You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- MedicalBooks PDFDocument80 pagesMedicalBooks PDFfgdhgfrh50% (8)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Gourmet FinalDocument33 pagesGourmet Finalrizwanhafsa50% (4)
- Cell Damage and DeathDocument1 pageCell Damage and DeathfgdhgfrhNo ratings yet
- Glasgow Coma ScaleDocument4 pagesGlasgow Coma ScalefgdhgfrhNo ratings yet
- Embryology 10Document5 pagesEmbryology 10fgdhgfrhNo ratings yet
- The Probe Level Monitor: Instruction Manual PL-517 January 2001Document20 pagesThe Probe Level Monitor: Instruction Manual PL-517 January 2001horacio mondragon100% (1)
- GHVGHDocument3 pagesGHVGHINDAH IKA SARININGRUMNo ratings yet
- Before Domination: The History of Jollibee in The PhilippinesDocument22 pagesBefore Domination: The History of Jollibee in The PhilippinesChestineErikhaUmagatNo ratings yet
- Detector arc-LAD - HS 2019Document11 pagesDetector arc-LAD - HS 2019kryo195No ratings yet
- AlmeidaDocument8 pagesAlmeidaNicole TristanchoNo ratings yet
- Supplier Evalution & Control ProcedureDocument4 pagesSupplier Evalution & Control ProcedurePrime Cap100% (1)
- Code - 2216 - Congenital EventrationDocument5 pagesCode - 2216 - Congenital EventrationHumaida Hasan SamiraNo ratings yet
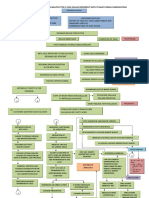
- Pathophysiology of Diabetes Mellitus Type Ii With ComplicationsDocument4 pagesPathophysiology of Diabetes Mellitus Type Ii With ComplicationsEricka Genove100% (1)
- Developmental Stages of Middle and Late AdolescenceDocument17 pagesDevelopmental Stages of Middle and Late AdolescenceFRED100% (1)
- Oncology McqsDocument115 pagesOncology McqsSyed NoorNo ratings yet
- Solid Recovered Fuels - Specifications andDocument8 pagesSolid Recovered Fuels - Specifications andLaraCarralNo ratings yet
- Aerial View of CII-Godrej GBC, Hyderabad Showing Wind Towers, Solar Photovoltaic Panels and Green Roofs. (Sourced)Document11 pagesAerial View of CII-Godrej GBC, Hyderabad Showing Wind Towers, Solar Photovoltaic Panels and Green Roofs. (Sourced)Happie SinghNo ratings yet
- Alpha Series Workshop Manual: Lpa, LPW, LPWT, Lpws and LPWGDocument109 pagesAlpha Series Workshop Manual: Lpa, LPW, LPWT, Lpws and LPWGAndres Huertas100% (1)
- Pat Bahasa Inggris Kelas IiDocument3 pagesPat Bahasa Inggris Kelas Iiwiwik widajatiNo ratings yet
- TSB SolventDocument9 pagesTSB SolventMaythee SaisriyootNo ratings yet
- Concept of Prana Vayu & Shat Chakras in Marma Chikitsa (मममम मममममममम)Document4 pagesConcept of Prana Vayu & Shat Chakras in Marma Chikitsa (मममम मममममममम)VestigeKamleshNo ratings yet
- PDS Benefit Overview - Dentist 2019Document4 pagesPDS Benefit Overview - Dentist 2019jentotheskyNo ratings yet
- When God Himself Was A StudentDocument2 pagesWhen God Himself Was A StudentSagar SharmaNo ratings yet
- Jds Journal of Syiah Kuala Dentistry SocietyDocument5 pagesJds Journal of Syiah Kuala Dentistry SocietyDewa Ayu Kumara DewiNo ratings yet
- Form No. 16: Details of Salary Paid and Any Other Income and Tax DeductedDocument2 pagesForm No. 16: Details of Salary Paid and Any Other Income and Tax DeductedSundaresan ChockalingamNo ratings yet
- Will The Real Sex Slave Please Stand UpDocument20 pagesWill The Real Sex Slave Please Stand Upabiwilkinson90No ratings yet
- RapeDocument34 pagesRapeGurpreet Singh Mandair100% (1)
- Erp SSTDocument32 pagesErp SSTAzmi Nurse OfficialNo ratings yet
- Statistics Mcqs Paper 2013Document2 pagesStatistics Mcqs Paper 2013zeb4019100% (1)
- Hooter - 72x72mm: Terminal ConnectionDocument1 pageHooter - 72x72mm: Terminal ConnectionImran TambatNo ratings yet
- Emission Calculation 2Document12 pagesEmission Calculation 2myungkwan haNo ratings yet
- Pico LL Very Fast-Acting Fuse 251/253 SeriesDocument4 pagesPico LL Very Fast-Acting Fuse 251/253 SeriesElhadj OualiNo ratings yet
- Brown Aluminium Oxide: AlcabDocument1 pageBrown Aluminium Oxide: AlcabIssam TrikiNo ratings yet
- Intro To First Aid and Basic Life SupportDocument31 pagesIntro To First Aid and Basic Life SupportLance BaraquielNo ratings yet