You might also like
- Deped Teachers Health CardDocument8 pagesDeped Teachers Health CardMarjorie Jacinto-Tañala100% (1)
- SHD Form 4 Teachers Health CardDocument1 pageSHD Form 4 Teachers Health CardAcorda Angelina100% (3)
- PHA Individual Health Profile & Assessment Form As of Oct.09, 2017Document8 pagesPHA Individual Health Profile & Assessment Form As of Oct.09, 2017Eden VblagasyNo ratings yet
- Nursing System Review ChartDocument2 pagesNursing System Review ChartifancyouuuNo ratings yet
- Mga Mumunting Magsasaka v1.0Document36 pagesMga Mumunting Magsasaka v1.0Elle RochNo ratings yet
- Teacher'S Health Card: SHD Form 4Document4 pagesTeacher'S Health Card: SHD Form 4DINA CANDELARIANo ratings yet
- SHD Form 4 T - NTPDocument3 pagesSHD Form 4 T - NTPKENT REEVE ROSALNo ratings yet
- Teacher'S Health Card: SHD Form 4Document3 pagesTeacher'S Health Card: SHD Form 4Jean Antoniet Acopiado LegadosNo ratings yet
- TNTP Health CardDocument4 pagesTNTP Health CardJennifer AlbaradoNo ratings yet
- Teacher Health CardDocument1 pageTeacher Health CardMaria Fatima ArnaizNo ratings yet
- Teacher'S Health Card: 2019 SHD Form 4Document3 pagesTeacher'S Health Card: 2019 SHD Form 4Edgar LucapaNo ratings yet
- Teacher Health Card SummaryDocument3 pagesTeacher Health Card SummaryGabriel NuezNo ratings yet
- SHD Form 4 T - NTP Aug 7Document5 pagesSHD Form 4 T - NTP Aug 7DIOSDADO MADRONIONo ratings yet
- Teacher'S Health Card: SHD Form 4Document3 pagesTeacher'S Health Card: SHD Form 4Chonie VillanuevaNo ratings yet
- Annual Medical FromDocument4 pagesAnnual Medical FromMelodine Gev'LibresNo ratings yet
- Health Examination RecordDocument3 pagesHealth Examination RecordJuliet CorpuzNo ratings yet
- SHD Form 4 T - NTPDocument3 pagesSHD Form 4 T - NTPalshed vallenteNo ratings yet
- Annual Profiling and Medical FormDocument4 pagesAnnual Profiling and Medical FormMhërvžž CatarataNo ratings yet
- Teachers Health Examination FormDocument2 pagesTeachers Health Examination FormNoly Mariano Alejandro100% (3)
- Teachers Health Examination FormDocument2 pagesTeachers Health Examination FormRosemarie Ceredon ChyNo ratings yet
- Teacher'S Health Card: M SingleDocument3 pagesTeacher'S Health Card: M SingleNathaniel AlobaNo ratings yet
- SHD Form 4 TNTP Health FormDocument3 pagesSHD Form 4 TNTP Health FormJASMIN FAMANo ratings yet
- SHD Form 4 T NTP 1Document4 pagesSHD Form 4 T NTP 1Marvin LintanNo ratings yet
- Teachers Health Examination Form 1Document2 pagesTeachers Health Examination Form 1Wussle JumaritoNo ratings yet
- Teacher'S Health Card: Male SingleDocument3 pagesTeacher'S Health Card: Male SingleAlfie Lumpay CagampangNo ratings yet
- Teacher'S Health Card: M F S M W SDocument3 pagesTeacher'S Health Card: M F S M W SKIMBERLY VARGASNo ratings yet
- Form 86 Medical certificateDocument4 pagesForm 86 Medical certificateNARCISO GALAGALANo ratings yet
- Teacher's Health RecordDocument1 pageTeacher's Health Recordmike gilbert boadoNo ratings yet
- Teacher's Health CardDocument1 pageTeacher's Health CardRien Jing TianNo ratings yet
- Teacher Health Card SummaryDocument3 pagesTeacher Health Card SummaryDEXTER LLOYD CATIAGNo ratings yet
- Form 86Document8 pagesForm 86Hanna Jane BayarcalNo ratings yet
- Clinic Forms All in One For TeachersDocument33 pagesClinic Forms All in One For TeachersMeriam BonghanoyNo ratings yet
- Teachers Annual PE Form 1Document3 pagesTeachers Annual PE Form 1Ma. Khulyn AlvarezNo ratings yet
- Medical and Dental Form For TeachersDocument7 pagesMedical and Dental Form For TeachersEarl James GalangNo ratings yet
- Health Check Up Booklet Mobo SouthDocument3 pagesHealth Check Up Booklet Mobo SouthJude GonzalesNo ratings yet
- Teacher's Health cardSHD-AnnualPE-TeachingNonTeachingDocument4 pagesTeacher's Health cardSHD-AnnualPE-TeachingNonTeachingJudy Ann CruzNo ratings yet
- Patient Medical HistoryDocument5 pagesPatient Medical HistoryTamara WilliamsonNo ratings yet
- Ponr InpDocument23 pagesPonr InpAshen GiradoNo ratings yet
- Physical Cyll 2 HR CareplanDocument9 pagesPhysical Cyll 2 HR Careplanmido hamamNo ratings yet
- Health Card TeachersDocument3 pagesHealth Card TeachersRuselle N. NavarroNo ratings yet
- Medical Record FormDocument3 pagesMedical Record FormBDL SkinNo ratings yet
- Patient History Edited 2019Document3 pagesPatient History Edited 2019api-468186696No ratings yet
- Nursing AssessmentDocument3 pagesNursing AssessmentJD AIZA CASANDRA O. SANCHEZNo ratings yet
- Medical Declaration Form - 28-10-23Document1 pageMedical Declaration Form - 28-10-23Erwadi ErwadiNo ratings yet
- MCU Nirmala Artha MeviaDocument3 pagesMCU Nirmala Artha MeviaHomecare AnandaNo ratings yet
- Generic Questionnaire ManualDocument3 pagesGeneric Questionnaire Manualndagijemorice659No ratings yet
- CompiledDocument9 pagesCompiledcogiezamoraNo ratings yet
- MEDICAL DECLARATION FORM - v1.00Document1 pageMEDICAL DECLARATION FORM - v1.00Erwadi ErwadiNo ratings yet
- 2019 Certificate of Health Letter SizeDocument1 page2019 Certificate of Health Letter SizeAnonymous YG4TA3No ratings yet
- (ARLED) Pre-Natal FormDocument8 pages(ARLED) Pre-Natal FormMike Dela CruzNo ratings yet
- Wallace State Community College NURSING DATABASE: Nursing HomeDocument9 pagesWallace State Community College NURSING DATABASE: Nursing HomeEnger NushunNo ratings yet
- (ARLED) Pre-Natal FormDocument5 pages(ARLED) Pre-Natal FormMike Dela CruzNo ratings yet
- Mass Screening Form Mass Screening Form: (In The Past 2 Years) (In The Past 2 Years)Document1 pageMass Screening Form Mass Screening Form: (In The Past 2 Years) (In The Past 2 Years)Tinea nigraNo ratings yet
- New Patient Questionnaire Physical Therapy: Chief ComplaintDocument4 pagesNew Patient Questionnaire Physical Therapy: Chief ComplaintAstonNo ratings yet
- New Patient Paperwork 10 2023Document7 pagesNew Patient Paperwork 10 2023María CristinaNo ratings yet
- 2013 MedicalsDocument5 pages2013 MedicalsSebastia Felipe SolisNo ratings yet
- Form 4b v050120Document4 pagesForm 4b v050120Estarmio ZaficoNo ratings yet
- MEDICAL FORDocument8 pagesMEDICAL FORmarandugebraNo ratings yet
- Anna Siska (Bu Tari)Document2 pagesAnna Siska (Bu Tari)Fetti Nur DiyantiNo ratings yet
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicFrom EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicRating: 5 out of 5 stars5/5 (1)
- Attendance ChartDocument4 pagesAttendance ChartElle RochNo ratings yet
- School Form 10 SF10 Learner's Permanent Academic Record For Elementary SchoolDocument10 pagesSchool Form 10 SF10 Learner's Permanent Academic Record For Elementary SchoolSheila Jean Dacillo85% (26)
- Drop Everything and ReadDocument34 pagesDrop Everything and ReadElle RochNo ratings yet
- Clinic Cover PageDocument3 pagesClinic Cover PageElle RochNo ratings yet
- School Form Front PageDocument52 pagesSchool Form Front PageElle RochNo ratings yet
- Dance Rubrics For AssessmentDocument3 pagesDance Rubrics For AssessmentElle RochNo ratings yet
- RubricsDocument6 pagesRubricsElle RochNo ratings yet
- Navarro Elementary School Weekly Learning Plan for Grade 4Document2 pagesNavarro Elementary School Weekly Learning Plan for Grade 4Elle RochNo ratings yet
- DLL TrackingDocument2 pagesDLL TrackingElle RochNo ratings yet
- Learning Continuity Plan for Navarro Elementary SchoolDocument35 pagesLearning Continuity Plan for Navarro Elementary SchoolElle RochNo ratings yet
- Grade 4 report cardDocument4 pagesGrade 4 report cardElle RochNo ratings yet
- Summary Report On Reading of Forms FormatDocument3 pagesSummary Report On Reading of Forms FormatElle RochNo ratings yet
- 02 WinS Monitoring System - Blank v2017 06 04Document16 pages02 WinS Monitoring System - Blank v2017 06 04Elle RochNo ratings yet
- Developing Reading PowerDocument6 pagesDeveloping Reading PowerElle RochNo ratings yet
- Template Ndep Accomplishment ReportDocument3 pagesTemplate Ndep Accomplishment ReportElle RochNo ratings yet
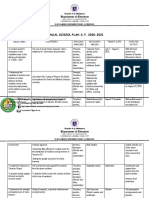
- Navarro Elementary School's Annual School Plan for S.Y. 2020-2021Document6 pagesNavarro Elementary School's Annual School Plan for S.Y. 2020-2021Elle RochNo ratings yet
- Deworming TemplateDocument4 pagesDeworming TemplateElle RochNo ratings yet
- Grade 4-6 - Summary Final GradesDocument12 pagesGrade 4-6 - Summary Final GradesArnel TanNo ratings yet
- The Lion and The MouseDocument1 pageThe Lion and The MouseMaiaHozNo ratings yet
- Science Activities-1st QuarteDocument25 pagesScience Activities-1st QuarteElle RochNo ratings yet
- Iv. Scaling and RankingDocument4 pagesIv. Scaling and RankingWenalyn Grace Abella LlavanNo ratings yet
- Common Health Problems in ChildrenDocument5 pagesCommon Health Problems in ChildrenLezrae Chescka Javier IlumbaNo ratings yet
- COVID-19 Vaccine Information SheetDocument11 pagesCOVID-19 Vaccine Information SheetKirbyCronoNo ratings yet
- Dysphagia After Stroke-An Overview PDFDocument18 pagesDysphagia After Stroke-An Overview PDFDhea SafitriNo ratings yet
- Submitted By: Swati Markandey Ashish Arya: Department of Pedodontics Govt. College of Dentistry, IndoreDocument40 pagesSubmitted By: Swati Markandey Ashish Arya: Department of Pedodontics Govt. College of Dentistry, Indorepriti adsulNo ratings yet
- 6513885brainy Kl6 Unit Test 6 ADocument3 pages6513885brainy Kl6 Unit Test 6 Akarola100% (1)
- Anemia at Older AgeDocument10 pagesAnemia at Older AgeAbdullah ZuhairNo ratings yet
- Daftar Pustaka Covid-19 LiteratureDocument4 pagesDaftar Pustaka Covid-19 LiteratureReynida HutagalungNo ratings yet
- DiverticulitisDocument27 pagesDiverticulitisBad AssNo ratings yet
- 2019 - Chelation Therapy in Medicine - Derrick Lonsdale Hormones MatterDocument9 pages2019 - Chelation Therapy in Medicine - Derrick Lonsdale Hormones MatterSimon SaundersNo ratings yet
- Nur3111p Professionalism and Lifelong Learning ReflectionDocument6 pagesNur3111p Professionalism and Lifelong Learning Reflectionapi-578141969No ratings yet
- Anatomy, Abdomen and Pelvis, Female External Genitalia - StatPearls - NCBI BookshelfDocument1 pageAnatomy, Abdomen and Pelvis, Female External Genitalia - StatPearls - NCBI Bookshelfpapoy123100% (1)
- Pregabalin Sciecure 25 MG, 50 MG, 75 MG, 100 MG, 150 MG, 200 MG, 225 MG, 300 MG Hard CapsulesDocument8 pagesPregabalin Sciecure 25 MG, 50 MG, 75 MG, 100 MG, 150 MG, 200 MG, 225 MG, 300 MG Hard CapsulesA-OUafi SeDDikiNo ratings yet
- Acute Pancreatitis in Children Fact SheetDocument3 pagesAcute Pancreatitis in Children Fact SheetNikola StojsicNo ratings yet
- Disorder of OsmoregulationDocument15 pagesDisorder of OsmoregulationiavahhoNo ratings yet
- Advanced Diploma in Applied Yoga and NaturotpathyDocument11 pagesAdvanced Diploma in Applied Yoga and NaturotpathyMonica ChoudharyNo ratings yet
- Urinary Tract Infections and Prostatitis GuideDocument10 pagesUrinary Tract Infections and Prostatitis GuideJane DoeNo ratings yet
- Module - Iii: Introduction To NaturopathyDocument10 pagesModule - Iii: Introduction To Naturopathysudinavada2009No ratings yet
- Toxic Megacolon: Daniel M. Autenrieth, MD, and Daniel C. Baumgart, MD, PHDDocument8 pagesToxic Megacolon: Daniel M. Autenrieth, MD, and Daniel C. Baumgart, MD, PHDGoran TomićNo ratings yet
- GASTROENTEROLOGY Maintenancy of Certification MOC ExaminationDocument11 pagesGASTROENTEROLOGY Maintenancy of Certification MOC ExaminationDannyNo ratings yet
- Biological Explanations of Eating DisordersDocument1 pageBiological Explanations of Eating DisordersMaggie PampinNo ratings yet
- MINDMAPDocument2 pagesMINDMAPrayzaoliveira.ausNo ratings yet
- The Therapeutics of Fever - 5fbded32d6a27Document29 pagesThe Therapeutics of Fever - 5fbded32d6a27Tariq MehmoodNo ratings yet
- Chain of Infection Content: 1. Chain of Infection. 2. Roles and Functions of The Nurse in The Chain of Infection. Chain of InfectionDocument3 pagesChain of Infection Content: 1. Chain of Infection. 2. Roles and Functions of The Nurse in The Chain of Infection. Chain of InfectionRespicio Christian Aejay G.No ratings yet
- Diabetes Case Presentation: Managing ComplicationsDocument7 pagesDiabetes Case Presentation: Managing Complicationskhalid.zainabNo ratings yet
- Basic of Geriatrics and Internal Medicine For PhysiotherapistDocument128 pagesBasic of Geriatrics and Internal Medicine For PhysiotherapistDoha EbedNo ratings yet
- Ampicillin Drug Study GuideDocument3 pagesAmpicillin Drug Study GuideAlyssa Mae DumularNo ratings yet
- Diabetic Foot Care Before and During The COVID-19 Epidemic: What Really Matters?Document2 pagesDiabetic Foot Care Before and During The COVID-19 Epidemic: What Really Matters?SitiNo ratings yet
- Branches and concepts of pharmacologyDocument15 pagesBranches and concepts of pharmacologyZaira Reine SantosNo ratings yet
- Wilson Disease in Children and Young Adults - State of The ArtDocument11 pagesWilson Disease in Children and Young Adults - State of The ArtJosueNo ratings yet