You might also like
- Getting Pregnant Faster: Step-By-Step Guide To Achieving PregnancyFrom EverandGetting Pregnant Faster: Step-By-Step Guide To Achieving PregnancyNo ratings yet
- Angrej Sir Obstetrics NotesssDocument119 pagesAngrej Sir Obstetrics Notessslakhwinder batthNo ratings yet
- Adaptasi Fisiologis KehamilanDocument57 pagesAdaptasi Fisiologis KehamilannafisaaNo ratings yet
- Pregnancy Signs GuideDocument8 pagesPregnancy Signs GuideMiguel LigasNo ratings yet
- Ghen ReviewDocument6 pagesGhen ReviewGenesis Marie Felices GonzalesNo ratings yet
- AntepartumDocument32 pagesAntepartumphoenix180100% (1)
- Ob Exam Study Guide The Bible 001 49pgsDocument50 pagesOb Exam Study Guide The Bible 001 49pgsVin Lorenzo CampbellNo ratings yet
- Pregnancy Confirmation and ChangesDocument37 pagesPregnancy Confirmation and Changesana aurea aquino de leonNo ratings yet
- Pre Natal CareDocument3 pagesPre Natal CareRoseanne SaraNo ratings yet
- Physical and Physiological Changes in PregnancyDocument35 pagesPhysical and Physiological Changes in PregnancyAYO NELSONNo ratings yet
- Maternity Nursing Review: Ahmed El KahloutDocument60 pagesMaternity Nursing Review: Ahmed El KahloutHabebt MusabNo ratings yet
- Lecturio 3041Document17 pagesLecturio 3041Pranjali WeladiNo ratings yet
- Pregnancy Anatomy PhysiologyDocument54 pagesPregnancy Anatomy PhysiologySam CiriacoNo ratings yet
- Post Partal Care 7Document36 pagesPost Partal Care 7Christian OpinaldoNo ratings yet
- HX and PX Obstetrics and GynecologyDocument21 pagesHX and PX Obstetrics and GynecologyTadesse MuhammedNo ratings yet
- DX of PregnancyDocument41 pagesDX of Pregnancyshivamg.sg1234No ratings yet
- 208-230 CH08 Lowdermilk - QXDDocument23 pages208-230 CH08 Lowdermilk - QXDSyarifah Ro'fahNo ratings yet
- Pregnancy Diagnosis: Peng Xuebing, M.D. Dept of Obs/Gyn Beijing Fu Xing Hospital Capital Medical UniversityDocument48 pagesPregnancy Diagnosis: Peng Xuebing, M.D. Dept of Obs/Gyn Beijing Fu Xing Hospital Capital Medical UniversityAhmed TarigNo ratings yet
- Perub Fisik Saat KehamilanDocument66 pagesPerub Fisik Saat KehamilanrismaNo ratings yet
- Positive Pregnancy Test-Presence of HCG in The 5. BallottmentDocument8 pagesPositive Pregnancy Test-Presence of HCG in The 5. BallottmentVince Matt BaguioNo ratings yet
- PuerperiumDocument85 pagesPuerperiumHema MaliniNo ratings yet
- ANTENATAL CARE Translate GooglingDocument26 pagesANTENATAL CARE Translate GooglingLutfi ari206100% (2)
- ACFrOgBadmrbzR Zbaf9LIsgA4xz3BXrf4T JrmRyxu5 5bkJFOaK1lMBnJ2 AUVEbPfI17GyIzBlEKvmA QY2 MBlLC8PHYkavITBEfKLN2rz Ns UV ETHtZJ3GVrlvuohWjtap7LzQ0YgxbfDocument37 pagesACFrOgBadmrbzR Zbaf9LIsgA4xz3BXrf4T JrmRyxu5 5bkJFOaK1lMBnJ2 AUVEbPfI17GyIzBlEKvmA QY2 MBlLC8PHYkavITBEfKLN2rz Ns UV ETHtZJ3GVrlvuohWjtap7LzQ0YgxbfBiraito TakanaNo ratings yet
- Changes During PregnancyDocument25 pagesChanges During PregnancyArambam ArunaNo ratings yet
- Signs of PregnancyDocument53 pagesSigns of PregnancyFrancr ToledanoNo ratings yet
- I. Skenario B Blok 17Document37 pagesI. Skenario B Blok 17Kadek MarthaNo ratings yet
- Maternity Client Antepartum Care ReviewDocument64 pagesMaternity Client Antepartum Care ReviewJaypee Fabros EdraNo ratings yet
- Diagnosis of PregnancyDocument48 pagesDiagnosis of PregnancyMukesh ThakurNo ratings yet
- Basic OB-GYN Terminology ExplainedDocument67 pagesBasic OB-GYN Terminology ExplainedCricket Highlights Full HD100% (1)
- Maternal and Child SemifinalsDocument31 pagesMaternal and Child SemifinalsKarl Symon AmperNo ratings yet
- Diagnosis of PregnancyDocument63 pagesDiagnosis of Pregnancyindri febiyanNo ratings yet
- Fetal CirculationDocument36 pagesFetal CirculationShfici AdanNo ratings yet
- Physiologic Changes in PregnancyDocument53 pagesPhysiologic Changes in PregnancyDorothy Jane OrdinarioNo ratings yet
- Maternity 2-1-1Document81 pagesMaternity 2-1-1kidisttaye578No ratings yet
- Pregnancy Diagnosis GuideDocument19 pagesPregnancy Diagnosis Guidemail4grlslkNo ratings yet
- Postpartum Changes and CareDocument34 pagesPostpartum Changes and Careanon_55864979No ratings yet
- PregnancyDocument26 pagesPregnancyarambam arunaNo ratings yet
- DIAGNOSIS of PREGNANCYDocument2 pagesDIAGNOSIS of PREGNANCYZarlyn MirafloresNo ratings yet
- Diagnosisofpregnancy 150127223055 Conversion Gate01Document40 pagesDiagnosisofpregnancy 150127223055 Conversion Gate01madhu.BNo ratings yet
- Ug Class 1Document38 pagesUg Class 1Saloni SaloniNo ratings yet
- Curs Stoma EnglezaDocument19 pagesCurs Stoma Englezamail4grlslkNo ratings yet
- Assessment of the Pregnant WomanDocument8 pagesAssessment of the Pregnant WomanVince Matt BaguioNo ratings yet
- 14 USI-Diagnosis of PregnancyDocument19 pages14 USI-Diagnosis of PregnancyEugene LancasterNo ratings yet
- Post Partum Nursing NotesDocument35 pagesPost Partum Nursing NotesyolondanicNo ratings yet
- OB Final Exam Study GuideDocument14 pagesOB Final Exam Study GuideMarissa SolanoNo ratings yet
- New NORMAL PUERPERIUMDocument21 pagesNew NORMAL PUERPERIUMvarshaNo ratings yet
- Diagnosis of PregnancyDocument53 pagesDiagnosis of PregnancyAdrija MukherjeeNo ratings yet
- Psychological and Physiological Changes of PregnancyDocument42 pagesPsychological and Physiological Changes of PregnancyAustine James Sabenicio PantiloNo ratings yet
- Signs and Symptoms of Pregnancy: Presumptive, Probable and Positive SignsDocument15 pagesSigns and Symptoms of Pregnancy: Presumptive, Probable and Positive SignsCRISTINE DELNo ratings yet
- Psychological and Physiological Changes of PregnancyDocument19 pagesPsychological and Physiological Changes of PregnancyRilly Yane PutryNo ratings yet
- Semifinals - NCM 107Document67 pagesSemifinals - NCM 107conahs nasugbuNo ratings yet
- 15 Signs Stages of LaborDocument84 pages15 Signs Stages of LaborDorothy Jane OrdinarioNo ratings yet
- Maternity Nursing Review: Marwa KHDocument27 pagesMaternity Nursing Review: Marwa KHHasan A AsFourNo ratings yet
- Diagnosis of Pregnancy - Signs, Differential DiagnosisDocument39 pagesDiagnosis of Pregnancy - Signs, Differential DiagnosisKripa SusanNo ratings yet
- Postpartum Psychotic DisordesDocument71 pagesPostpartum Psychotic DisordesramandeepNo ratings yet
- Maternity NursingDocument162 pagesMaternity Nursingniogan anthonyNo ratings yet
- Prenatal MGTDocument16 pagesPrenatal MGTClairie Jhane ClaorNo ratings yet
- Physiologic Changes of PregnancyDocument7 pagesPhysiologic Changes of PregnancyReyna Mee AhiyasNo ratings yet
- Week 3 Care of The Woman Experiencing A Sudden Pregnancy ComplicationsDocument68 pagesWeek 3 Care of The Woman Experiencing A Sudden Pregnancy ComplicationsWendell Mark B FernandezNo ratings yet
- 5 Normal PeurpuriumDocument48 pages5 Normal Peurpuriumdemeke andebetNo ratings yet
- Secretary's Certificate To Open and Close An Account FIVE TRAVELLERSDocument3 pagesSecretary's Certificate To Open and Close An Account FIVE TRAVELLERSmaria reyesNo ratings yet
- AntepartumDocument46 pagesAntepartummaria reyesNo ratings yet
- AntepartumDocument13 pagesAntepartummaria reyesNo ratings yet
- Ae Iv-JannahDocument5 pagesAe Iv-Jannahmaria reyesNo ratings yet
- Antepartum & Postpartum CareDocument3 pagesAntepartum & Postpartum Caremaria reyesNo ratings yet
- ReviewerDocument3 pagesReviewermaria reyesNo ratings yet
- 1Document1 page1maria reyesNo ratings yet
- Pantheon-Katalog Eng WebDocument16 pagesPantheon-Katalog Eng WebJoe DoeNo ratings yet
- Management Foreign BodyDocument6 pagesManagement Foreign BodyRahmatia SyukrinaNo ratings yet
- VSD Power Supply Connections and EarthingDocument4 pagesVSD Power Supply Connections and EarthingHumaid ShaikhNo ratings yet
- Columbus Files Motion To Dismiss Bankruptcy Claim by Latitude Five25 OwnersDocument38 pagesColumbus Files Motion To Dismiss Bankruptcy Claim by Latitude Five25 OwnersWSYX/WTTENo ratings yet
- CaseStudy AmtrakDocument14 pagesCaseStudy Amtraksnob_kNo ratings yet
- Recycle ProgramDocument2 pagesRecycle ProgramKaps BlazeNo ratings yet
- Communications in Algebra: On The U-Invariant of P-Adic Function FieldsDocument9 pagesCommunications in Algebra: On The U-Invariant of P-Adic Function FieldsKarim ZahidiNo ratings yet
- yudaturana,+Manajer+Jurnal,+dr +nelson+rev+2+ (162-172)Document12 pagesyudaturana,+Manajer+Jurnal,+dr +nelson+rev+2+ (162-172)Fath TiaraNo ratings yet
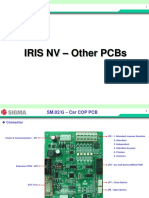
- 07 IRIS NV PCB OtherDocument15 pages07 IRIS NV PCB OtherArnaldo cordovaNo ratings yet
- Hydraulic Excavator RH 200 1,568 kW 30.5 m3Document8 pagesHydraulic Excavator RH 200 1,568 kW 30.5 m3mchan1965100% (1)
- EniSpA - The Corporate Strategy of An International Energy Major PDFDocument24 pagesEniSpA - The Corporate Strategy of An International Energy Major PDFAnonymous 9ZMbuR75% (4)
- Mañanita Songs Mañanita SongsDocument2 pagesMañanita Songs Mañanita SongsSanchez Bayan100% (1)
- Free Printable House Cleaning Schedule Template PDFDocument1 pageFree Printable House Cleaning Schedule Template PDFclear100% (1)
- Effect of Pregnancy Induced Hypertension on Mothers and Babies Hematological ProfilesDocument3 pagesEffect of Pregnancy Induced Hypertension on Mothers and Babies Hematological ProfilesAbdifatah AhmedNo ratings yet
- Fault Codes: STO U AndriivDocument3 pagesFault Codes: STO U AndriivAtochkavNo ratings yet
- Musical Siren Project Report Under 40 CharactersDocument10 pagesMusical Siren Project Report Under 40 Charactersvinod kapateNo ratings yet
- Lista Arancelaria EUADocument547 pagesLista Arancelaria EUAvilisbeth18No ratings yet
- Collaboration Processes: Looking Inside the Black BoxDocument13 pagesCollaboration Processes: Looking Inside the Black Boxเข้าใจว่า น่าจะชื่อตุ้นNo ratings yet
- Image Forgery DetectionDocument17 pagesImage Forgery DetectionanlemacoNo ratings yet
- Sliding, Overturning, Bearing Pressure and Bending Reinforcement Calculations for Retaining WallDocument4 pagesSliding, Overturning, Bearing Pressure and Bending Reinforcement Calculations for Retaining WallAbdul Aziz Julkarnain ZulkifliNo ratings yet
- Wily Walnut BRAIN SQUEEZERS Vol.1Document116 pagesWily Walnut BRAIN SQUEEZERS Vol.1tarzaman88% (8)
- List of Students Allotted in Open Elective Subjects (B. Tech and M. Tech (Dual Degree) Integrated MSc. - 4th Semester - Regular - 2018 - 19) - 2 PDFDocument26 pagesList of Students Allotted in Open Elective Subjects (B. Tech and M. Tech (Dual Degree) Integrated MSc. - 4th Semester - Regular - 2018 - 19) - 2 PDFArpan JaiswalNo ratings yet
- Unit 4 Early HumansDocument8 pagesUnit 4 Early HumansSepfira ReztikaNo ratings yet
- Fit For WashingDocument85 pagesFit For WashingIyaka YoeNo ratings yet
- Bosch EBike Product Catalogue MY2021 enDocument92 pagesBosch EBike Product Catalogue MY2021 enIvanNo ratings yet
- Jigoku Shoujo Eikyuu No SonzaiDocument166 pagesJigoku Shoujo Eikyuu No Sonzaiapi-224188021No ratings yet
- EU Food Label GuidanceDocument99 pagesEU Food Label GuidanceMunteanu CristianNo ratings yet
- Kapla ResumeDocument35 pagesKapla ResumeAbinashNo ratings yet
- Binzel - Katalog MAGDocument64 pagesBinzel - Katalog MAGAdrian KustraNo ratings yet
- The Future - G&VDocument6 pagesThe Future - G&VManuelHerreraMontoyaNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)