You might also like
- E 2182 - 02 - Rtixodi - PDFDocument36 pagesE 2182 - 02 - Rtixodi - PDFumur kaçamaklıNo ratings yet
- A Quick Introduction To XMLDocument3 pagesA Quick Introduction To XMLZL2ABVNo ratings yet
- XML Signature Syntax and ProcessingDocument53 pagesXML Signature Syntax and ProcessingHelen GrayNo ratings yet
- Analytical Data Interchange Protocol For Mass Spectrometric DataDocument25 pagesAnalytical Data Interchange Protocol For Mass Spectrometric DataPYDNo ratings yet
- XML identification and descriptionDocument5 pagesXML identification and descriptionMultan Singh BhatiNo ratings yet
- XML-based Content Management: Integration, Methodologies and ToolsFrom EverandXML-based Content Management: Integration, Methodologies and ToolsNo ratings yet
- XML APPLICATIONS Ijariie4092Document4 pagesXML APPLICATIONS Ijariie4092ナレシュ ナヤクNo ratings yet
- Mil DTL 87269DDocument14 pagesMil DTL 87269DChhoteeNo ratings yet
- Mil DTL 87269DDocument14 pagesMil DTL 87269DChhoteeNo ratings yet
- Extensible Markup LanguageDocument74 pagesExtensible Markup LanguagekalyanvsinfoNo ratings yet
- HL7 Recommendation: Using XML As A Supplementary Messaging Syntax For HL7 Version 2.3.1Document25 pagesHL7 Recommendation: Using XML As A Supplementary Messaging Syntax For HL7 Version 2.3.1David Uribe KatzNo ratings yet
- Introduction To XML: A Universal Data FormatDocument41 pagesIntroduction To XML: A Universal Data FormatPhuong LeNo ratings yet
- E 1948 - 98 - Rte5ndgtotgDocument7 pagesE 1948 - 98 - Rte5ndgtotgPrakash MakadiaNo ratings yet
- Q.1) Relation Between XML, HTML, SGML. Relation Between XML and HTMLDocument7 pagesQ.1) Relation Between XML, HTML, SGML. Relation Between XML and HTMLariyan8841No ratings yet
- SoaDocument129 pagesSoaBala Krishnan100% (1)
- Overview of XMLDocument28 pagesOverview of XMLhamshenryNo ratings yet
- Unit Iii XML: Cs T63 - Web Technology - Unit 3Document46 pagesUnit Iii XML: Cs T63 - Web Technology - Unit 3sankrajegowdaNo ratings yet
- E 1715 - 99 Rte3mtutotkDocument25 pagesE 1715 - 99 Rte3mtutotkMarceloNo ratings yet
- SOA Ans Bank For MIDDocument15 pagesSOA Ans Bank For MIDpalakNo ratings yet
- Computerized Exchange of Corrosion Data For MetalsDocument10 pagesComputerized Exchange of Corrosion Data For MetalswellbeingempireNo ratings yet
- Unit 3 Working With XML Introduction To XMLDocument41 pagesUnit 3 Working With XML Introduction To XMLAishwaryaNo ratings yet
- Analytical Data Interchange Protocol For Mass Spectrometric DataDocument13 pagesAnalytical Data Interchange Protocol For Mass Spectrometric DataPYDNo ratings yet
- Using XML With The Progress 4gl by Gus BjorklundDocument18 pagesUsing XML With The Progress 4gl by Gus Bjorklunddilks_100% (1)
- Introduction To Informatics - Fall 02Document40 pagesIntroduction To Informatics - Fall 02vinothNo ratings yet
- Computerized Exchange of Corrosion Data For MetalsDocument10 pagesComputerized Exchange of Corrosion Data For Metalsmohammed karasnehNo ratings yet
- XML is used to store data which is read by people or by machinesDocument19 pagesXML is used to store data which is read by people or by machinesDivya guptaNo ratings yet
- E5x Implementation For OrganisationsDocument9 pagesE5x Implementation For OrganisationsAnushka MohitNo ratings yet
- W3C.xml Path Language (XPath) 2Document105 pagesW3C.xml Path Language (XPath) 2bogirajaNo ratings yet
- XML and Oracle: A How-To Guide for PL/SQL UsersDocument11 pagesXML and Oracle: A How-To Guide for PL/SQL UsersEyad Muin IbdairNo ratings yet
- 3 XML DTD and XSLTDocument4 pages3 XML DTD and XSLTshivali.maliNo ratings yet
- XML Signature Syntax and Processing (Second Edition)Document44 pagesXML Signature Syntax and Processing (Second Edition)Sergio ArcangeliNo ratings yet
- XML Technology Family RolesDocument23 pagesXML Technology Family Rolesram krishnaNo ratings yet
- XML Signature Syntax and Processing (Second Edition) : W3C Recommendation 10 June 2008Document47 pagesXML Signature Syntax and Processing (Second Edition) : W3C Recommendation 10 June 2008Julio SantosNo ratings yet
- XMLDocument40 pagesXMLVaishnavi ChauhanNo ratings yet
- Analytical Data Interchange Protocol For Chromatographic DataDocument7 pagesAnalytical Data Interchange Protocol For Chromatographic DatapechugonisNo ratings yet
- Part II: Document Type Definitions: PrefaceDocument1 pagePart II: Document Type Definitions: PrefaceSai KuamrNo ratings yet
- XML Basics and .NET Support for XMLDocument13 pagesXML Basics and .NET Support for XMLArjun DomleNo ratings yet
- WT Unit-3 NotesDocument41 pagesWT Unit-3 NoteslavanyaNo ratings yet
- XML Unit 3Document75 pagesXML Unit 3Tammaneni NavyaNo ratings yet
- UNIT 2 - XML Complete WTDocument131 pagesUNIT 2 - XML Complete WTPrasanna PrasannaNo ratings yet
- What Is An XML Schema?Document12 pagesWhat Is An XML Schema?HarshaNo ratings yet
- ETP Specification v1.2 Doc v1.1Document515 pagesETP Specification v1.2 Doc v1.1Jose PalumboNo ratings yet
- Linking To Linguistic Data Categories in Isocat: Abstract Iso Technical Committee 37, Terminology and Other Language andDocument9 pagesLinking To Linguistic Data Categories in Isocat: Abstract Iso Technical Committee 37, Terminology and Other Language andChihebeddine AmmarNo ratings yet
- XML Syntax 2Document11 pagesXML Syntax 2Rajesh Bindumadhav MatthNo ratings yet
- Unit 1: Benefits of XML 1.structured DocumentDocument26 pagesUnit 1: Benefits of XML 1.structured Document923 Rishi kumar G GNo ratings yet
- Type Safe XML Generation in ScalaDocument7 pagesType Safe XML Generation in ScalaCoolToad484No ratings yet
- Module 2: Selecting and Navigating Nodes Using XpathDocument56 pagesModule 2: Selecting and Navigating Nodes Using XpathArtem RodionovNo ratings yet
- XML Signature Syntax and ProcessingDocument51 pagesXML Signature Syntax and ProcessingAlexandraNo ratings yet
- Seg 2Document20 pagesSeg 2Liavon SokalNo ratings yet
- CDA L1 R1 Schema: XML Schemas For CDA Level 1 Release 1Document54 pagesCDA L1 R1 Schema: XML Schemas For CDA Level 1 Release 1Andrea RiañoNo ratings yet
- 0021 Content 02654Document15 pages0021 Content 02654khfifi mohamedNo ratings yet
- Table and Descriptor Templates PDFDocument13 pagesTable and Descriptor Templates PDFRahul C RNo ratings yet
- XML DatabasesDocument11 pagesXML DatabasesElite TutorsNo ratings yet
- XML Programming: The Ultimate Guide to Fast, Easy, and Efficient Learning of XML ProgrammingFrom EverandXML Programming: The Ultimate Guide to Fast, Easy, and Efficient Learning of XML ProgrammingRating: 2.5 out of 5 stars2.5/5 (2)
- 2 Marksand 16 Marks - SOADocument15 pages2 Marksand 16 Marks - SOAThangaselviGovindarajNo ratings yet
- Three methods for posing database queriesDocument4 pagesThree methods for posing database querieseisaNo ratings yet
- Subject Name: Web Engineering Subject Code: CS-7003 Semester: 7Document25 pagesSubject Name: Web Engineering Subject Code: CS-7003 Semester: 7Amit SahuNo ratings yet
- XML Difference FAQS Compiled-1Document7 pagesXML Difference FAQS Compiled-1Umar AliNo ratings yet
- DITA: An XML-based Technical Documenta-Tion Authoring and Publishing ArchitectureDocument16 pagesDITA: An XML-based Technical Documenta-Tion Authoring and Publishing ArchitecturenaveenNo ratings yet
- The SEG Standard For Magnetotelluric DataDocument10 pagesThe SEG Standard For Magnetotelluric DataRemote Desktop RFINo ratings yet
- Aws d1.6 Ss Struct Welding CodeDocument215 pagesAws d1.6 Ss Struct Welding Codeumur kaçamaklıNo ratings yet
- En4179 DraftDocument7 pagesEn4179 Draftumur kaçamaklıNo ratings yet
- European Pressure Vessel Inspection StandardsDocument10 pagesEuropean Pressure Vessel Inspection Standardsumur kaçamaklıNo ratings yet
- PD Cen TR 10261 - 2013Document36 pagesPD Cen TR 10261 - 2013umur kaçamaklıNo ratings yet
- En 12681 Bi̇lgi̇Document9 pagesEn 12681 Bi̇lgi̇umur kaçamaklıNo ratings yet
- API 1104 Errata - 4and5Document5 pagesAPI 1104 Errata - 4and5umur kaçamaklıNo ratings yet
- En 10246-7 2005Document11 pagesEn 10246-7 2005umur kaçamaklıNo ratings yet
- En 10253 4 2008Document99 pagesEn 10253 4 2008umur kaçamaklıNo ratings yet
- Licensed by Information Handling Services Licensed by Information Handling ServicesDocument2 pagesLicensed by Information Handling Services Licensed by Information Handling Servicesumur kaçamaklıNo ratings yet
- Asme B 16 10 1992Document39 pagesAsme B 16 10 1992umur kaçamaklıNo ratings yet
- E2736-10 Standard Guide For Digital Detector Array RadiologyDocument22 pagesE2736-10 Standard Guide For Digital Detector Array Radiologyumur kaçamaklıNo ratings yet
- BS en Iso 11970 2016Document28 pagesBS en Iso 11970 2016umur kaçamaklı100% (2)
- BS en 1559-2 2014Document28 pagesBS en 1559-2 2014umur kaçamaklı100% (1)
- Astm E2868 - 13Document5 pagesAstm E2868 - 13umur kaçamaklıNo ratings yet
- Asme B16 34 1996 Interpretations PDFDocument21 pagesAsme B16 34 1996 Interpretations PDFumur kaçamaklıNo ratings yet
- Asme B18 2 1 1996 PDFDocument55 pagesAsme B18 2 1 1996 PDFumur kaçamaklıNo ratings yet
- Asme B16 11 1996 PDFDocument27 pagesAsme B16 11 1996 PDFumur kaçamaklıNo ratings yet
- Iso 19840 2 2004Document22 pagesIso 19840 2 2004umur kaçamaklı0% (1)
- Asme B16-9-2012 PDFDocument52 pagesAsme B16-9-2012 PDFumur kaçamaklıNo ratings yet
- Iso 15614 8 2002 PDFDocument26 pagesIso 15614 8 2002 PDFumur kaçamaklıNo ratings yet
- Asme B 16 1 1998 PDFDocument41 pagesAsme B 16 1 1998 PDFumur kaçamaklıNo ratings yet
- Asme B 16.5 1997 PDFDocument157 pagesAsme B 16.5 1997 PDFumur kaçamaklıNo ratings yet
- Iso 19675 2015 06 29 en PDFDocument23 pagesIso 19675 2015 06 29 en PDFcristobalNo ratings yet
- 2 5418388499906691582 PDFDocument12 pages2 5418388499906691582 PDFrezaNo ratings yet
- E 2212 - 02 - Rtiymti - PDFDocument21 pagesE 2212 - 02 - Rtiymti - PDFumur kaçamaklıNo ratings yet
- Iso 15607 2003Document24 pagesIso 15607 2003umur kaçamaklı100% (2)
- E 2210 - 02 - Rtiymta - PDFDocument13 pagesE 2210 - 02 - Rtiymta - PDFumur kaçamaklıNo ratings yet
- E 2171 - 02 - Rtixnze - PDFDocument23 pagesE 2171 - 02 - Rtixnze - PDFumur kaçamaklıNo ratings yet
- Telugu Boothu Kathala 16Document41 pagesTelugu Boothu Kathala 16peter parker25% (4)
- Europe - Returns Note PDFDocument1 pageEurope - Returns Note PDFDanaNo ratings yet
- InterventionDocument8 pagesInterventionFairy-Lou MejiaNo ratings yet
- PAN card request formDocument1 pagePAN card request formsrinivas moraNo ratings yet
- Smart Tube Free TemplateDocument59 pagesSmart Tube Free TemplateMETRO24JAM pracetakNo ratings yet
- Temporary signboard requirements road constructionDocument4 pagesTemporary signboard requirements road constructionAli Asyraf HamzahNo ratings yet
- IRJET Manuscript TemplateDocument2 pagesIRJET Manuscript TemplateSaurabh KhopadeNo ratings yet
- Superior Type Kunda Book SpecimenDocument19 pagesSuperior Type Kunda Book Specimenverticalgash100% (1)
- Calculating Time in The Different World Time Zones in Relation To The PhilippinesDocument17 pagesCalculating Time in The Different World Time Zones in Relation To The PhilippinesLinda Rotairo CosteloNo ratings yet
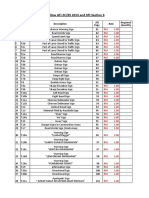
- Anilox and Sleeve List Aniloxes Bridge Sleeves: Worldwide Specialist in Machinery For The Flexible Packaging IndustryDocument1 pageAnilox and Sleeve List Aniloxes Bridge Sleeves: Worldwide Specialist in Machinery For The Flexible Packaging IndustryFlorin ArnautuNo ratings yet
- MES Program Internship GuideDocument11 pagesMES Program Internship GuideKhairul Anam ChowdhuryNo ratings yet
- Anatomy of A Letter 1Document3 pagesAnatomy of A Letter 1apriele rose hermogenesNo ratings yet
- Company ID card instructionsDocument1 pageCompany ID card instructionsNg AnggieNo ratings yet
- Handwriting During Early Childhood DevelDocument35 pagesHandwriting During Early Childhood DevelOkuzeneNo ratings yet
- Instructions Online Label Record: Usps Tracking #Document1 pageInstructions Online Label Record: Usps Tracking #Ernesto PadronNo ratings yet
- Postal Manual Vol V MCQDocument14 pagesPostal Manual Vol V MCQSauradipta MukherjeeNo ratings yet
- UTU M. Tech. Thesis - GuidelinesDocument21 pagesUTU M. Tech. Thesis - GuidelinesABHI THAKKARNo ratings yet
- Tarot SssDocument5 pagesTarot SssVi Na KumarNo ratings yet
- Taxipermit1 8winlist2014Document1,963 pagesTaxipermit1 8winlist2014Sandesh M Madkaikar100% (1)
- Ea Surcharge EuropeDocument1,119 pagesEa Surcharge Europealihossain armanNo ratings yet
- Prapanchasara Sara Sangraha Part-IiDocument1 pagePrapanchasara Sara Sangraha Part-IiPallab ChakrabortyNo ratings yet
- Legal Writing PointsDocument5 pagesLegal Writing Pointsdarling adjahoeNo ratings yet
- Publish Your Book On Amazon For Free - How To Self-Publish Without Paying A Dime (PDFDrive)Document105 pagesPublish Your Book On Amazon For Free - How To Self-Publish Without Paying A Dime (PDFDrive)Tristan BlakeNo ratings yet
- Formatting Paper for Conference ProceedingsDocument2 pagesFormatting Paper for Conference ProceedingsRose Chen Siew KeeNo ratings yet
- PlastexDocument98 pagesPlastexpaoloc19No ratings yet
- PH 2022Document16 pagesPH 2022y(tytytNo ratings yet
- Authority LetterDocument1 pageAuthority Letterrehan ul haqNo ratings yet
- Juarez Cartel SuitDocument52 pagesJuarez Cartel SuitAlex DerosierNo ratings yet
- STD 7 Chapter 6 NotesDocument3 pagesSTD 7 Chapter 6 NotesKunal SumukNo ratings yet
- A Primer On Writing Business Letters (Femme S. Writer 2011)Document27 pagesA Primer On Writing Business Letters (Femme S. Writer 2011)femme_s_writerNo ratings yet