 pagesThe Debut Olympia DietFrank Black90% (10)
- Levels of EvidenceDocument4 pagesLevels of EvidenceshineeicaNo ratings yet
- Narayana Hrudalaya - Section D Group 7Document4 pagesNarayana Hrudalaya - Section D Group 7Prateek100% (1)
- Revised Sample Scheme of Work and Lesson Plan For Nursing Class (Koya)Document6 pagesRevised Sample Scheme of Work and Lesson Plan For Nursing Class (Koya)NATHANIEL YERINo ratings yet
- Study: Observational Travelers' DiarrheaDocument5 pagesStudy: Observational Travelers' DiarrheaFathah MuhammadNo ratings yet
- Brexpiprazole - Chem RevDocument112 pagesBrexpiprazole - Chem RevSam SonNo ratings yet
- CT PNSDocument22 pagesCT PNSHany85No ratings yet
- 1955 Ball LauraDocument55 pages1955 Ball LauraBene BeanNo ratings yet
- HSS 1101 - FINAL NotesDocument40 pagesHSS 1101 - FINAL NotesDARCY HAYDENNo ratings yet
- JAK Neural PlasticityDocument15 pagesJAK Neural PlasticityOwais KhanNo ratings yet