You might also like
- Ancient Skies of Northern Europe: Stars, Constellations, and The Moon in Nordic MythologyDocument12 pagesAncient Skies of Northern Europe: Stars, Constellations, and The Moon in Nordic MythologyoldenglishblogNo ratings yet
- CT Angiography of The Lower Extremities The Peripheral Vascular System Presents Unique Imaging ChallengesDocument7 pagesCT Angiography of The Lower Extremities The Peripheral Vascular System Presents Unique Imaging ChallengesDavid Puyó100% (1)
- Heat Sink Capacity Mesurment in Inservice PipelineDocument13 pagesHeat Sink Capacity Mesurment in Inservice PipelineSomeshNo ratings yet
- 5276Document52 pages5276Sean PorterNo ratings yet
- Standard Welding Procedure SpecificationsDocument2 pagesStandard Welding Procedure SpecificationsAnonymous dh6DITNo ratings yet
- CardiomyopathyDocument1 pageCardiomyopathyTrisha VergaraNo ratings yet
- Stresses in Large Horizontal Cylindrical Pressure Vessels On Two Saddle Supports - Zick (1951) OriginalDocument11 pagesStresses in Large Horizontal Cylindrical Pressure Vessels On Two Saddle Supports - Zick (1951) OriginalBryan Pérez PérezNo ratings yet
- The Word Became Flesh An Exploratory Essay On Jesu 003Document62 pagesThe Word Became Flesh An Exploratory Essay On Jesu 003Alexios VrionisNo ratings yet
- Thoracoabdominal Aortic Aneurysms Open RepairDocument13 pagesThoracoabdominal Aortic Aneurysms Open RepairJonathan Frimpong AnsahNo ratings yet
- Et0420 MedAffairs MouawadDocument5 pagesEt0420 MedAffairs MouawadAna Silvia LebrOnNo ratings yet
- Carotid Endarterectomy: Experience in 8743 Cases.Document13 pagesCarotid Endarterectomy: Experience in 8743 Cases.Alexandre Campos Moraes AmatoNo ratings yet
- CT Support of Cardiac Structural Interventions: Review ArticleDocument12 pagesCT Support of Cardiac Structural Interventions: Review ArticlefibiaNo ratings yet
- Lemus Rangel 2010Document2 pagesLemus Rangel 2010audiNo ratings yet
- Percutaneous Transluminal Angioplasty and Stenting As First-Choice Treatment in Patients With Chronic Mesenteric IschemiaDocument6 pagesPercutaneous Transluminal Angioplasty and Stenting As First-Choice Treatment in Patients With Chronic Mesenteric IschemiaCotaga IgorNo ratings yet
- CT Angiography in Vertebral Artery DissectionDocument6 pagesCT Angiography in Vertebral Artery DissectionDaniel AraujoNo ratings yet
- Video-Atlas of Open Thoracoabdominal Aortic Aneurysm RepairDocument6 pagesVideo-Atlas of Open Thoracoabdominal Aortic Aneurysm Repairvan le hoangNo ratings yet
- Video-Atlas of Open Thoracoabdominal Aortic Aneurysm RepairDocument6 pagesVideo-Atlas of Open Thoracoabdominal Aortic Aneurysm Repairvan le hoangNo ratings yet
- CT Angiography Versus Digital Subtraction Angiography For Intracranial Vascular Pathology in A Clinical SettingDocument9 pagesCT Angiography Versus Digital Subtraction Angiography For Intracranial Vascular Pathology in A Clinical SettingPari Pengda BaliNo ratings yet
- Retrolaparoscopic Adrenalectomy Assisted by Three-Dimensional Reconstructed Digital Model in A Patient With Situs Inversus TotalisDocument5 pagesRetrolaparoscopic Adrenalectomy Assisted by Three-Dimensional Reconstructed Digital Model in A Patient With Situs Inversus Totalisyerich septaNo ratings yet
- Clarivein - Early Results From A Large Single-Centre Series of Mechanochemical Endovenous Ablation For Varicose VeinsDocument7 pagesClarivein - Early Results From A Large Single-Centre Series of Mechanochemical Endovenous Ablation For Varicose VeinsronnyNo ratings yet
- Art 02Document8 pagesArt 02Paula Milla TorresNo ratings yet
- Imagingofacutestroke: Current StateDocument9 pagesImagingofacutestroke: Current Statealejandro echeverriNo ratings yet
- Duarte Junior 2021Document11 pagesDuarte Junior 2021fumblefumbleNo ratings yet
- Hybrid Repair of Aortic Arch AneurysmDocument8 pagesHybrid Repair of Aortic Arch AneurysmFrancesca MazzolaniNo ratings yet
- Interdisciplinary Neurosurgery: Advanced Techniques and Case ManagementDocument16 pagesInterdisciplinary Neurosurgery: Advanced Techniques and Case ManagementEvelyn JudithNo ratings yet
- 1 s2.0 S1875213618300913 MainDocument10 pages1 s2.0 S1875213618300913 MainSara TeixeiraNo ratings yet
- Recanalizacion EndovascularDocument8 pagesRecanalizacion Endovascularjuan perezNo ratings yet
- Rolf2013 Article PreproceduralCoronaryCTAngiogrDocument9 pagesRolf2013 Article PreproceduralCoronaryCTAngiogrرقية ياسينNo ratings yet
- Management of 219 Consecutive Cases of Postcatheterization PseudoaneurysmDocument6 pagesManagement of 219 Consecutive Cases of Postcatheterization PseudoaneurysmdrelvNo ratings yet
- Art:10.1007/s11517 014 1165 7Document8 pagesArt:10.1007/s11517 014 1165 7Mustafa A. ElattarNo ratings yet
- Review Article: Computed Tomography in The Evaluation For Transcatheter Aortic Valve Implantation (TAVI)Document13 pagesReview Article: Computed Tomography in The Evaluation For Transcatheter Aortic Valve Implantation (TAVI)Paul SchoenhagenNo ratings yet
- 10 1 1 525 6842Document6 pages10 1 1 525 6842sandyNo ratings yet
- Tratamiento Endovascular de La Disección Aórtica Tipo B Mediante EndoprótesisDocument8 pagesTratamiento Endovascular de La Disección Aórtica Tipo B Mediante EndoprótesisNicki CondezaNo ratings yet
- New England Journal Medicine: The ofDocument11 pagesNew England Journal Medicine: The ofahmadto80No ratings yet
- Presentation 3Document47 pagesPresentation 3NAGESH RAJNo ratings yet
- Articles by Dr. Nata ParnesDocument19 pagesArticles by Dr. Nata ParnesWatertown Daily TimesNo ratings yet
- Bush2015 1 PDFDocument15 pagesBush2015 1 PDFMoukhtar MahdyNo ratings yet
- Khairy 2017Document7 pagesKhairy 2017Beby Dwi Lestari BajryNo ratings yet
- (19330693 - Journal of Neurosurgery) MRI-guided Stereotactic Laser Corpus Callosotomy For Epilepsy: Distinct Methods and OutcomesDocument13 pages(19330693 - Journal of Neurosurgery) MRI-guided Stereotactic Laser Corpus Callosotomy For Epilepsy: Distinct Methods and Outcomeswafaa moNo ratings yet
- Ctangiographyincomplexupperextremity Reconstruction: Keywords: CT Angiography, Upper Extremity ReconstructionDocument5 pagesCtangiographyincomplexupperextremity Reconstruction: Keywords: CT Angiography, Upper Extremity ReconstructionIrinel BuscaNo ratings yet
- Cost-Effectiveness Analysis of The SAPIEN 3 Transcatheter Aortic Valve Implant in Patients With Symptomatic Severe Aortic StenosisDocument9 pagesCost-Effectiveness Analysis of The SAPIEN 3 Transcatheter Aortic Valve Implant in Patients With Symptomatic Severe Aortic StenosisGaal PinNo ratings yet
- JR Integrasi InvasiveDocument72 pagesJR Integrasi InvasiveRian AprizaNo ratings yet
- SMJ 60 247Document6 pagesSMJ 60 247Chee Yung NgNo ratings yet
- Goyal Et Al-2015-Annals of NeurologyDocument7 pagesGoyal Et Al-2015-Annals of NeurologyWinda Wahyu IkaputriNo ratings yet
- Terapia de Resincronización en Pacientes Con Insuficiencia Cardiaca Experiencia Acumulada de 10 AñosDocument9 pagesTerapia de Resincronización en Pacientes Con Insuficiencia Cardiaca Experiencia Acumulada de 10 AñosKevin Alegre AguileraNo ratings yet
- Parameter CTDocument8 pagesParameter CTI Putu GedeNo ratings yet
- Mitral Valve Annular Downsizing Forces: Implications For Annuloplasty Device DevelopmentDocument8 pagesMitral Valve Annular Downsizing Forces: Implications For Annuloplasty Device Developmentdiana25No ratings yet
- Modelo 2Document5 pagesModelo 2kodagaNo ratings yet
- Langen&formatpdfDocument6 pagesLangen&formatpdftameemNo ratings yet
- Clinical Neurology and NeurosurgeryDocument5 pagesClinical Neurology and NeurosurgeryRina NovitrianiNo ratings yet
- 405 2013 Article 2598Document5 pages405 2013 Article 2598M Shiddiq GhiffariNo ratings yet
- Imaging, Intervention, and Work Ow in Acute Ischemic Stroke: The Calgary ApproachDocument7 pagesImaging, Intervention, and Work Ow in Acute Ischemic Stroke: The Calgary ApproachwidyadariNo ratings yet
- (10920684 - Neurosurgical Focus) Falcotentorial Meningiomas - Clinical, Neuroimaging, and Surgical Features in Six PatientsDocument7 pages(10920684 - Neurosurgical Focus) Falcotentorial Meningiomas - Clinical, Neuroimaging, and Surgical Features in Six PatientsPutri PrameswariNo ratings yet
- 701 2022 Article 5445Document9 pages701 2022 Article 5445PeyepeyeNo ratings yet
- Anderson 2016Document2 pagesAnderson 2016Pallavi SutarNo ratings yet
- CT Angiography ThesisDocument7 pagesCT Angiography ThesisHelpWritingPapersSingapore100% (3)
- Quantification Asynchhrony Last REv 03 2008 Reordenando AntDocument20 pagesQuantification Asynchhrony Last REv 03 2008 Reordenando AntEtel SilvaNo ratings yet
- Endoscopic Treatment of Choanal Atresia and Use of Balloon Dilation: Our ExperienceDocument6 pagesEndoscopic Treatment of Choanal Atresia and Use of Balloon Dilation: Our Experiencefarah maulida martaNo ratings yet
- Endovenous Microwave Ablation of Great Saphenous VeinDocument3 pagesEndovenous Microwave Ablation of Great Saphenous VeinMalekseuofi مالك السيوفيNo ratings yet
- Doble ArcoDocument19 pagesDoble ArcoCorazon MabelNo ratings yet
- A-Line Complication PDFDocument8 pagesA-Line Complication PDFaeagesNo ratings yet
- Value of Repeated Imaging in Patients With A Stroke Who Are Transferred For Endovascular TreatmentDocument5 pagesValue of Repeated Imaging in Patients With A Stroke Who Are Transferred For Endovascular TreatmentRafika Ayu NadiaNo ratings yet
- Atlas of 3D Transesophageal Echocardiography in Structural Heart Disease Interventions: Cases and VideosFrom EverandAtlas of 3D Transesophageal Echocardiography in Structural Heart Disease Interventions: Cases and VideosNo ratings yet
- Accepted Manuscript: Cardiovascular Revascularization MedicineDocument19 pagesAccepted Manuscript: Cardiovascular Revascularization MedicineNasriNo ratings yet
- Original ArticleDocument9 pagesOriginal ArticleJason HuangNo ratings yet
- Acs 04 05 422Document6 pagesAcs 04 05 422Enrico SquiccimarroNo ratings yet
- Atlas of Coronary Intravascular Optical Coherence TomographyFrom EverandAtlas of Coronary Intravascular Optical Coherence TomographyNo ratings yet
- DSP Lab RecordDocument97 pagesDSP Lab RecordLikhita UttamNo ratings yet
- Riparian Flora of Kaliwa River Watershed in The Sierra Madre Mountain Range, PhilippinesDocument12 pagesRiparian Flora of Kaliwa River Watershed in The Sierra Madre Mountain Range, PhilippinesMichael Angelo ValdezNo ratings yet
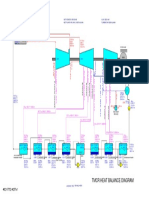
- 01 TMCR Heat Balance DiagramDocument1 page01 TMCR Heat Balance DiagramPrescila PalacioNo ratings yet
- Thin Film DepositionDocument34 pagesThin Film Depositionsenthil100% (2)
- Falsework For Concrete Structures - Guidelines: Indian StandardDocument24 pagesFalsework For Concrete Structures - Guidelines: Indian StandardLivinston JosephNo ratings yet
- Laying Out Compoud Curve and Reverse by Deflection Angle MethodDocument10 pagesLaying Out Compoud Curve and Reverse by Deflection Angle MethodEljenColanggo0% (2)
- Reglas Digitales Mitutoyo Scale Units Linear ScalesDocument31 pagesReglas Digitales Mitutoyo Scale Units Linear ScalesAngelmambrinNo ratings yet
- Mechanics of Solids - (Riveted and Welded Joints)Document37 pagesMechanics of Solids - (Riveted and Welded Joints)TusherNo ratings yet
- Ix T7AM-CAN - Beijer ElectronicsDocument1 pageIx T7AM-CAN - Beijer ElectronicsKen VikstromNo ratings yet
- cs229.... Machine Language. Andrew NGDocument17 pagescs229.... Machine Language. Andrew NGkrishnaNo ratings yet
- Berkeley To San JoseDocument88 pagesBerkeley To San JoseTimothy HightowerNo ratings yet
- A 388 - A 388M - 03 - Qtm4oc9bmzg4tqDocument8 pagesA 388 - A 388M - 03 - Qtm4oc9bmzg4tqRod RoperNo ratings yet
- Meat PieDocument13 pagesMeat Piecrispitty100% (1)
- A Proposal Study On The Construction of An Automated People Mover APM Inside The New Manila International Airport NMIADocument78 pagesA Proposal Study On The Construction of An Automated People Mover APM Inside The New Manila International Airport NMIAMckyle FaustinoNo ratings yet
- ER2 Manual 125kg 5t - 04Document144 pagesER2 Manual 125kg 5t - 04Muhammed ShamseerNo ratings yet
- EmpathyDocument5 pagesEmpathyHijaab KhaanNo ratings yet
- In-Lab Sharp-Edged Orifice Meter ReportDocument9 pagesIn-Lab Sharp-Edged Orifice Meter ReportLiliane AlameddineNo ratings yet
- Cytokines and Interferons Types and FunctionsDocument25 pagesCytokines and Interferons Types and FunctionsSereen Abd El-rahmanNo ratings yet
- Bastidas Et Al, 2010Document8 pagesBastidas Et Al, 2010Panji Satria N.No ratings yet
- BotanyDocument11 pagesBotanyGirish GuptaNo ratings yet
- Random Processes: Saravanan Vijayakumaran Sarva@ee - Iitb.ac - inDocument10 pagesRandom Processes: Saravanan Vijayakumaran Sarva@ee - Iitb.ac - inSonu kumarNo ratings yet
- Lecture-I Introduction To Concrete TechnologyDocument102 pagesLecture-I Introduction To Concrete Technologyjs kalyana rama100% (4)
- Extravagant - Bethel Music CHORDS PDFDocument2 pagesExtravagant - Bethel Music CHORDS PDFKamila Joseph Hernandez VanegasNo ratings yet