You might also like
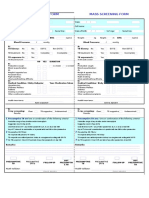
- Health Examination RecordDocument3 pagesHealth Examination RecordJuliet CorpuzNo ratings yet
- Teacher Health Card SummaryDocument3 pagesTeacher Health Card SummaryGabriel NuezNo ratings yet
- Teacher'S Health Card: 2019 SHD Form 4Document3 pagesTeacher'S Health Card: 2019 SHD Form 4Edgar LucapaNo ratings yet
- TNTP Health CardDocument4 pagesTNTP Health CardJennifer AlbaradoNo ratings yet
- Teacher'S Health Card: SHD Form 4Document4 pagesTeacher'S Health Card: SHD Form 4DINA CANDELARIANo ratings yet
- SHD Form 4 T - NTPDocument3 pagesSHD Form 4 T - NTPElle RochNo ratings yet
- Teacher'S Health Card: SHD Form 4Document3 pagesTeacher'S Health Card: SHD Form 4Jean Antoniet Acopiado LegadosNo ratings yet
- SHD Form 4 T - NTPDocument3 pagesSHD Form 4 T - NTPKENT REEVE ROSALNo ratings yet
- SHD Form 4 Teachers Health CardDocument1 pageSHD Form 4 Teachers Health CardAcorda Angelina100% (3)
- Teacher Health CardDocument1 pageTeacher Health CardMaria Fatima ArnaizNo ratings yet
- Annual Medical FromDocument4 pagesAnnual Medical FromMelodine Gev'LibresNo ratings yet
- Teacher'S Health Card: SHD Form 4Document3 pagesTeacher'S Health Card: SHD Form 4Chonie VillanuevaNo ratings yet
- SHD Form 4 T - NTPDocument3 pagesSHD Form 4 T - NTPalshed vallenteNo ratings yet
- Annual Profiling and Medical FormDocument4 pagesAnnual Profiling and Medical FormMhërvžž CatarataNo ratings yet
- Teachers Health Examination FormDocument2 pagesTeachers Health Examination FormNoly Mariano Alejandro100% (3)
- Teachers Health Examination FormDocument2 pagesTeachers Health Examination FormRosemarie Ceredon ChyNo ratings yet
- SHD Form 4 TNTP Health FormDocument3 pagesSHD Form 4 TNTP Health FormJASMIN FAMANo ratings yet
- Teacher'S Health Card: M SingleDocument3 pagesTeacher'S Health Card: M SingleNathaniel AlobaNo ratings yet
- Deped Teachers Health CardDocument8 pagesDeped Teachers Health CardMarjorie Jacinto-Tañala100% (1)
- Teachers Health Examination Form 1Document2 pagesTeachers Health Examination Form 1Wussle JumaritoNo ratings yet
- SHD Form 4 T NTP 1Document4 pagesSHD Form 4 T NTP 1Marvin LintanNo ratings yet
- Teacher'S Health Card: Male SingleDocument3 pagesTeacher'S Health Card: Male SingleAlfie Lumpay CagampangNo ratings yet
- Teacher'S Health Card: M F S M W SDocument3 pagesTeacher'S Health Card: M F S M W SKIMBERLY VARGASNo ratings yet
- Teacher's Health RecordDocument1 pageTeacher's Health Recordmike gilbert boadoNo ratings yet
- Clinic Forms All in One For TeachersDocument33 pagesClinic Forms All in One For TeachersMeriam BonghanoyNo ratings yet
- Form 86 Medical certificateDocument4 pagesForm 86 Medical certificateNARCISO GALAGALANo ratings yet
- Teacher's Health CardDocument1 pageTeacher's Health CardRien Jing TianNo ratings yet
- Teacher Health Card SummaryDocument3 pagesTeacher Health Card SummaryDEXTER LLOYD CATIAGNo ratings yet
- Form 86Document8 pagesForm 86Hanna Jane BayarcalNo ratings yet
- Teachers Annual PE Form 1Document3 pagesTeachers Annual PE Form 1Ma. Khulyn AlvarezNo ratings yet
- Medical and Dental Form For TeachersDocument7 pagesMedical and Dental Form For TeachersEarl James GalangNo ratings yet
- Health Check Up Booklet Mobo SouthDocument3 pagesHealth Check Up Booklet Mobo SouthJude GonzalesNo ratings yet
- Ponr InpDocument23 pagesPonr InpAshen GiradoNo ratings yet
- Patient Medical HistoryDocument5 pagesPatient Medical HistoryTamara WilliamsonNo ratings yet
- Teacher's Health cardSHD-AnnualPE-TeachingNonTeachingDocument4 pagesTeacher's Health cardSHD-AnnualPE-TeachingNonTeachingJudy Ann CruzNo ratings yet
- Physical Cyll 2 HR CareplanDocument9 pagesPhysical Cyll 2 HR Careplanmido hamamNo ratings yet
- Health Card TeachersDocument3 pagesHealth Card TeachersRuselle N. NavarroNo ratings yet
- Medical Record FormDocument3 pagesMedical Record FormBDL SkinNo ratings yet
- Nursing AssessmentDocument3 pagesNursing AssessmentJD AIZA CASANDRA O. SANCHEZNo ratings yet
- Patient History Edited 2019Document3 pagesPatient History Edited 2019api-468186696No ratings yet
- Medical Declaration Form - 28-10-23Document1 pageMedical Declaration Form - 28-10-23Erwadi ErwadiNo ratings yet
- MEDICAL DECLARATION FORM - v1.00Document1 pageMEDICAL DECLARATION FORM - v1.00Erwadi ErwadiNo ratings yet
- (ARLED) Pre-Natal FormDocument8 pages(ARLED) Pre-Natal FormMike Dela CruzNo ratings yet
- CompiledDocument9 pagesCompiledcogiezamoraNo ratings yet
- 2019 Certificate of Health Letter SizeDocument1 page2019 Certificate of Health Letter SizeAnonymous YG4TA3No ratings yet
- Mass Screening Form Mass Screening Form: (In The Past 2 Years) (In The Past 2 Years)Document1 pageMass Screening Form Mass Screening Form: (In The Past 2 Years) (In The Past 2 Years)Tinea nigraNo ratings yet
- PHA Individual Health Profile & Assessment Form As of Oct.09, 2017Document8 pagesPHA Individual Health Profile & Assessment Form As of Oct.09, 2017Eden VblagasyNo ratings yet
- Psych ODDocument2 pagesPsych ODsand25701No ratings yet
- (ARLED) Pre-Natal FormDocument5 pages(ARLED) Pre-Natal FormMike Dela CruzNo ratings yet
- Generic Questionnaire ManualDocument3 pagesGeneric Questionnaire Manualndagijemorice659No ratings yet
- MCU Nirmala Artha MeviaDocument3 pagesMCU Nirmala Artha MeviaHomecare AnandaNo ratings yet
- Ommc Covid 19 Checklist FinalDocument1 pageOmmc Covid 19 Checklist FinalEunice RiveraNo ratings yet
- MEDICAL FORDocument8 pagesMEDICAL FORmarandugebraNo ratings yet
- TarPr QF SGOD SHU 10teachers Health CardDocument2 pagesTarPr QF SGOD SHU 10teachers Health CardMark Jhosua Austria GalinatoNo ratings yet
- Form 4b v050120Document4 pagesForm 4b v050120Estarmio ZaficoNo ratings yet
- Anna Siska (Bu Tari)Document2 pagesAnna Siska (Bu Tari)Fetti Nur DiyantiNo ratings yet
- Nursing System Review ChartDocument2 pagesNursing System Review ChartifancyouuuNo ratings yet
- Global COVID-19 Clinical Data PlatformDocument5 pagesGlobal COVID-19 Clinical Data PlatformCecilia PinedaNo ratings yet
- Clearance Form: Tarlac State UniversityDocument2 pagesClearance Form: Tarlac State UniversityDIOSDADO MADRONIONo ratings yet
- Tayabo Elementary School: Division of San Jose CityDocument19 pagesTayabo Elementary School: Division of San Jose CityDIOSDADO MADRONIONo ratings yet
- School Report Card - 2020-2021Document20 pagesSchool Report Card - 2020-2021DIOSDADO MADRONIO100% (1)
- LNS-PA-TemplateDocument4 pagesLNS-PA-TemplateDIOSDADO MADRONIO100% (1)
- LNS-PA-TemplateDocument4 pagesLNS-PA-TemplateDIOSDADO MADRONIO100% (1)
- Hydro AquaDocument74 pagesHydro AquaDIOSDADO MADRONIONo ratings yet
- Automated Test ResultsDocument10 pagesAutomated Test ResultsDIOSDADO MADRONIONo ratings yet
- SIM SAMPLE Distance Between Two PointsDocument14 pagesSIM SAMPLE Distance Between Two PointsDIOSDADO MADRONIONo ratings yet
- I do not have access to your math book. Could you please provide the problem statements for problems 1-14 on page 232? Then I can try to solve themDocument23 pagesI do not have access to your math book. Could you please provide the problem statements for problems 1-14 on page 232? Then I can try to solve themDIOSDADO MADRONIONo ratings yet
- School Form 10 SF10 Learner's Permanent Academic Record For Elementary SchoolDocument10 pagesSchool Form 10 SF10 Learner's Permanent Academic Record For Elementary SchoolSheila Jean Dacillo85% (26)
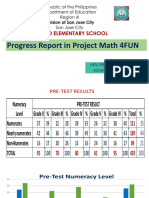
- Progress Report in Math 4FUNDocument16 pagesProgress Report in Math 4FUNDIOSDADO MADRONIONo ratings yet
- Circulation and Blood 1B.1Document17 pagesCirculation and Blood 1B.1tas xoNo ratings yet
- The Relationship Between Lower Intelligence Crime and Custodial Outcomes A Brief Literary Review of A Vulnerable GroupDocument16 pagesThe Relationship Between Lower Intelligence Crime and Custodial Outcomes A Brief Literary Review of A Vulnerable GroupSteveNo ratings yet
- NASKAH-PUBLIKASI (1) Nanot HalamanDocument13 pagesNASKAH-PUBLIKASI (1) Nanot HalamanNurul FitrianiNo ratings yet
- 02 Id Ego and Super EgoDocument11 pages02 Id Ego and Super EgoEmraan MalikNo ratings yet
- Medication AdministrationDocument61 pagesMedication Administrationkerema BadasaNo ratings yet
- Timeless Beauty - Over 100 Tips, Secrets, and Shortcuts To Looking Great (PDFDrive)Document488 pagesTimeless Beauty - Over 100 Tips, Secrets, and Shortcuts To Looking Great (PDFDrive)Isabel Matta100% (1)
- Chapter 20 Tobacco: Lesson 2 Choosing To Live Tobacco FreeDocument2 pagesChapter 20 Tobacco: Lesson 2 Choosing To Live Tobacco Freeroshni rNo ratings yet
- Immuno GlowDocument11 pagesImmuno GlowNoly ClaveringNo ratings yet
- A Quick Guide For Busy Parents: Connect and Re-Direct Name It To Tame ItDocument1 pageA Quick Guide For Busy Parents: Connect and Re-Direct Name It To Tame ItSanjeev Sharma100% (2)
- Operational Management Assignment PDFDocument7 pagesOperational Management Assignment PDFYonas D. EbrenNo ratings yet
- Programmatic Safety Plan (PSP) : Required For High Risk Routine & Repetitive WorkDocument4 pagesProgrammatic Safety Plan (PSP) : Required For High Risk Routine & Repetitive WorkSteve ParkerNo ratings yet
- Mom 202108003Document2 pagesMom 202108003Ckucku AranetaNo ratings yet
- Annex4 fm1Document2 pagesAnnex4 fm1jhenny lazarteNo ratings yet
- G7M-1055-05 - On-Line Visual Inspection Procedures and ChecklistDocument1 pageG7M-1055-05 - On-Line Visual Inspection Procedures and ChecklistMohammad Qureshi100% (1)
- Trainee's Record Book SWBLDocument12 pagesTrainee's Record Book SWBLaaronjules100% (2)
- Pa RewriteDocument6 pagesPa Rewriteapi-611938804No ratings yet
- Columbia-Suicide Severity Rating Scale (C-SSRS) : Past 3 Months LifetimeDocument1 pageColumbia-Suicide Severity Rating Scale (C-SSRS) : Past 3 Months LifetimeIzabel EstevamNo ratings yet
- Birth NotesDocument9 pagesBirth Notesrakesh180814No ratings yet
- C Is New India Floater Medi Claim PolicyDocument12 pagesC Is New India Floater Medi Claim PolicyDeepan ManojNo ratings yet
- End of Life Care GuideDocument79 pagesEnd of Life Care GuideAbcd TolibasNo ratings yet
- Treatment Plan PortfolioDocument2 pagesTreatment Plan Portfolioapi-518560779No ratings yet
- Abstract of ThesisDocument2 pagesAbstract of ThesisdrkartikeytyagiNo ratings yet
- Professional Teachers (Secondary) 10-2022 FilipinoDocument26 pagesProfessional Teachers (Secondary) 10-2022 FilipinoPRC Baguio100% (1)
- Presentation 1Document6 pagesPresentation 1Joarlin BianesNo ratings yet
- DLL Health 9 & 10Document6 pagesDLL Health 9 & 10Gladys GutierrezNo ratings yet
- Diag AutismoDocument12 pagesDiag AutismoSandra Carranza ZavalaNo ratings yet
- Calif Organic Fertilizers 2012 Label BookDocument40 pagesCalif Organic Fertilizers 2012 Label BookOrganicXpertNo ratings yet
- HS ConsultantDocument2 pagesHS Consultantdeeman4yahNo ratings yet
- 4.1.10 Practice Grammar FeedbackDocument10 pages4.1.10 Practice Grammar FeedbackbaileyNo ratings yet
- Case ReportDocument13 pagesCase ReportZaryab Waheed0% (1)