You might also like
- UvpDocument43 pagesUvpgaasheNo ratings yet
- Pelvic Organ ProlapsDocument46 pagesPelvic Organ ProlapsMuthiah nurul IzzahNo ratings yet
- Kleitsch 1958Document6 pagesKleitsch 1958CojocariNo ratings yet
- Genital ProlapseDocument90 pagesGenital ProlapseKilp MosesNo ratings yet
- Pelvic Organ Prolapse: Cheryl B. Iglesia, MD, and Katelyn R. Smithling, MDDocument7 pagesPelvic Organ Prolapse: Cheryl B. Iglesia, MD, and Katelyn R. Smithling, MDpatrick chanyaNo ratings yet
- What S New in The Functional Anatomy of Pelvic Organ ProlapseDocument18 pagesWhat S New in The Functional Anatomy of Pelvic Organ ProlapseNicol Campos HernándezNo ratings yet
- Groin AnatomyDocument7 pagesGroin AnatomyLorenzo Daniel AntonioNo ratings yet
- Utero-Vaginal Prolapse: BY: Muhammad Anwar Ridzwan Bin Abd HarisDocument47 pagesUtero-Vaginal Prolapse: BY: Muhammad Anwar Ridzwan Bin Abd HarisHizami NorddinNo ratings yet
- OB Chap 22 - Normal LaborDocument4 pagesOB Chap 22 - Normal LaborChino Paolo SamsonNo ratings yet
- Pelvic Organ ProlapseDocument5 pagesPelvic Organ Prolapsecgao30No ratings yet
- HerniaDocument100 pagesHerniaangelaanapaku100% (3)
- Hernia AnakDocument31 pagesHernia AnakHerry SukmawardiNo ratings yet
- 556 - Breechwilliams Obstetrics 25th Edition (2018)Document12 pages556 - Breechwilliams Obstetrics 25th Edition (2018)yayayanizaNo ratings yet
- Pediatric HerniasDocument19 pagesPediatric HerniasAndria SaputraNo ratings yet
- Imperforate Anus and Cloacal MalformationsDocument110 pagesImperforate Anus and Cloacal MalformationsAhmad Abu KushNo ratings yet
- Gerretsen 1981Document6 pagesGerretsen 1981Min ThuNo ratings yet
- Anatomic Aspects of Vaginal Eversion After Hysterectomy Delancey PDFDocument12 pagesAnatomic Aspects of Vaginal Eversion After Hysterectomy Delancey PDFANA ROSA HERNANDEZ HERNANDEZNo ratings yet
- Mechanism of LaborDocument34 pagesMechanism of LaborHenok Y KebedeNo ratings yet
- Lec.18 Genitourinary DysfunctionDocument37 pagesLec.18 Genitourinary Dysfunctionشريف محمد حسين شريف يوسفNo ratings yet
- KistokelDocument4 pagesKistokelIntan PermataNo ratings yet
- Diagnosis and Management of Pelvic Organ ProlapseDocument47 pagesDiagnosis and Management of Pelvic Organ ProlapseWindy Puspa Kusumah100% (1)
- Pop QDocument45 pagesPop QObgyn Maret2016No ratings yet
- Trans - OB 2 (Placenta Previa & Morbidly Adherent Placenta) PDFDocument5 pagesTrans - OB 2 (Placenta Previa & Morbidly Adherent Placenta) PDFMary Stephanie Parcon ChongNo ratings yet
- Klee Man 2005Document6 pagesKlee Man 2005erlita28No ratings yet
- Dashe 2013Document5 pagesDashe 2013Nữ Vương Nguyễn TrầnNo ratings yet
- 2018my Zamala BreechmalpresentationDocument72 pages2018my Zamala BreechmalpresentationSaeed HasanNo ratings yet
- USG Trimester 2 & 3 PatologisDocument48 pagesUSG Trimester 2 & 3 PatologisanggitaNo ratings yet
- USG Trimester 2 & 3 PatologisDocument48 pagesUSG Trimester 2 & 3 PatologisanggitaNo ratings yet
- Labor Part 1Document7 pagesLabor Part 1RANDY ERNEST GESTOSANINo ratings yet
- Ruiz, P. - SGD and NCP On Imperforate AnusDocument8 pagesRuiz, P. - SGD and NCP On Imperforate AnusPatricia Dianne RuizNo ratings yet
- HisterectomíaDocument2 pagesHisterectomíaTamara PricilaNo ratings yet
- Anatomy of The Vulva and The Female Sexual Response 2016 Obstetrics and Gynecology Clinics of North AmericaDocument18 pagesAnatomy of The Vulva and The Female Sexual Response 2016 Obstetrics and Gynecology Clinics of North Americafujimeister0% (1)
- Endometriosis Infiltrating The Lateral ParametriumDocument7 pagesEndometriosis Infiltrating The Lateral ParametriumAgung SentosaNo ratings yet
- Trans Male ReproDocument4 pagesTrans Male ReproJames MaravillasNo ratings yet
- Anatomy Physiology and Diagnosis of COlorectalDocument15 pagesAnatomy Physiology and Diagnosis of COlorectalOvamelia JulioNo ratings yet
- POPQDocument15 pagesPOPQKhairul ShafiqNo ratings yet
- Sonographic Findings in Acute Urinary Retention Secondary To Retroverted Gravid Uterus: Pathophysiology and Preventive MeasuresDocument6 pagesSonographic Findings in Acute Urinary Retention Secondary To Retroverted Gravid Uterus: Pathophysiology and Preventive MeasuresEndrianus Jaya PutraNo ratings yet
- The Uterus - Structure - Location - Vasculature - TeachMeAnatomyDocument5 pagesThe Uterus - Structure - Location - Vasculature - TeachMeAnatomywzt2001No ratings yet
- 1.01 Esophagus and Diaphragmatic HerniaDocument10 pages1.01 Esophagus and Diaphragmatic HerniaZazaNo ratings yet
- MCN 2Document7 pagesMCN 2GabNo ratings yet
- General Aspects On Post Partum Care of Laparoschisis in NewbornsDocument8 pagesGeneral Aspects On Post Partum Care of Laparoschisis in NewbornsErica DagdagNo ratings yet
- Ob8pg PDFDocument8 pagesOb8pg PDFErica DagdagNo ratings yet
- Ultrasound of The Abdominal Wall and GroinDocument11 pagesUltrasound of The Abdominal Wall and Groinfahmi rosyadiNo ratings yet
- The Value of Transperineal Three Dimensional Pelvic Floor Ultrasound in The Observation of Pelvic Support in Primipara WomenDocument6 pagesThe Value of Transperineal Three Dimensional Pelvic Floor Ultrasound in The Observation of Pelvic Support in Primipara WomenHerald Scholarly Open AccessNo ratings yet
- INGUINAL HERNIAS and HYDROCELES Ashcraft's Pediatric Surgery 5th EditionDocument7 pagesINGUINAL HERNIAS and HYDROCELES Ashcraft's Pediatric Surgery 5th EditionEmma AssagafNo ratings yet
- Prolapse Organ Pelvic 2010 Rev HahahaDocument42 pagesProlapse Organ Pelvic 2010 Rev HahahaResti CahyaniNo ratings yet
- Gross Anatomy of Uterus: D R. Vibhash Kumar Vaidya Department of AnatomyDocument25 pagesGross Anatomy of Uterus: D R. Vibhash Kumar Vaidya Department of AnatomyAhsan TariqNo ratings yet
- Back Et Al - 2017 - Emergent Ultrasound Evaluation of The Pediatric Female PelvisDocument10 pagesBack Et Al - 2017 - Emergent Ultrasound Evaluation of The Pediatric Female PelvisBerry BancinNo ratings yet
- Focseneanu2015 PDFDocument3 pagesFocseneanu2015 PDFAniydaNo ratings yet
- Gravida - The Number of Pregnancies That o Progesterone Deprivation TheoryDocument27 pagesGravida - The Number of Pregnancies That o Progesterone Deprivation TheoryRoshin Tejero100% (1)
- 3 - Anatomy, Abdomen and Pelvis - Female Internal Genitals - StatPearls - NCBI BookshelfDocument10 pages3 - Anatomy, Abdomen and Pelvis - Female Internal Genitals - StatPearls - NCBI BookshelfmimatechcontabilidadNo ratings yet
- Obsgyn - Case (Prolaps Uteri)Document11 pagesObsgyn - Case (Prolaps Uteri)vitomasNo ratings yet
- Plprevia PDFDocument3 pagesPlprevia PDFAtikah RahmadhaniNo ratings yet
- POP Review DietzDocument7 pagesPOP Review DietznadiaNo ratings yet
- Pelvic Organ Prolapse 2222222222222222222Document9 pagesPelvic Organ Prolapse 2222222222222222222Cristian C BecerraNo ratings yet
- The Great Obstetrical SyndromesDocument19 pagesThe Great Obstetrical SyndromeswadhitaubahNo ratings yet
- Fetal OrientationDocument4 pagesFetal Orientationangela mamauagNo ratings yet
- PREVENTIVEDocument12 pagesPREVENTIVEDivine SangutanNo ratings yet
- BIOCHEMISTRYDocument11 pagesBIOCHEMISTRYDivine SangutanNo ratings yet
- MICROBIOLOGYDocument12 pagesMICROBIOLOGYDivine SangutanNo ratings yet
- PHYSIOLOGYDocument9 pagesPHYSIOLOGYDivine SangutanNo ratings yet
- PATHOLOGYDocument10 pagesPATHOLOGYDivine SangutanNo ratings yet
- BIOCHEMISTRYDocument11 pagesBIOCHEMISTRYDivine SangutanNo ratings yet
- Pharmacology 2010 MedboardDocument15 pagesPharmacology 2010 Medboarddave_dm13No ratings yet
- Vanhoutte2012 PDFDocument11 pagesVanhoutte2012 PDFDivine SangutanNo ratings yet
- Medicine FinalDocument26 pagesMedicine FinalDivine SangutanNo ratings yet
- ANATOMY MCQ - S and KEY ANSWERS 2010 MedboardDocument18 pagesANATOMY MCQ - S and KEY ANSWERS 2010 MedboardDivine SangutanNo ratings yet
- Guglielmi1998 PDFDocument40 pagesGuglielmi1998 PDFDivine SangutanNo ratings yet
- Fruit and Water Policy in School Pilot ProjectDocument2 pagesFruit and Water Policy in School Pilot ProjectDivine SangutanNo ratings yet
- Book Trans StrokeDocument1 pageBook Trans StrokeDivine SangutanNo ratings yet
- 2007 NeuroDocument6 pages2007 NeuroDivine SangutanNo ratings yet
- 2017histo ExamDocument8 pages2017histo ExamDivine SangutanNo ratings yet
- ORL-HNS TestBlueprintDocument2 pagesORL-HNS TestBlueprintDivine SangutanNo ratings yet
- Study Notes Obstetrics GynecologyDocument55 pagesStudy Notes Obstetrics GynecologyMedShare82% (17)
- Obstetrics Test Blue PrintDocument8 pagesObstetrics Test Blue Printjose carlo araojoNo ratings yet
- 2010 - Macroanatomy 2Document3 pages2010 - Macroanatomy 2Divine SangutanNo ratings yet
- Board Examination Compre 1Document13 pagesBoard Examination Compre 1Avelina Suerte GuittapNo ratings yet
- Obstetrics Test Blue PrintDocument8 pagesObstetrics Test Blue Printjose carlo araojoNo ratings yet
- OB-GynMCQ S BlueprintDocument20 pagesOB-GynMCQ S BlueprintDivine Sangutan100% (1)
- ORL-HNS TestBlueprintDocument2 pagesORL-HNS TestBlueprintDivine SangutanNo ratings yet
- Answer Key To Ent QuestionsDocument2 pagesAnswer Key To Ent QuestionsDivine SangutanNo ratings yet
- International Research Journal of Pharmacy: Benign Prostatic Hyperplasia: Updated ReviewDocument7 pagesInternational Research Journal of Pharmacy: Benign Prostatic Hyperplasia: Updated ReviewRose DeasyNo ratings yet
- SMChejconf PaperDocument2 pagesSMChejconf PaperDivine SangutanNo ratings yet
- Ent MCQ A PFD PDFDocument61 pagesEnt MCQ A PFD PDFKay Bristol0% (1)
- Surgery Compilation PDFDocument92 pagesSurgery Compilation PDFDivine SangutanNo ratings yet
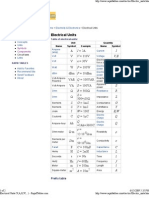
- Electrical UnitsDocument2 pagesElectrical Unitsevtoma100% (1)
- North Wester 2019 Second TermDocument20 pagesNorth Wester 2019 Second TermTharuka AdikariNo ratings yet
- 3d Printing CEDocument11 pages3d Printing CEShivam SamaiyaNo ratings yet
- Quantum Optical Memory For Entanglement DistributionDocument22 pagesQuantum Optical Memory For Entanglement DistributionJay-R Notorio PallegaNo ratings yet
- 8085 Microprocessor Programs: Microprocessor & Microcontroller Lab ManualDocument16 pages8085 Microprocessor Programs: Microprocessor & Microcontroller Lab ManualLIFE of PSNo ratings yet
- XT1C 160 TMD 25-450 4p F F: General InformationDocument3 pagesXT1C 160 TMD 25-450 4p F F: General InformationHenrics MayoresNo ratings yet
- Example Paper CC270 SpontaneousGenDocument14 pagesExample Paper CC270 SpontaneousGenLaert VeliaNo ratings yet
- Chemistry Manual NewDocument44 pagesChemistry Manual NewRACHETA BHARATNo ratings yet
- s67 Rosen Thermo - Hi.pvc Iz 2018 enDocument34 pagess67 Rosen Thermo - Hi.pvc Iz 2018 enSomea NoneaNo ratings yet
- Toro Wheelhorse Demystification Electical Wiring Diagrams For All WheelHorse TractorsDocument546 pagesToro Wheelhorse Demystification Electical Wiring Diagrams For All WheelHorse TractorsKevins Small Engine and Tractor Service69% (32)
- 17.11.1501 - Andhy Panca SaputraDocument10 pages17.11.1501 - Andhy Panca SaputraRiyan pandusadewoNo ratings yet
- ME:5160 (58:160) Intermediate Mechanics of Fluids Fall 2021 - HW6 SolutionDocument6 pagesME:5160 (58:160) Intermediate Mechanics of Fluids Fall 2021 - HW6 SolutionDiki AgungNo ratings yet
- Fkeyrouz@ndu - Edu.lb: Systems Using MATLAB, Second Edition, Prentice Hall 2002Document2 pagesFkeyrouz@ndu - Edu.lb: Systems Using MATLAB, Second Edition, Prentice Hall 2002Elio EidNo ratings yet
- RPI Form PDFDocument1 pageRPI Form PDFJoko WiwiNo ratings yet
- Control of Compressor Surge With Rotating Stall: Jan Van Helvoirt, Bram de Jager, Maarten SteinbuchDocument1 pageControl of Compressor Surge With Rotating Stall: Jan Van Helvoirt, Bram de Jager, Maarten Steinbuchinam vfNo ratings yet
- 299509Document2 pages299509Shahed FacebookNo ratings yet
- Automated Zone Speci C Irrigation With Wireless Sensor Actuator Network and Adaptable Decision SupportDocument28 pagesAutomated Zone Speci C Irrigation With Wireless Sensor Actuator Network and Adaptable Decision SupportNakal Hans Beta VersionNo ratings yet
- Pantron Amplifier ISG-N138 DatasheetDocument7 pagesPantron Amplifier ISG-N138 DatasheetlutfirozaqiNo ratings yet
- DC80D MK3 Genset Controller User Manual V1.1Document37 pagesDC80D MK3 Genset Controller User Manual V1.1nathalie gonzelez100% (1)
- IT Companies - in MumbaiDocument22 pagesIT Companies - in MumbaiRicky OrtizNo ratings yet
- 3 Chrono VisualizationDocument24 pages3 Chrono VisualizationVikramnath VenkatasubramaniNo ratings yet
- AWS TCO WorkSpacesDocument16 pagesAWS TCO WorkSpacessantuchetuNo ratings yet
- Data Sartocon X-Cap15 SPC2065-eDocument2 pagesData Sartocon X-Cap15 SPC2065-eJosé Ramón Devan DevanNo ratings yet
- Study of RGB Color Classification Using Fuzzy LogicDocument6 pagesStudy of RGB Color Classification Using Fuzzy LogicBhavin GajjarNo ratings yet
- 24945: FISS 011 - Fisica Experimental II - 005: Coulombs Law SimulationDocument2 pages24945: FISS 011 - Fisica Experimental II - 005: Coulombs Law SimulationAlberto GMNo ratings yet
- Xenon LampDocument25 pagesXenon LampJamaica Peñaloza NatuelNo ratings yet
- Model 4WI 100 - 800 HP Boilers: 1.4 SubmittalsDocument4 pagesModel 4WI 100 - 800 HP Boilers: 1.4 SubmittalssebaversaNo ratings yet
- Availability Simulation - IsographDocument1 pageAvailability Simulation - IsographsaospieNo ratings yet
- AGN 234 - Generating Set Assembly - AlignmentDocument6 pagesAGN 234 - Generating Set Assembly - AlignmentbaljeetjatNo ratings yet
- Usp31nf26s1 - c731, General Chapters - 731 - LOSS ON DRYINGDocument1 pageUsp31nf26s1 - c731, General Chapters - 731 - LOSS ON DRYINGEfsha KhanNo ratings yet