Professional Documents
Culture Documents
Escoliosis Idiopatica Infantil
Uploaded by
suad5stambulieOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Escoliosis Idiopatica Infantil
Uploaded by
suad5stambulieCopyright:
Available Formats
Early Onset Idiopathic
Scoliosis
Bruce L. Gillingham, MD, Abstract
CAPT, MC, USN Children with early onset scoliosis typically present before age 5
Ryan A. Fan, MD, LT, MC, years. Radiographic criteria help to distinguish progressive cases
USNR from those that will spontaneously resolve. Severe
cardiopulmonary problems may occur in untreated progressive
Behrooz A. Akbarnia, MD
cases. A comprehensive evaluation should be performed to identify
commonly associated conditions, such as plagiocephaly, congenital
heart disease, inguinal hernia, and hip dysplasia. For curves >20°,
magnetic resonance imaging of the neural axis is indicated to rule
out occult central nervous system lesions. Surgical management
Dr. Gillingham is Director, Surgical
Services, Naval Medical Center, San should be considered when nonsurgical measures, including
Diego, CA, and Assistant Professor of bracing and casting, fail to arrest progression. Surgical methods
Surgery, Uniformed Services University
continue to evolve and are primarily directed at obtaining and
of the Health Sciences, Bethesda, MD.
Dr. Fan is Resident, Orthopaedic
maintaining curve correction while simultaneously preserving
Surgery, Naval Medical Center, San spinal and trunk growth.
Diego. Dr. Akbarnia is Clinical Professor
of Orthopaedic Surgery, University of
California, San Diego, and Medical
T
Director, San Diego Center for Spinal reatment of children with pro- In 1954, James2 described three
Disorders, La Jolla, CA. gressive scoliosis occurring be- categories of idiopathic scoliosis ac-
None of the following authors or the fore age 5 years is challenging. Left cording to the age of onset: infantile,
departments with which they are untreated, progressive curves may with curves present before age 3
affiliated has received anything of value produce significant thoracic defor- years; juvenile, with curves appear-
from or owns stock in a commercial mity, leading to deleterious effects ing between the ages of 4 and 9
company or institution related directly or on the cardiopulmonary system. As years; and adolescent, in which
indirectly to the subject of this article: James et al1 observed in 1959, pro- curves present from age 10 years un-
Dr. Gillingham and Dr. Fan. Dr. Akbarnia gressive early onset scoliosis “devel- til the end of growth. These three pe-
or the departments with which he is ops rapidly and relentlessly, causing riods were thought to correspond to
affiliated has received royalties from the severest form of orthopaedic distinct periods of increased growth
DePuy Spine. Dr. Akbarnia or the cripple with dreadful deformity, velocity during childhood and ado-
departments with which he is affiliated marked dwarfing and shortening of lescence. In fact, during the juvenile
serves as a consultant to or is an life.” Standard treatment options for period, there is a deceleration in spi-
employee of DePuy Spine. adolescent scoliosis, including brac- nal growth, and onset of scoliosis is
Reprint requests: Dr. Akbarnia, San ing and spinal fusion, have limited uncommon.3,4 More recently, the
Diego Center for Spinal Disorders, Suite use in much younger children be- term “early onset” has been used to
300, 4130 La Jolla Village Drive, La cause of potential adverse effects on reflect the presence of scoliosis of all
Jolla, CA 92037-1481. the developing spine, chest wall, and etiologies by age 5 years; “late on-
lungs. Successful management of set” is used to describe the appear-
J Am Acad Orthop Surg 2006;14:101-
idiopathic scoliosis requires under- ance of scoliosis after age 5 years.5
112
standing the etiology, natural his- These terms more accurately reflect
Copyright 2006 by the American tory, evaluation, and available non- the physiologic basis of and clinical
Academy of Orthopaedic Surgeons. surgical and surgical management experience with this condition. The
options for these patients. distinction between early and late
Volume 14, Number 2, February 2006 101
Early Onset Idiopathic Scoliosis
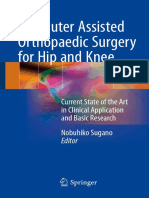
Figure 1 strate a much more favorable
outcome.8-11 Magnetic resonance im-
2.5 aging (MRI) evaluation of the neural
2 2 axis was unavailable at the time of
2
1.75 these reports, however. In 1951,
1.5
1.25
James8 identified a pattern of scolio-
cm/year
1.25 1.25
1 sis he termed “infantile idiopathic
1
0.75 0.75 scoliosis,” involving primarily in-
0.75 0.5
0.5 fant boys with a left mid or lower
0 .25 thoracic curve. Only 4 of 33 patients
Age 1 Age 5 Age 10 Age 15 (12%) resolved. In contrast, Lloyd-
Roberts and Pilcher10 reported on
T1-L5 T1-T12 L1-L5
100 patients with structural curves
diagnosed within the first year of
life. Ninety-two percent of the
Spinal growth velocity from ages 1 through 15 years. (Adapted with permission curves resolved spontaneously. In
from Dimeglio A: Growth of the spine before age 5 years. J Pediatr Orthop B their study of 99 infants, Ceballos et
1993;1:102-107.) al11 reported progression in 26%.
The original hypothesis that in-
fantile cases were caused by intra-
onset is important because of the po- age 10 years and after but does not uterine molding was refuted by the
tential for serious cardiopulmonary equal the velocity occurring before absence of scoliosis at birth. Scott
compromise in patients in whom age 5 years3 (Figure 1). Overall, the and Morgan9 compared the inci-
scoliosis appears before age 5 years. height of the thoracic spine doubles dence of idiopathic scoliosis in En-
between birth and skeletal maturity. gland and the United States, as re-
Thoracic volume is approximately ported by the Research Committee
Basic Science
6% of adult volume at birth, reach- of the American Orthopaedic Asso-
Anatomy, Growth, and ing roughly 30% of adult volume by ciation in 1941. Twenty-eight of 218
Development age 5 years and 50% by age 10 years. patients from England presented
Knowledge of the normal growth Final thoracic volume is achieved by with idiopathic scoliosis before age 2
of the chest, spine, and pulmonary age 15 years in both boys and girls.3 years, compared with only 1 of 404
system is essential in understanding patients in the United States. Mau12
the effect of scoliosis on these struc- Etiology subsequently proposed that postna-
tures. The number of alveoli in the Several causes have been identi- tal pressure caused by constant ob-
terminal respiratory unit rapidly in- fied for early onset scoliosis, includ- lique supine positioning in European
creases in number and volume dur- ing congenital vertebral anomalies, infants (compared with prone posi-
ing the first year of life. The number neuromuscular conditions (eg, cere- tioning in North American babies)
of alveoli increases more than 10- bral palsy, myelomeningocele, mus- was responsible for this difference in
fold between birth and adulthood, cular dystrophies), associated syn- incidence. He also noted associated
primarily during the first 8 years of dromes (eg, neurofibromatosis), and ipsilateral plagiocephaly (an asym-
life.6 In addition, the number of re- structural lesions of the central ner- metric and twisted head in reference
spiratory branches increases from 21 vous system (eg, diastematomyelia, to the spine), pelvic flattening and
at age 3 months to 23 at age 8 syrinx, tethered cord). Patients with obliquity, and hip adduction. This
years.7 no obvious associated abnormalities proposed correlation between infant
The significant increase in are considered to have early onset id- positioning and early onset scoliotic
growth of the lung parenchyma is iopathic scoliosis. deformities is disquieting and war-
paralleled by corresponding growth rants further research in light of the
of the spine and chest. Two thirds of Natural History current trend in American pediatrics
the final sitting height is achieved by In contrast with late-onset dis- to recommend positioning infants
age 5 years.3 The growth velocity of ease, early onset idiopathic scoliosis, supine to reduce the risk of sudden
the T1 to L5 segment is greatest specifically infantile idiopathic infant death syndrome.13
from birth to age 5 years, averaging scoliosis, spontaneously resolves in Several factors, such as age of on-
>2 cm per year, with marked decel- a large number of patients. Although set; location, type and magnitude of
eration between ages 5 and 10 years. early series reported a low incidence the scoliotic curve; associated devel-
Growth velocity increases again at of resolution, later reports demon- opmental anomalies; sex; and fami-
102 Journal of the American Academy of Orthopaedic Surgeons
Bruce L. Gillingham, MD, CAPT, MC, USN, et al
Figure 2 develop when the vital capacity re-
mains >40% of the predicted normal
value.
Clinically, there is a far greater
risk of cardiorespiratory complica-
tion when scoliosis is apparent be-
fore age 5 years. Even in the absence
of associated disease, disabling or
life-threatening respiratory failure is
relatively common and is likely to
present at or before late middle
age.17,19
Physical Examination
To measure the rib-vertebra angle difference, a line is drawn perpendicular to the
end plate of the apical vertebrae (a). Next, a line is drawn from the midpoint of the The evaluation of a child with sus-
neck of the rib through the midpoint of the head of the rib to the perpendicular on pected spinal deformity should begin
the convex side (b). The resultant angle is calculated. The angle on the concave side with a comprehensive history and
is calculated in a similar manner. Concave − convex = rib-vertebra angle difference. physical examination. Given that
(Adapted with permission from Mehta MH: The rib-vertebra angle in the early
the presence of cognitive delay has
diagnosis between resolving and progressive infantile scoliosis. J Bone Joint Surg
been shown to correlate with curve
Br 1972;54:230-243.)
progression, particular attention
should be paid to whether the child
ly history, have been proposed as This effect is directly related to the has appropriately reached develop-
predictors of curve progression. The age of onset. The most hypoplastic mental milestones.20,21 It is also im-
most reliable indicator, however, is lungs are found in patients with the portant to obtain a birth history; ear-
the rib-vertebra angle difference earliest onset of scoliosis.17 ly onset idiopathic scoliosis has been
(RVAD), reported by Mehta14 in 1972 Patients with scoliosis demon- noted to occur more frequently with
(Figure 2). strate a restrictive pattern of lung breech presentation and in prema-
Progressive scoliosis during the disease, with reduction in vital ca- ture, low-birth-weight males.21
first 5 years of life may negatively af- pacity and total lung capacity along A thorough physical examination
fect the normal development of the with increased residual volume. should be performed, beginning with
lungs, chest wall, and spine. The pri- This reflects decreased compliance a search for cutaneous markers of
mary effect of scoliosis on the devel- of both the lung and chest wall. In systemic disorders, such as the café
oping lung is its inhibition of the children with early onset curves, the au lait spots and axillary freckling
growth of both alveoli and pulmo- amount by which vital capacity is observed in neurofibromatosis and
nary arterioles. This incomplete reduced depends on the severity of the hairy patch associated with oc-
maturation of the lung and pulmo- the deformity. This severity has lit- cult spinal dysraphism. Evidence of
nary vasculature is the primary tle or no effect on vital capacity in chest wall and shoulder height
cause of the ventilation defect seen patients whose curves begin in ado- asymmetry, trunk imbalance, and
in patients with early onset scolio- lescence.15 Ultimately, severe re- pelvic obliquity are sought. Flexibil-
sis.15 Although progressive distor- strictive lung disease causes alveolar ity of the scoliosis should be as-
tion of the pulmonary architecture hypoventilation, hypoxic vasocon- sessed: the patient is laid horizontal-
by increasing deformity of the spine striction, and, eventually, pulmo- ly over the examiner’s knee with the
and thorax would be thought to nary arterial hypertension and cor convex side downward, or by hold-
compress the developing alveoli, pulmonale. Arterial hypoxemia in ing the infant suspended under the
this has not been observed. Histolog- scoliosis patients is primarily caused arms, looking for correction of cur-
ic studies of lung tissue in patients by a decrease in minute ventilation vature with lateral pressure. Curves
with early onset scoliosis demon- secondary to small tidal volumes that correct are considered to be flex-
strate alveoli that are normal in rather than an impairment in gas ex- ible; those that do not are termed
shape and outline but diminished in change.18 The smallest tidal vol- rigid. The relative rigidity of the
number. In addition, the number of umes and greatest decreases in curve is an approximate clinical in-
alveoli for a given lung volume was minute ventilation are seen in pa- dicator of the likelihood of scoliosis
diminished more than could be ac- tients with the highest Cobb angles. progression and should be correlated
counted for by limitation of space.16 Cardiorespiratory failure does not with the RVAD and Cobb angle.22
Volume 14, Number 2, February 2006 103
Early Onset Idiopathic Scoliosis
Figure 3
Convex
Convex
Concave Concave
A B
A, Phase 1 rib-vertebrae relationship demonstrating no overlap of the rib head and vertebral body. B, Phase 2 rib-vertebrae
relationship. The overlap of the rib head on the vertebral body is indicative of curve progression. (Adapted with permission from
Mehta MH: The rib-vertebra angle in the early diagnosis between resolving and progressive infantile scoliosis. J Bone Joint
Surg Br 1972;54:230-243.)
Lower extremity limb-length equal- and rib asymmetry and respiratory phase 1 curves resolved. Of those
ity is verified to rule out nonstruc- insufficiencies, more frequent pul- that resolved, 83% had an RVAD
tural scoliosis, particularly in the monary function tests may be re- <20°, with a mean RVAD of 11.7°.
ambulatory child with a predomi- quired. Pulmonary function tests are The progressive group demonstrated
nant lumbar curve. difficult to obtain before age 5 years. a mean RVAD of 25.5°; 84% had an
Following this focused evaluation Other techniques to assess lung RVAD >20°.
of the scoliotic curve and its second- function and volume, such as three- In a series of 132 patients, Ferrei-
ary manifestations, the patient is ex- dimensional computed tomography, ra et al26 confirmed these findings,
amined for conditions associated provide valuable information in de- reporting that 67 of 68 resolving
with early onset idiopathic scoliosis. termining the severity of the pa- curves had an angle difference <20°;
Plagiocephaly, which is extremely tient’s condition and the timing and all were in a phase 1 relationship,
common, is found in most patients effect of surgical intervention.25 and only two had a Cobb angle >30°.
with early onset idiopathic scoliosis. Of the progressive curves in that
Developmental dysplasia of the hip, study, 37 of 40 had an RVAD ≥20°,
Radiographic
inguinal hernia, and congenital heart with two of the remaining three dis-
Evaluation
disease are found at a higher frequen- playing an increased RVAD to >21°
cy in patients with early onset idio- Anteroposterior and lateral radio- by the first year.
pathic scoliosis than in children graphs with full-length spinal views The RVAD is also useful in de-
without scoliosis.20,21,23 should be obtained to evaluate both tecting the lumbar component of
Finally, a careful neurologic ex- the Cobb angle and the RVAD.14 early double curves. Detecting dou-
amination, including assessment of These radiographs are also helpful in ble curves is important because they
muscle tone and reflexes, is imper- ruling out other associated vertebral, are highly likely to progress.11 Meh-
ative to detect occult central ner- lumbosacral, and hip joint abnor- ta14 noted key radiographic features
vous system abnormalities. Superfi- malities. The RVAD (Figure 2) is use- of the early double curve: the near
cial abdominal reflex also should be ful in predicting curve progression symmetric alignment of the apical
examined for abnormalities because when there is no overlap of the rib ribs with a resultant low RVAD of
it may be the only clue to an under- heads on the apical vertebra (phase 1 the thoracic curve, downward obliq-
lying syringomyelia with an asso- relationship)14 (Figure 3, A). An uity of the twelfth rib on the con-
ciated Chiari I malformation. The RVAD >20° indicates a high likeli- cave side of the curve, and vertebral
superficial abdominal reflex is char- hood of curve progression; curves rotation in opposite directions in the
acteristically absent on the same with RVAD measuring <20° are thoracic and lumbar vertebrae.
side as the curve convexity.24 more likely to resolve. A phase 2 re- Recent attention has focused on
Consideration should be given to lationship, in which a rib head over- defining the role of special imaging
obtaining a pediatric pulmonology laps the apical vertebra, implies that for patients with early onset scolio-
evaluation, at least at the beginning progression is certain; thus, the sis. In contrast to patients with late-
and again at the end of treatment. In RVAD is not measured14 (Figure 3, onset scoliosis, the incidence of
the presence of significant chest wall B). In the Mehta study,14 46 of the 86 occult central nervous system ab-
104 Journal of the American Academy of Orthopaedic Surgeons
Bruce L. Gillingham, MD, CAPT, MC, USN, et al
Figure 4 mended performing total spine MRI
in patients with early onset curves
Early onset measuring ≥20°.28
scoliosis (< age 5)
Absent abdominal Comprehensive history and Significant Management
reflexes or physical examination and nonorthopaedic
Cobb angle >20° scoliosis radiographs findings Nonsurgical
No The treatment of children with
No
Yes
Yes early onset scoliosis is based on an-
ticipated or actual curve progression
Continue with nonsurgical
(Figure 4). Mehta’s prognostic crite-
orthopaedic management; Specialty referral for
MRI of spinal cord, ria have proved to be very helpful in
No progression to Cobb angle nonorthopaedic
positive finding
>25°, RVAD >20°, conditions differentiating between resolving
or positive phase 2 rib
Yes relationship and progressive curves. Curves with
Cobb angles <25° with an RVAD
Yes <20° are at low risk for progression.
Neurosurgery Casting/bracing
specialty evaluation
These patients may be observed and
No should be reevaluated with serial ra-
Good response diographs every 4 to 6 months. Ac-
tive treatment should be initiated
No with curve progression >10°. Upon
Serial observation
Yes
curve resolution, follow-up at 1- to
every 4-6 months
Consider surgical 2-year intervals until maturity is
intervention prudent to ensure that there is no re-
Progression of currence during the adolescent
curve Growing rod ±
Yes
anterior release
growth spurt. A recent long-term
Other study of resolving curves validated
No emerging
techniques the use of the RVAD and demon-
Serial lengthenings strated that there was no advantage
every 4-6 months of supine plaster bed treatment over
Annual clinical
examination until physiotherapy in regard to either
skeletal maturity
Possible removal of time to resolution or functional out-
instrumentation and come.29
continued observation Definitive fusion
Infants with an RVAD >20° or a
phase 2 rib-vertebral relationship
and a Cobb angle between 20° and
Treatment algorithm for early onset (<5 years) idiopathic scoliosis. MRI = magnetic 35° have a high likelihood of progres-
resonance imaging, RVAD = rib-vertebra angle difference
sion. When a child presents with a
curve >35°, immediate treatment
normalities is high in otherwise an associated cervicothoracic syrinx should be seriously considered.
healthy-appearing patients with requiring surgical decompression. These patients should be followed
early onset scoliosis. In a prospec- The MRI of the third patient dis- closely at 4- to 6-month intervals,
tive study of 34 patients younger closed diffuse dural ectasia. with active treatment initiated in
than age 10 years who presented A more recent, larger study retro- the presence of >5° of Cobb angle
with curves measuring >20° and a spectively reviewed 46 patients with progression.
normal neurologic examination, a Cobb angle ≥20°, normal neuro- Traditional nonsurgical manage-
Gupta et al27 reported a 17.6% inci- logic examination, no associated ment for early onset scoliosis in-
dence of neural axis abnormalities. syndromes, and no congenital abnor- cludes casting, bracing, or a combi-
Occult abnormalities were discov- mality. The mean age at presenta- nation of both. Cast application is
ered in three of the six patients tion was 17 months (range, 2 to 37 usually done under anesthesia. The
younger than age 4 years. Two of months). Neural axis abnormality cast is changed at 6- to 12-week in-
these patients demonstrated caudal was demonstrated on MRI in 10 pa- tervals until maximum correction is
displacement of the cerebellar ton- tients (21.7%), 8 of whom required achieved. Following this, the cast
sils below the foramen magnum neurosurgical intervention. Based on may be replaced by a Milwaukee
(Chiari type I malformation), with these findings, the authors recom- brace with full-time implementa-
Volume 14, Number 2, February 2006 105
Early Onset Idiopathic Scoliosis
tion (23 h/day). The Milwaukee of the spine and inhibition of growth aged with instrumentation alone,
brace is preferred over a thoracolum- on the concave side of the curve. He whereas children age 10 years and
bar orthosis because of the rib cage recommended and performed con- older should be fused initially. Re-
distortion and pulmonary function vex spinal epiphysiodesis to address gardless of patient age, treatment
reduction reported with the circum- this imbalance. Twenty-three per- should not be considered definitive.33
ferentially fitting thoracolumbar cent of his patients showed signifi- Moe et al34 subsequently modi-
brace. In addition, the immature rib cant improvement. However, 40% fied Harrington’s technique by limit-
cage often deforms before significant were stationary or showed very little ing subperiosteal exposure to the
correction is transmitted to the improvement (<10°). area of hook placement. The hook
spine. Bracing is generally continued In a recent study reviewing long- sites were not fused. The rod itself
for a minimum of 2 years until there term results, Marks et al32 found was placed subcutaneously. Moe et
is no further evidence of progression, that convex spinal epiphysiodesis al34 also modified the Harrington rod
as indicated by an unchanging Cobb with or without Harrington instru- to have a smooth, thicker central
angle and RVAD. mentation did not significantly re- portion to prevent scar adhesion to
Mehta and Morel22 studied 21 pa- verse the established deformity. threads and to allow sagittal con-
tients with infantile idiopathic scoli- Thirteen patients with infantile id- touring. Patients were placed in a
osis who were treated nonsurgically. iopathic scoliosis were treated with Milwaukee brace postoperatively;
They reported that with total correc- anterior and posterior convex epi- the construct was lengthened when
tion before the prepubertal growth physiodesis alone (four received Har- >10° loss of correction occurred.
spurt, there is no relapse during ad- rington instrumentation 2 to 4 years There was an average increase of
olescence. Without full correction, later); a further nine patients were 2.9 cm in the length of the instru-
however, small relapses may occur. treated with convex epiphysiodesis mented portion for all 20 patients
These patients may require surgical and concurrent Harrington instru- and of 3.8 cm (compared with a pre-
intervention if further progression mentation. Radiographic progres- dicted growth of 4.5 cm) in the 9 pa-
occurs during the adolescent growth sion, mirrored by a deteriorating tients who went on to fusion. Nota-
spurt. They should be followed until clinical result, occurred in all but ble decrease in curve magnitude was
skeletal maturity. one patient. The best results were reported in the two patients with
noted with epiphysiodesis and si- progressive early onset curves. Com-
Surgical multaneous Harrington instrumen- plications occurred in 50% of pa-
Fusion tation placement, which controlled tients. Rod breakage, although less
Several surgical procedures have but did not improve the degree of the common with the modified thicker
been used to manage progressive primary curve. rod, still occurred. The authors also
curves in skeletally immature pa- reported hook dislodgement from
tients. Early procedures focused on Single Rod Instrumentation the rod and dislocation from the
slowing or halting curve progression Instrumentation without arthro- lamina.
with spinal fusion, with the ratio- desis has been performed in an at- Klemme et al35 in 1997 reported
nale that a short, straight spine was tempt to preserve spinal growth, ob- the results of a 20-year experience
preferable to a long, crooked one. tain initial scoliosis correction, and with the Moe technique. An average
Continued anterior growth follow- control ongoing deformity. Har- of 6.1 procedures were performed
ing posterior fusion alone, known as rington33 first reported this tech- from initial instrumentation to de-
the crankshaft phenomenon,30 ne- nique in 27 idiopathic and post-polio finitive fusion in 67 patients. In 44 of
cessitates circumferential fusion in patients in 1962. Using a subperi- the 67 patients, curve progression
preadolescents. Although effective osteal approach, Harrington placed was arrested or improved over the
in halting curve progression, this ap- on the curve concavity a single dis- course of treatment, with an aver-
proach prevents future spinal growth traction rod connected to hooks at age curve reduction of 30%. In the
and has deleterious effects on the de- the upper and lower end vertebrae. remaining 23 patients, including
veloping thorax and lungs. These patients were a subset of the 12 with neuromuscular scoliosis,
The effectiveness of hemiepi- 129 patients he initially treated with curves progressed an average of 33%.
physiodesis in correcting lower ex- his implant. No longitudinal results The overall growth rate of instru-
tremity axial malalignment led to were reported. Complications in- mented but unfused spinal segments
the application of this technique to cluded hook dislocation and rod was 0.08 cm per segment per year.
the growing spine. In 1963, Roaf31 breakage. Based on this early experi- Implant-related problems, including
proposed that the spinal deformity ence, Harrington believed that chil- hook dislocation and rod breakage,
was produced by growth asymmetry, dren younger than age 10 years with were reported in 33 of 402 proce-
with overgrowth on the convex side progressive scoliosis could be man- dures (8%).
106 Journal of the American Academy of Orthopaedic Surgeons
Bruce L. Gillingham, MD, CAPT, MC, USN, et al
Marchetti and Faldini36 in 1978 re- mentation with and without convex cations of single rod distraction
ported on what they termed the “end epiphysiodesis in 26 patients. Curve techniques, Akbarnia and Marks44
fusion technique.” Fourteen patients deterioration was observed in all eight developed a dual growing rod tech-
underwent staged procedures in patients treated with the Luque trol- nique, building on concepts formu-
which the vertebrae at each end of the ley alone. In curves managed with lated by Asher.45 We currently prefer
curve were initially fused. Five to 6 combined convex epiphysiodesis and this technique. Subperiosteal dissec-
months later, hook placement was Luque instrumentation, the Cobb an- tion is limited to upper and lower
performed along with subperiosteal gle worsened in 7 of 13 patients, was anchor sites (foundations) (Figure 5).
rod placement. Finally, at a third pro- unchanged in 4, and improved in 2. Hooks or screws are placed on both
cedure 6 to 8 weeks later, the upper Growth of the instrumented spinal sides of the spine in so-called claw
hook was distracted. Serial lengthen- segment was 49% of the curve pre- patterns over two to three spinal lev-
ing was performed until definitive fu- dicted in patients treated with the els to avoid hook crowding. Pedicle
sion at maturity. Four of the 14 pa- Luque trolley alone, and 32% of the screws seem to add stability to the
tients had completed treatment at the curve predicted in patients undergo- construct.46 A transverse rod con-
time of publication of their report, ing the combined procedure. nector is positioned adjacent to or in
with “most satisfactory” results. More recently, Blakemore et al43 the middle of the claw constructs at
In 1977, Luque and Cardoso37 re- reported periodic lengthening with a both foundations. Foundation sites
ported on their technique for segmen- submuscular rod with and without may be fused with local bone graft
tal spinal instrumentation (SSI) with- limited apical fusion in 29 children supplemented with synthetic graft.
out arthrodesis. In 1982, Luque38 with scoliosis. Ten of the curves Upper and lower contoured 3/16-
reported the results of adding sublam- were idiopathic. The single rod was inch-diameter rods are placed subcu-
inar wiring to a Harrington rod in 47 placed within the muscle above the taneously on both sides of the spine.
paralytic patients. The immobilized spinal periosteum. This approach The rods are joined on each side with
area grew an average of 4.6 cm, with placed the rod closer to the spine for extended tandem connectors placed
curve correction of 78%. Smooth, better contour and alignment with- at the thoracolumbar junction to
L-shaped rods were subsequently sub- out causing spontaneous posterior avoid disturbing sagittal balance.44
stituted for the Harrington rod in a fusion. Apical fusion was performed Lengthening is performed with a
construct that became known as the in curves >70° and in those that were distractor designed to fit within the
Luque trolley. Initial enthusiasm stiff on side bending radiographs. All longitudinal openings in the tandem
based on these perceived advantages patients were placed in a Milwaukee connector. The intent of initial
was tempered by reports that the sub- brace postoperatively. Curves im- lengthening during implant inser-
periosteal exposure and sublaminar proved from a mean preoperative tion is to achieve modest correction
wire passage created scar tissue and Cobb angle of 66° to a mean of 38° of the scoliotic curve without plac-
weakened the lamina, which made on initial postoperative radiographs. ing undue stress on the foundations.
revision and later definitive fusion Slight deterioration to a mean of 47° More aggressive correction is at-
difficult. In addition, premature spon- was observed on the most recent ra- tempted at the first lengthening after
taneous fusion was noted in several diographs. Spinal growth had not fusion of the foundation sites. Serial
patients. In subsequent reports by been calculated for the entire group lengthening occurs at approximately
other authors, growth preservation at the time of publication. Compli- 6-month intervals. Somatosensory
was demonstrated to be substantially cations occurred in 24%, including evoked potential monitoring is per-
less than expected.39,40 five hook displacements, three rod formed during each lengthening,
Patterson et al41 combined SSI breakages, and one superficial infec- which is generally done as an outpa-
with anterior apical convex growth tion. The authors concluded that, tient surgery. Bracing is performed
arrest and fusion in 9 of 13 patients despite the frequent but manageable until the foundation sites are fused.
who had previously undergone sur- complications, their technique is Encouraging results were ob-
gery at an average age of 5 years 5 useful for managing severe spinal de- tained from a multicenter study at
months. At 2-year follow-up, curve formities in young children who minimum 2-year follow-up (range,
correction averaged 46%. Patients have failed, or who have a contrain- 24 to 111 months) of 23 patients, in-
with anterior apical growth arrest dication to, orthotic management. cluding 7 with early onset idiopath-
combined with SSI without fusion ic curves.47 The average age at initial
had less curve deterioration than did Emerging Techniques surgery was 5 years 5 months; pa-
those who had SSI alone. No sponta- Dual Growing Rod tients had an average of 6.6 length-
neous fusions were reported. Instrumentation enings. The mean Cobb angle im-
Pratt et al42 performed a retrospec- Dissatisfied with the unpredict- proved from 82° to 38° following the
tive analysis of Luque trolley instru- ability and implant-related compli- initial surgery; it was 36° at the lat-
Volume 14, Number 2, February 2006 107
Early Onset Idiopathic Scoliosis
Figure 5 in 28 patients followed through de-
finitive surgery. Five patients had
single rod with anterior and posteri-
or apical fusion, 16 had single rod
Upper
without apical fusion, and 7 had dual
foundation rod without fusion. The mean Cobb
angle respectively improved from
85° to 65°, 61° to 39°, and 92° to 26°.
Spinal growth respectively was 0.3,
1.0, and 1.7 cm per year. The authors
concluded that growing rod tech-
niques using single or dual rods are
effective in establishing and main-
Extended taining curve correction and allow-
tandem ing spinal growth. On the basis of its
connectors
greater strength and more frequent
Extended
tandem
lengthening, however, dual rod in-
connectors strumentation produced better ini-
tial correction and maintenance of
correction and allowed more growth
than did single rod instrumentation.
Lower Although the numbers were small,
foundation the least favorable outcomes were in
patients who underwent short apical
fusion. This technique appeared to
lead to stiffening of the curve, crank-
A B
shaft phenomenon, less correction,
and a higher incidence of complica-
Dual growing rod instrumentation. A, Anteroposterior view. The upper and lower tions. The authors indicated that
rods are joined at the thoracolumbar junction by extended tandem connectors. apical fusion may not be helpful.49
B, Lateral view. The rods are contoured to maintain sagittal alignment. Extended
tandem connectors are placed at the thoracolumbar junction to minimize adverse Other Emerging
effects on thoracic kyphosis and lumbar lordosis. (Reproduced with permission Techniques
from Bagheri R, Akbarnia BA: Pediatric ISOLA [DePuy Spine] instrumentation, in Although still evolving, current
Kim DH, Vaccaro AR, Fessler RG [eds]: Spinal Instrumentation: Surgical surgical techniques using instru-
Techniques. New York, NY: Thieme, 2005, pp 636-643.) mentation with minimal or no ar-
throdesis in the treatment of early
est follow-up. Growth of the T1-S1 displacements, two rod breakages, onset idiopathic scoliosis are capable
segment averaged 1.21 cm per year. two deep wound infections, four of significant initial curve correction
The seven patients who completed superficial wound problems, one and prevention of subsequent curve
treatment at an average age of 10 crankshaft, and one junctional ky- decompensation. This allows defin-
years 3 months achieved a total T1- phosis requiring an extension of in- itive fusion to be delayed until ado-
S1 length increase of 11.8 cm from strumentation. lescence. In addition, it is possible to
preoperative status to postoperative These results indicate that the preserve nearly normal growth
final fusion (1.66 cm growth per dual rod technique is safe and effec- within the area of instrumentation.
year). In 14 patients with thoracic tive and provides increased implant It is hoped that growing rod instru-
curves, the space available for lung stability. Although the complication mentation may be removed at matu-
ratio, as described by Campbell et rate is high, this procedure has few- rity in some patients, avoiding fu-
al,48 improved from 0.87 preopera- er complications compared with sin- sion completely and preserving
tively to normal (1.00) at latest gle rod systems (Figures 6 and 7). A spinal motion. The search continues,
follow-up or after final fusion.47 recent study by Thompson et al49 of- however, for methods that will
Complications occurred in 11 of 23 fers additional support for the use of achieve curve correction and prevent
patients between initial surgery and the dual growing rod technique. The subsequent curve decompensation in
final fusion. The complications in- authors compared the results of sin- a less invasive fashion and minimize
cluded three anchor (hook or screw) gle and dual growing rod techniques the need for repeat surgical proce-
108 Journal of the American Academy of Orthopaedic Surgeons
Bruce L. Gillingham, MD, CAPT, MC, USN, et al
Figure 6
Radiographs and photographs of a girl aged 5 years 10 months old with infantile idiopathic scoliosis who was followed for 7
years and eventually had final fusion. Preoperative anteroposterior (A) and lateral (B) radiographs of the spine. Anteroposterior
(C) and lateral (D) radiographs taken after the initial surgery. Anteroposterior (E) and lateral (F) radiographs taken 5 years after
initial surgery. G and H, Clinical appearance at 5-year follow-up. Note the correction of scoliotic curve and the linear scar (G).
Patient kyphosis fell within normal limits (~50°) at the time of radiographs and clinical photographs.
Volume 14, Number 2, February 2006 109
Early Onset Idiopathic Scoliosis
Figure 7 and deeper understanding of the cen-
tral role that the spine plays in the
architecture and function of the
chest wall and thorax. This new
awareness emphasizes the impor-
tance of evaluating thoracic volume
in addition to the standard assess-
ment of anteroposterior and sagittal
spinal alignment. Restoring this
“fourth dimension,” thereby maxi-
mizing the potential for pulmonary
development, is emerging as an im-
portant goal in the treatment of pa-
tients with congenital spine and rib
anomalies or with thoracic insuffi-
ciency syndrome.48
Summary
Treating progressive early onset idio-
pathic scoliosis is challenging. Un-
treated curves may cause significant
disturbance of normal trunk and
spine growth, with severely deleteri-
Graphic representation of the improvement in length of implant, T1-S1 length, and
ous effects on the cardiopulmonary
Cobb angle magnitude in the patient shown in Figure 6. 5 + 10 = 5 years 10
months; 13 + 6 = 13 years 6 months. system. Surgical treatment is indi-
cated in patients whose curves
progress despite nonsurgical treat-
dures. The ideal implant would re- failures, in part because of loss of sta- ment. Spinal fusion at an early age
quire minimally invasive insertion; ple fixation.51 Improved staple designs also may lead to a shorter trunk, a
would be durable, rarely requiring re- promise better fixation, however. smaller thorax, and resultant pulmo-
vision or replacement; would have a Betz et al51 recently reviewed 21 nary complications. Other tech-
minimal effect on adjacent tissue; patients with adolescent idiopathic niques, such as hemiepiphysiodesis,
and, if required, would be easily in- scoliosis who were treated with ver- single growing rod methods, and SSI,
corporated into the definitive fusion. tebral body stapling. No patients have yielded satisfactory results in
One intriguing possibility is the with either infantile or juvenile scoli- this patient population. New, more
development of an implant that can osis were included. Six of 10 patients effective techniques, such as the dual
be lengthened by remote control. In with curves between 28° and 40° re- growing rod technique, anterior non-
1998, Takaso et al50 reported on the mained stable or improved at 1-year fusion techniques, and the vertically
development of a rod containing a follow-up. Four patients progressed. expandable prosthetic titanium rib,
direct-current motor attached to a Further investigation is needed to de- have emerged with the goal of pre-
radio-controlled receiver. Successful termine the efficacy of this technique serving spinal growth and maintain-
serial correction of experimental in early onset scoliosis. ing scoliosis correction. Even though
scoliosis was achieved in beagles. The technique of expansion tho- they often require the patient to un-
The main problems encountered racoplasty for managing thoracic in- dergo multiple operations through-
were the relatively large size of the sufficiency syndrome with the verti- out childhood, these techniques
rod (16 mm) and the receiver, which cally expandable prosthetic titanium promise to be less invasive in the fu-
necessitated placement in the ab- rib has recently been described.48,52 ture and more valuable in treating pa-
dominal cavity. This device was designed to manage tients with early onset scoliosis.
Recently, interest has returned to thoracic deformities resulting from
attempts at modulating the growth of absent and fused ribs in congenital
Acknowledgment
the scoliotic spine with anterior and syndromic conditions, such as
asymmetric growth arrest performed Jeune’s asphyxiating thoracic dystro- The authors wish to acknowledge
with staples placed endoscopically. phy and Jarcho-Levin syndrome. Sarah Canale, BS, for her assistance
Historically, this technique had some This effort has resulted in a broader with the editorial process.
110 Journal of the American Academy of Orthopaedic Surgeons
Bruce L. Gillingham, MD, CAPT, MC, USN, et al
References sudden infant death syndrome (SIDS) nosis. J Bone Joint Surg Br 1972;54:
in the United States: Joint commen- 648-655.
Evidence-based Medicine: Evidence- tary from the American Academy of 27. Gupta P, Lenke LG, Bridwell KH: In-
based studies are identified in Ak- Pediatrics and selected agencies of the cidence of neural axis abnormalities
barnia et al (reference 47, a multi- Federal Government. Pediatrics in infantile and juvenile patients with
1994;93:820. spinal deformity: Is a magnetic reso-
center study on dual growing rods)
14. Mehta MH: The rib-vertebra angle in nance image screening necessary?
and Thompson et al (reference 49, a the early diagnosis between resolving Spine 1998;23:206-210.
comparison of single and dual grow- and progressive infantile scoliosis. 28. Dobbs MB, Lenke LG, Szymanski DA,
ing rod techniques). J Bone Joint Surg Br 1972;54:230-243. et al: Prevalence of neural axis abnor-
15. Muirhead A, Conner AN: The assess- malities in patients with infantile id-
Citation numbers printed in bold ment of lung function in children iopathic scoliosis. J Bone Joint Surg
type indicate references published with scoliosis. J Bone Joint Surg Br Am 2002;84:2230-2234.
within the past 5 years. 1985;67:699-702. 29. Diedrich O, von Strempel A, Schloz
16. Davies G, Reid L: Effect of scoliosis on M, Schmitt O, Kraft CN: Long-term
1. James JI, Lloyd-Roberts GC, Pilcher growth of alveoli and pulmonary ar- observation and management of re-
MF: Infantile structural scoliosis. teries and on right ventricle. Arch solving infantile idiopathic scoliosis:
J Bone Joint Surg Br 1959;41:719-735. Dis Child 1971;46:623-632. A 25-year follow-up. J Bone Joint
2. James JI: Idiopathic scoliosis: The 17. Branthwaite MA: Cardiorespiratory Surg Br 2002;84:1030-1035.
prognosis, diagnosis, and operative in- consequences of unfused idiopathic 30. Dubousset J, Herring JA, Shufflebarg-
dications related to curve patterns scoliosis. Br J Dis Chest 1986;80:360- er H: The crankshaft phenomenon.
and the age at onset. J Bone Joint 369. J Pediatr Orthop 1989;9:541-550.
Surg Br 1954;36:36-49. 18. Kafer ER: Idiopathic scoliosis: Gas ex- 31. Roaf R: The treatment of progressive
3. Dimeglio A: Growth of the spine be- change and the age dependence of ar- scoliosis by unilateral growth-arrest.
fore age 5 years. J Pediatr Orthop B terial blood gases. J Clin Invest 1976; J Bone Joint Surg Br 1963;45:637-651.
1993;1:102-107. 58:825-833. 32. Marks DS, Iqbal MJ, Thompson AG,
4. Dickson RA: Early-onset idiopathic 19. Pehrsson K, Larsson S, Oden A, Piggott H: Convex spinal epiphysiod-
scoliosis, in Weinstein S (ed): The Pe- Nachemson A: Long-term follow-up
esis in the management of progressive
diatric Spine: Principles and Practice. of patients with untreated scoliosis: A
infantile idiopathic scoliosis. Spine
New York, NY: Raven Press, 1994, pp study of mortality, causes of death,
1996;21:1884-1888.
421-429. and symptoms. Spine 1992;17:1091-
33. Harrington PR: Treatment of scolio-
5. Dickson RA, Archer IA: Surgical 1096.
treatment of late-onset idiopathic 20. Conner AN: Developmental anoma- sis: Correction and internal fixation
thoracic scoliosis: The Leeds proce- lies and prognosis in infantile idio- by spine instrumentation. J Bone
dure. J Bone Joint Surg Br 1987;69: pathic scoliosis. J Bone Joint Surg Br Joint Surg Am 1962;44:591-610.
709-714. 1969;51:711-713. 34. Moe JH, Kharrat K, Winter RB, Cum-
6. Emery JL, Mithal A: The number of al- 21. Wynne-Davies R: Infantile idiopathic mine JL: Harrington instrumentation
veoli in the terminal respiratory unit scoliosis: Causative factors, particu- without fusion plus external orthotic
of man during late intrauterine life larly in the first six months of life. support for the treatment of difficult
and childhood. Arch Dis Child 1960; J Bone Joint Surg Br 1975;57:138-141. curvature problems in young chil-
35:544-547. 22. Mehta M, Morel G: The non-operative dren. Clin Orthop 1984;185:35-45.
7. Dunnill MS: Postnatal growth of the treatment of infantile idiopathic scoli- 35. Klemme WR, Denis F, Winter RB,
lung. Thorax 1962;17:329-333. osis, in Zorab P, Siezler D (eds): Scoli- Lonstein JW, Koop SE: Spinal instru-
8. James JI: Two curve patterns in idio- osis 1979. London, England: Academic mentation without fusion for progres-
pathic structural scoliosis. J Bone Press, 1979, pp 71-84. sive scoliosis in young children.
Joint Surg Br 1951;33:399-406. 23. Hooper G: Congenital dislocation of J Pediatr Orthop 1997;17:734-742.
9. Scott JC, Morgan TH: The natural his- the hip in infantile idiopathic scolio- 36. Marchetti P, Faldini A: “End fusions”
tory and prognosis of infantile idio- sis. J Bone Joint Surg Br 1980;62:447- in the treatment of some progressive
pathic scoliosis. J Bone Joint Surg Br 449. scoliosis in childhood or early adoles-
1955;37:400-413. 24. Zadeh HG, Sakka SA, Powell MP, Me- cence. Orthopaedic Transactions
10. Lloyd-Roberts GC, Pilcher MF: Struc- hta MH: Absent superficial abdomi- 1978;2:271.
tural idiopathic scoliosis in infancy: A nal reflexes in children with scoliosis: 37. Luque ER, Cardoso A: Treatment of
study of the natural history of 100 pa- An early indicator of syringomyelia. scoliosis without arthrodesis or exter-
tients. J Bone Joint Surg Br 1965;47: J Bone Joint Surg Br 1995;77:762-767. nal support: A preliminary report.
520-523. 25. Gollogly S, Smith JT, Campbell RM: Orthopaedic Transactions 1977;1:37.
11. Ceballos T, Ferrer-Torrelles M, Determining lung volume with three- 38. Luque ER: Paralytic scoliosis in grow-
Castillo F, Fernandez-Paredes E: Prog- dimensional reconstructions of CT ing children. Clin Orthop 1982;163:
nosis in infantile idiopathic scoliosis. scan data: A pilot study to evaluate 202-209.
J Bone Joint Surg Am 1980;62:863- the effects of expansion thoracoplasty 39. Mardjetko SM, Hammerberg KW, Lu-
875. on children with severe spinal defor- bicky JP, Fister JS: The Luque trolley
12. Mau H: Does infantile scoliosis re- mities. J Pediatr Orthop 2004;24: revisited: Review of nine cases requir-
quire treatment? J Bone Joint Surg 323-328. ing revision. Spine 1992;17:582-589.
Am 1968;50:881. 26. Ferreira JH, de Janeiro R, James JI: Pro- 40. Rinsky LA, Gamble JG, Bleck EE: Seg-
13. Kattwinkel J, Brooks J, Keenan ME, gressive and resolving infantile idio- mental instrumentation without fu-
Malloy M: Infant sleep position and pathic scoliosis: The differential diag- sion in children with progressive
Volume 14, Number 2, February 2006 111
Early Onset Idiopathic Scoliosis
scoliosis. J Pediatr Orthop 1985;5: (ed): The Textbook of Spinal Surgery. P, et al: Comparison of single and dual
687-690. Philadelphia, PA: Lippincott-Raven, growing rod techniques followed
41. Patterson JF, Webb JK, Burwell RG: 1997, pp 569-609. through definitive surgery: A prelim-
The operative treatment of progres- 46. Bagheri R, Oka R, Mahar A, Kostial P, inary study. Spine 2005;30:2039-
sive early onset scoliosis: A prelimi- Akbarnia BA: Biomechanical compar- 2044.
nary report. Spine 1990;15:809-815. ison of different anchors (foundations) 50. Takaso M, Moriya H, Kitahara H,
42. Pratt RK, Webb JK, Burwell RG, Cum- used in the growing dual rod tech- et al: New remote-controlled grow-
mings SL: Luque trolley and convex nique. IMAST 11th International ing-rod spinal instrumentation pos-
epiphysiodesis in the management of Meeting on Advanced Spine Tech- sibly applicable for scoliosis in young
infantile and juvenile idiopathic scoli- niques: Final Program. Session 9, Pa- children. J Orthop Sci 1998;3:336-
osis. Spine 1999;24:1538-1547. per 90. Milwaukee, WI: Scoliosis Re- 340.
43. Blakemore LC, Scoles PV, Poe- search Society, 2004. 51. Betz RR, Kim J, D’Andrea LP, Mulca-
Kochert C, Thompson GH: Submus- 47. Akbarnia BA, Marks DS, Boachie- hey MJ, Balsara RK, Clements DH: An
cular Isola rod with or without limit- Adjei O, Thompson A, Asher MA: innovative technique of vertebral
ed apical fusion in the management of Dual growing rod technique for the body stapling for the treatment of pa-
severe spinal deformities in young treatment of progressive early onset tients with adolescent idiopathic
children: Preliminary report. Spine scoliosis: A multicenter study. Spine scoliosis: A feasibility, safety, and
2001;26:2044-2048. 2005;30:S46-S57. utility study. Spine 2003;28:S255-
44. Akbarnia BA, Marks DS: Instrumen- 48. Campbell RM, Smith MD, Mayes TC, S265.
tation with limited arthrodesis for the et al: The characteristics of thoracic 52. Campbell RM, Smith MD, Hell-
treatment of progressive early-onset insufficiency syndrome associated Vocke AK: Expansion thoracoplasty:
scoliosis. Spine: State of the Art with fused ribs and congenital scolio- The surgical technique of opening-
Reviews 2000;14:181-189. sis. J Bone Joint Surg Am 2003;85: wedge thoracostomy. Surgical tech-
45. Asher MA: Isola spinal instrumenta- 399-408. nique. J Bone Joint Surg Am
tion system for scoliosis, in DeWald R 49. Thompson GH, Akbarnia BA, Kostial 2004;86(suppl 1):51-64.
112 Journal of the American Academy of Orthopaedic Surgeons
You might also like
- The Case of Radonda.... KeilaniDocument6 pagesThe Case of Radonda.... KeilaniTrabajos SOSNo ratings yet
- Sejarah Ortho Dunia Dan IndonesiaDocument2 pagesSejarah Ortho Dunia Dan Indonesiayudha anantha khaerul putraNo ratings yet
- Narayana HrudayalayaDocument20 pagesNarayana HrudayalayaVivek Sinha100% (1)
- Orthopedic History Taking: DR - Kholoud Al-ZainDocument30 pagesOrthopedic History Taking: DR - Kholoud Al-ZainKaizar EnnisNo ratings yet
- Neurosurg Focus Article Pe2Document9 pagesNeurosurg Focus Article Pe2Roberto CamposNo ratings yet
- Nonsurgical Management of Early-Onset ScoliosisDocument11 pagesNonsurgical Management of Early-Onset Scoliosisgoscolombia goscolombiaNo ratings yet
- Managment of ScoliosisDocument18 pagesManagment of ScoliosisCarlos Fernando Roca AkamineNo ratings yet
- Articulo#3 2007 (201) Pag 4Document3 pagesArticulo#3 2007 (201) Pag 4Sebastian LeonNo ratings yet
- ArticleDocument8 pagesArticleLusian VissNo ratings yet
- 2012 33 553 Blaise A. Nemeth and Vinay Narotam: Developmental Dysplasia of The HipDocument11 pages2012 33 553 Blaise A. Nemeth and Vinay Narotam: Developmental Dysplasia of The HipERICKNo ratings yet
- Developmental Hip Dysplasia: Case StudyDocument2 pagesDevelopmental Hip Dysplasia: Case StudyIlias ParaskevopoulosNo ratings yet
- Spinal Muscular Atrophy: Stephen J. Kolb,, John T. KisselDocument16 pagesSpinal Muscular Atrophy: Stephen J. Kolb,, John T. KisselZouhour MiladiNo ratings yet
- DSA10 Scoliosis, Posture and Muscle BalanceDocument11 pagesDSA10 Scoliosis, Posture and Muscle BalanceWilliam JonesNo ratings yet
- DDH 6-4 PDFDocument11 pagesDDH 6-4 PDFRonalCadilloNo ratings yet
- Surgical and Conservative Treatment of Patients With Congenital Scoliosis: A Search For Long-Term ResultsDocument17 pagesSurgical and Conservative Treatment of Patients With Congenital Scoliosis: A Search For Long-Term ResultsFaris Aziz PridiantoNo ratings yet
- Updateonevaluationand Treatmentofscoliosis: Ron El-Hawary,, Chukwudi ChukwunyerenwaDocument19 pagesUpdateonevaluationand Treatmentofscoliosis: Ron El-Hawary,, Chukwudi Chukwunyerenwacarla grauNo ratings yet
- Clinical Practice: The Spine From Birth To AdolescenceDocument6 pagesClinical Practice: The Spine From Birth To Adolescencechristian roblesNo ratings yet
- Adolescent Lumbar Disc Herniation:: A CaseDocument4 pagesAdolescent Lumbar Disc Herniation:: A CasefeliNo ratings yet
- Consensus Statementskaggs2015Document1 pageConsensus Statementskaggs2015Никита ХусаиновNo ratings yet
- 44 - Adult ScoliosisDocument6 pages44 - Adult ScoliosismiiiiiiiiiiiiithaNo ratings yet
- Back Pain and Scoliosis in Children When To Image, What To ConsiderDocument12 pagesBack Pain and Scoliosis in Children When To Image, What To ConsiderGiancarlo PalaciosNo ratings yet
- AJGP 12 2020 Clinical Parr Paediatric Scoliosis Update WEBDocument6 pagesAJGP 12 2020 Clinical Parr Paediatric Scoliosis Update WEBalex.ttkNo ratings yet
- Osteogenisis Imperfecta: Christopher LimDocument34 pagesOsteogenisis Imperfecta: Christopher LimRhomadhoni Ika PutraNo ratings yet
- Case Reflection 1 POD 1Document7 pagesCase Reflection 1 POD 1seankelly327No ratings yet
- Scoliosis Charper12Document122 pagesScoliosis Charper12Simón Pérez LópezNo ratings yet
- p1310 PDFDocument7 pagesp1310 PDFArya PratamaNo ratings yet
- Rol Ton 2014Document7 pagesRol Ton 2014anonNo ratings yet
- American Academy of Pediatrics: Developmental Dysplasia of The Hip Is TheDocument10 pagesAmerican Academy of Pediatrics: Developmental Dysplasia of The Hip Is Thelolamusic90No ratings yet
- Scoliosis: Review of Diagnosis and Treatment: Janusz Popko, Michał Kwiatkowski, Monika GałczykDocument5 pagesScoliosis: Review of Diagnosis and Treatment: Janusz Popko, Michał Kwiatkowski, Monika Gałczykandi dirhanNo ratings yet
- Five New Cases and Review of Nine Previously Published CasesDocument8 pagesFive New Cases and Review of Nine Previously Published CasesBogdan SoptereanNo ratings yet
- Spine 2009 MarksDocument5 pagesSpine 2009 MarksSamantha FilevNo ratings yet
- Tracy 2004Document8 pagesTracy 2004alanna07No ratings yet
- Torticollis, Facial Asymmetry and Plagiocephaly in Normal NewbornsDocument6 pagesTorticollis, Facial Asymmetry and Plagiocephaly in Normal NewbornsJuan Pablo PérezNo ratings yet
- Aaos Pediatric 2020Document57 pagesAaos Pediatric 2020ABUBAKER ZANBOUZINo ratings yet
- The "Epidemic" of Occipital Flattening: Why It Is Happening and What To Do About ItDocument5 pagesThe "Epidemic" of Occipital Flattening: Why It Is Happening and What To Do About ItDinner and a Donkey Show TheatreNo ratings yet
- Brachial Plexus Birth Palsy: An Overview of Early Treatment ConsiderationsDocument7 pagesBrachial Plexus Birth Palsy: An Overview of Early Treatment Considerationsphannghia.ydsNo ratings yet
- Pediatrichipandpelvis: Bertrand W. ParcellsDocument14 pagesPediatrichipandpelvis: Bertrand W. ParcellsMarlin Berliannanda TawayNo ratings yet
- Developmental Dysplasia of The HipDocument12 pagesDevelopmental Dysplasia of The HipkaremiaNo ratings yet
- Paralisis de Bell PDFDocument10 pagesParalisis de Bell PDFCarlos Andrés Barrera ParraNo ratings yet
- Pediatricspinalcordinjury: A Review by Organ SystemDocument24 pagesPediatricspinalcordinjury: A Review by Organ SystemDana DumitruNo ratings yet
- Severe Scoliosis in An Adolescent Benefits of EarlDocument7 pagesSevere Scoliosis in An Adolescent Benefits of EarlNEUROLIVROS NEUROLIVROSNo ratings yet
- Graham 2016Document25 pagesGraham 2016Constanzza Arellano LeivaNo ratings yet
- Jurnal ScoliosisDocument14 pagesJurnal ScoliosisimanuelNo ratings yet
- Adolescent Idiopathic Scoliosis - Clinical Features, Evaluation, and Diagnosis - UpToDateDocument43 pagesAdolescent Idiopathic Scoliosis - Clinical Features, Evaluation, and Diagnosis - UpToDateKiri GeorgeNo ratings yet
- Scoliosis (Curved Spine)Document7 pagesScoliosis (Curved Spine)Chow Mun FaiNo ratings yet
- P13 - Fractures of The Spine in ChildrenDocument47 pagesP13 - Fractures of The Spine in Childrenkosmynin86No ratings yet
- Positional Plagiocephaly Evaluati - 2004 - Oral and Maxillofacial Surgery CliniDocument8 pagesPositional Plagiocephaly Evaluati - 2004 - Oral and Maxillofacial Surgery Clinilaljadeff12No ratings yet
- Pectus ExcavatumDocument10 pagesPectus ExcavatumEnfermeiros Ostomia Equipe de EnfermagemNo ratings yet
- Pectus ExcavatumDocument10 pagesPectus ExcavatumEnfermeiros Ostomia Equipe de EnfermagemNo ratings yet
- SCOLIOSISDocument19 pagesSCOLIOSISEspers BluesNo ratings yet
- Sarah N. Dalrymple, MD Jessica H. Row, MD and John Gazewood, MD, MSPHDocument6 pagesSarah N. Dalrymple, MD Jessica H. Row, MD and John Gazewood, MD, MSPHKarine RodriguesNo ratings yet
- About Scoliosis PDFDocument7 pagesAbout Scoliosis PDFNiessha ZuhrotulNo ratings yet
- Management of The Spine in Cerebral PalsyDocument7 pagesManagement of The Spine in Cerebral PalsyDitaAnggaraKusumaNo ratings yet
- The Pediatric Physical Examination - HEENT - UpToDateDocument87 pagesThe Pediatric Physical Examination - HEENT - UpToDateEmily LinharesNo ratings yet
- LWBK836 Ch72 p711-720Document10 pagesLWBK836 Ch72 p711-720metasoniko81No ratings yet
- (23444959 - Romanian Neurosurgery) Shaken Baby Syndrome. Case ReportDocument9 pages(23444959 - Romanian Neurosurgery) Shaken Baby Syndrome. Case ReportRio M RajagukgukNo ratings yet
- Developmental (Congenital) Dysplasia of The HipDocument12 pagesDevelopmental (Congenital) Dysplasia of The HipFifi Chi Keluarga PrajaNo ratings yet
- Cerebral Palsy-1 PDFDocument94 pagesCerebral Palsy-1 PDFgpediatrics myNo ratings yet
- US For Glenohumeral DysplasiaDocument10 pagesUS For Glenohumeral DysplasiaTeoNo ratings yet
- Clinical Management of Krabbe Diseas Source J Neurosci Res SO 2016 Nov 94 11 1118 25 (PMIDT27638597)Document8 pagesClinical Management of Krabbe Diseas Source J Neurosci Res SO 2016 Nov 94 11 1118 25 (PMIDT27638597)dai shujuanNo ratings yet
- 5 FullDocument2 pages5 FullrahelNo ratings yet
- A Simple Guide to Klippel-Feil Syndrome, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Klippel-Feil Syndrome, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Insulin Resistance: Childhood Precursors of Adult DiseaseFrom EverandInsulin Resistance: Childhood Precursors of Adult DiseasePhilip S. ZeitlerNo ratings yet
- Metatarsalgia Besse2017Document11 pagesMetatarsalgia Besse2017suad5stambulieNo ratings yet
- Outcomes of Hip Arthroscopy in Patients Aged 50 Years or Older Compared With A Matched-Pair Control of Patients Aged 30 Years or YoungerDocument8 pagesOutcomes of Hip Arthroscopy in Patients Aged 50 Years or Older Compared With A Matched-Pair Control of Patients Aged 30 Years or Youngersuad5stambulieNo ratings yet
- Escoliosis Idiopacitca Infantilkarol2019Document6 pagesEscoliosis Idiopacitca Infantilkarol2019suad5stambulieNo ratings yet
- 2007 JBJS External Fixation How To Make It Work PDFDocument15 pages2007 JBJS External Fixation How To Make It Work PDFsuad5stambulieNo ratings yet
- Cosmotic Surgical Center Business PlanDocument37 pagesCosmotic Surgical Center Business PlanRamchandra Cv100% (1)
- Ultrasonic Surgical & Electrosurgical System: All in One Pla Orm, All With Superior PerformanceDocument2 pagesUltrasonic Surgical & Electrosurgical System: All in One Pla Orm, All With Superior PerformanceDiego DulcamareNo ratings yet
- Basic Surgical InstrumenDocument36 pagesBasic Surgical InstrumenYoga PribadiNo ratings yet
- Office Memorandum Dated 17.10Document21 pagesOffice Memorandum Dated 17.10Pradeep SaxenaNo ratings yet
- Mayo CurveDocument6 pagesMayo CurveDanielle Marie SimoraNo ratings yet
- Phaco Machine Procedure PDFDocument4 pagesPhaco Machine Procedure PDFAlim SumonNo ratings yet
- Additive Manufacturing of Custom Orthoses and Prostheses - A ReviewDocument7 pagesAdditive Manufacturing of Custom Orthoses and Prostheses - A ReviewÖzgeSevinKeskinNo ratings yet
- CranioplastyDocument2 pagesCranioplastyLaila munazadNo ratings yet
- DOC-0025 - Clinical Evaluations - Qualified Persons and Evaluators Declaration of InterestsDocument3 pagesDOC-0025 - Clinical Evaluations - Qualified Persons and Evaluators Declaration of InterestsAndrew SaxtonNo ratings yet
- Shouldice NotesDocument3 pagesShouldice NotesDisha TutejaNo ratings yet
- OTO Alex ProgDocument54 pagesOTO Alex ProgCharm MeelNo ratings yet
- Doctor On Duty Treatment Guide 2NDDocument106 pagesDoctor On Duty Treatment Guide 2NDWaleedNo ratings yet
- Bromage Motor Blockade Score - A Score That Has Lasted More Than A LifetimeDocument2 pagesBromage Motor Blockade Score - A Score That Has Lasted More Than A LifetimeGeter PairikasNo ratings yet
- Hari Waktu Acara Narasumber Fasilitator/ Pengawas Pusat Senin, 26 April 2021Document2 pagesHari Waktu Acara Narasumber Fasilitator/ Pengawas Pusat Senin, 26 April 2021Larvahmir SpDVNo ratings yet
- Electric Operating Table: Shanghai PAX Medical Instrument CO., LTDDocument4 pagesElectric Operating Table: Shanghai PAX Medical Instrument CO., LTDMeidita JuliandaNo ratings yet
- Percutaneous Pinning: Pictures 1 and 2Document3 pagesPercutaneous Pinning: Pictures 1 and 2Ishan BramhbhattNo ratings yet
- Computer Assisted Orthopaedic Surgery For Hip and Knee 2018 Sugano PDFDocument202 pagesComputer Assisted Orthopaedic Surgery For Hip and Knee 2018 Sugano PDFValdete FigueiredoNo ratings yet
- Learning Contract InternDocument3 pagesLearning Contract Internapi-344149486No ratings yet
- IDA Membership FormDocument3 pagesIDA Membership FormAbhijit LeleNo ratings yet
- Ahead,: Is What We AreDocument10 pagesAhead,: Is What We AreKothapalli ChiranjeeviNo ratings yet
- ARAR Calibration and TestingDocument4 pagesARAR Calibration and TestingAbid HussainNo ratings yet
- AOSpine Thoracolumbar Classification System - Poster PDFDocument1 pageAOSpine Thoracolumbar Classification System - Poster PDFmhmiguelNo ratings yet
- Endoscopy PaperDocument2 pagesEndoscopy Paperapi-543734210No ratings yet
- Casting 8-1Document54 pagesCasting 8-1damaris seberioNo ratings yet
- Two Novel Clinical Tests For The Diagnosis of Hip Labral TearsDocument8 pagesTwo Novel Clinical Tests For The Diagnosis of Hip Labral TearsmontseNo ratings yet
- Closed Reduction in Distal Radius FractureDocument4 pagesClosed Reduction in Distal Radius FractureAdhitya IndraNo ratings yet