You might also like
- Abnormal Labor. BBBB WWPPTXDocument53 pagesAbnormal Labor. BBBB WWPPTXHamss Ahmed100% (2)
- Herbs - Monograph On Marigold & DandelionDocument17 pagesHerbs - Monograph On Marigold & DandelionalbertofarmaNo ratings yet
- Neuro TherapyDocument505 pagesNeuro TherapyBrîndușa Petruțescu100% (8)
- Antenatal CareDocument12 pagesAntenatal CarefiramnNo ratings yet
- Drug ClassificationDocument14 pagesDrug ClassificationRPh Krishna Chandra Jagrit100% (2)
- SELECTION OF PUBLICATIONS-BACTALERT VIRTUO 9312725 010GBB Web PDFDocument21 pagesSELECTION OF PUBLICATIONS-BACTALERT VIRTUO 9312725 010GBB Web PDFSaifuddin KhaledNo ratings yet
- Science 9 Q1 Module 1 Respiratory and Circulatory With Key AnswerDocument42 pagesScience 9 Q1 Module 1 Respiratory and Circulatory With Key AnswerJan Ice90% (128)
- GCS dan REMS dalam Memprediksi Outcome Pasien Trauma KepalaDocument12 pagesGCS dan REMS dalam Memprediksi Outcome Pasien Trauma KepalaSatria Yosi HernawanNo ratings yet
- Jaa 9 155Document8 pagesJaa 9 155nesytiaraNo ratings yet
- OmeprazoleCisaprideAsthmaDocument6 pagesOmeprazoleCisaprideAsthmaRika SeptiawatiNo ratings yet
- Japanese Guidelines For Childhood Asthma 2017 PDFDocument15 pagesJapanese Guidelines For Childhood Asthma 2017 PDFcindy315No ratings yet
- Journal of Clinical Microbiology-2015-Van Ingen-2343.FullDocument3 pagesJournal of Clinical Microbiology-2015-Van Ingen-2343.Fullbunga farnadaNo ratings yet
- Perbandingan Perbaikan Nilai Peak Ekspiratory Flow Penggunaan Aminofilin Dan Salbutamol Pada Eksaserbasi AsmaDocument10 pagesPerbandingan Perbaikan Nilai Peak Ekspiratory Flow Penggunaan Aminofilin Dan Salbutamol Pada Eksaserbasi AsmarezaNo ratings yet
- Formoterol, A New Long-Acting Bronchodilator For InhalationDocument6 pagesFormoterol, A New Long-Acting Bronchodilator For InhalationAlief AkbarNo ratings yet
- Molecular Genetics and Metabolism Reports: Case ReportDocument4 pagesMolecular Genetics and Metabolism Reports: Case ReportLeidy Paola Gamboa GamboaNo ratings yet
- Normal Menstrual Cycle LectureDocument41 pagesNormal Menstrual Cycle LectureMorita Taka100% (1)
- Guide For Diagnosis and Treatment: Bronchial Asthma in Children 6 Years. Update 2016. Executive SummaryDocument3 pagesGuide For Diagnosis and Treatment: Bronchial Asthma in Children 6 Years. Update 2016. Executive SummaryLuis MtzNo ratings yet
- Levamisole in L.PDocument5 pagesLevamisole in L.PjalalfaizNo ratings yet
- Pi Is 1323893016301745Document27 pagesPi Is 1323893016301745Afria TikaNo ratings yet
- Antihistamines in Children and Adolescents: A Practical UpdateDocument10 pagesAntihistamines in Children and Adolescents: A Practical Updateahmed fareedNo ratings yet
- Fluconazole For The Treatment of Onychomycosis An UpdateDocument6 pagesFluconazole For The Treatment of Onychomycosis An UpdateRenée IbáñezNo ratings yet
- Jurnal Gerd 3Document6 pagesJurnal Gerd 3sega maulanaNo ratings yet
- Antihistamínicos en PediatríaDocument10 pagesAntihistamínicos en PediatríaAdrianRuizNo ratings yet
- Rhinitis, sinusitis, and ocular diseases phototherapyDocument7 pagesRhinitis, sinusitis, and ocular diseases phototherapyJulian LeeNo ratings yet
- Allergology InternationalDocument9 pagesAllergology InternationalTazrian FarahNo ratings yet
- Allergology InternationalDocument9 pagesAllergology Internationalvijay dagdiNo ratings yet
- Gosset Et Al. - 1991 - Increased Secretion of Tumor Necrosis Factor Alpha and Interleukin-6 by Alveolar Macrophages Consecutive To The DDocument11 pagesGosset Et Al. - 1991 - Increased Secretion of Tumor Necrosis Factor Alpha and Interleukin-6 by Alveolar Macrophages Consecutive To The DMaría Reynel TarazonaNo ratings yet
- Biologic Therapy For AsthmaDocument59 pagesBiologic Therapy For AsthmaErnesto Santiago HenriquezNo ratings yet
- Matera 2017Document8 pagesMatera 2017Yuni RochyaningsihNo ratings yet
- Nejmoa 1814917Document11 pagesNejmoa 1814917yasserNo ratings yet
- Review Differentiates Between Adult and Child Asthma TreatmentsDocument10 pagesReview Differentiates Between Adult and Child Asthma TreatmentsnadiaNo ratings yet
- Endozepine Stupor: Disease or Deception? A Critical Review: ReviewsDocument3 pagesEndozepine Stupor: Disease or Deception? A Critical Review: ReviewshungleteNo ratings yet
- Teofilina Vs AcebrofilinaDocument9 pagesTeofilina Vs AcebrofilinaAgencia FaroNo ratings yet
- 2.5 Ethambutol in The Treatment of Patients With Chronic Pulmonary TuberculosisDocument4 pages2.5 Ethambutol in The Treatment of Patients With Chronic Pulmonary TuberculosisRara IndrianiNo ratings yet
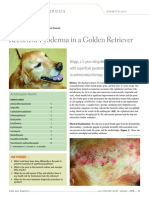
- Recurrent Pyoderma in a Golden RetrieverDocument2 pagesRecurrent Pyoderma in a Golden RetrieverArima ChatterjeeNo ratings yet
- Treatment of Larva Migrans Syndrome With Long-Term Administration of AlbendazoleDocument6 pagesTreatment of Larva Migrans Syndrome With Long-Term Administration of AlbendazoleSartika Ayu NingsihNo ratings yet
- Theophylline - Recent Advances in The Understanding of Its Mode of Action and Uses in Clinical PracticeDocument9 pagesTheophylline - Recent Advances in The Understanding of Its Mode of Action and Uses in Clinical PracticeAndreiNo ratings yet
- Fluticasone Furoate Nasal Spray PDFDocument6 pagesFluticasone Furoate Nasal Spray PDFDH DipuNo ratings yet
- Stigma Suicide and ReligionDocument2 pagesStigma Suicide and ReligionAndreas Dani TjNo ratings yet
- Chemical Composition and Anti-Inflammatory Activity of Essential Oils From The Leaves of Ocimum Basilicum L. and Ocimum Gratissimum L. (Lamiaceae)Document7 pagesChemical Composition and Anti-Inflammatory Activity of Essential Oils From The Leaves of Ocimum Basilicum L. and Ocimum Gratissimum L. (Lamiaceae)ahahahNo ratings yet
- Oral Esomeprazole in Japanese Pediatric Patients With Gastric Acid-Related Disease: Safety, Efficacy, and PharmacokineticsDocument9 pagesOral Esomeprazole in Japanese Pediatric Patients With Gastric Acid-Related Disease: Safety, Efficacy, and Pharmacokineticsdesak indryNo ratings yet
- Mepolizumab For Prednisone-Dependent Asthma With Sputum EosinophiliaDocument9 pagesMepolizumab For Prednisone-Dependent Asthma With Sputum EosinophiliaKinan BasalimNo ratings yet
- Articulo de Alergia A Polipropileno en Implante CoclearDocument9 pagesArticulo de Alergia A Polipropileno en Implante CoclearFreddy RojasNo ratings yet
- AlergiDocument37 pagesAlergidewapariyogaNo ratings yet
- Azathioprine: An immunosuppressant drugDocument4 pagesAzathioprine: An immunosuppressant drugasmanNo ratings yet
- Br. J. Anaesth. 2013 Schutte Bja Aet257Document4 pagesBr. J. Anaesth. 2013 Schutte Bja Aet257Mădălina RădulescuNo ratings yet
- Use of Biologics in AsthmaDocument55 pagesUse of Biologics in Asthmaosama.khalifaNo ratings yet
- Celvapan LeafletDocument30 pagesCelvapan LeafletEllaNo ratings yet
- Multidrug Resistant Pneumonia: A Case Study: April 2018Document4 pagesMultidrug Resistant Pneumonia: A Case Study: April 2018ummuNo ratings yet
- EosinófilosDocument13 pagesEosinófilosdkbritobNo ratings yet
- Studying The Release Ratio of Some PPIsDocument7 pagesStudying The Release Ratio of Some PPIsSamer HoushehNo ratings yet
- Asthma Diagnosis & Treatment GuideDocument5 pagesAsthma Diagnosis & Treatment GuideShalini ShanmugalingamNo ratings yet
- Case 15-2007: A 20-Year-Old Woman With Asthma and Cardiorespiratory ArrestDocument9 pagesCase 15-2007: A 20-Year-Old Woman With Asthma and Cardiorespiratory ArresteliNo ratings yet
- Journal of Otolaryngology and Rhinology Jor 1 009Document8 pagesJournal of Otolaryngology and Rhinology Jor 1 009Rizki Putri AndiniNo ratings yet
- Mepolizumab for treatment of adolescents and adults with eosinophilic oesophagitis: a multicentre, randomised, double-blind, placebo-controlled clinical trialDocument10 pagesMepolizumab for treatment of adolescents and adults with eosinophilic oesophagitis: a multicentre, randomised, double-blind, placebo-controlled clinical trialLindsay CortrightNo ratings yet
- Ig E-Mediated Immediate-Type Hypersensitivity To The Pyrazolone Drug PropyphenazoneDocument7 pagesIg E-Mediated Immediate-Type Hypersensitivity To The Pyrazolone Drug PropyphenazoneSergioNo ratings yet
- Clinical Effects of Apple Polyphenols On Persistent Allergic Rhinitis: A Randomized Double-Blind Placebo-Controlled Parallel Arm StudyDocument7 pagesClinical Effects of Apple Polyphenols On Persistent Allergic Rhinitis: A Randomized Double-Blind Placebo-Controlled Parallel Arm StudyadistimayaNo ratings yet
- Mepolizumab COPD NEJMDocument17 pagesMepolizumab COPD NEJM5fqkqkcdhtNo ratings yet
- Drug Study: La Salle UniversityDocument3 pagesDrug Study: La Salle UniversityJb RosillosaNo ratings yet
- Mild Persistent Asthma JournalDocument6 pagesMild Persistent Asthma JournalMohammed Ramzy GhifariNo ratings yet
- Letrozole For Patients With PCOSDocument4 pagesLetrozole For Patients With PCOSGevania ArantzaNo ratings yet
- Allergology InternationalDocument10 pagesAllergology InternationalaliNo ratings yet
- Anti-Immunoglobulin E (Omalizumab) Therapy in Seasonal Allergic RhinitisDocument4 pagesAnti-Immunoglobulin E (Omalizumab) Therapy in Seasonal Allergic RhinitisAndri SaputraNo ratings yet
- Pharmacogenetics of Inhaled Long-Acting Beta2-Agonists in Asthma A Systematic ReviewDocument29 pagesPharmacogenetics of Inhaled Long-Acting Beta2-Agonists in Asthma A Systematic Reviewwawa chenNo ratings yet
- Anaphylaxis: Watch For Any One of The Following Signs of AnaphylaxisDocument1 pageAnaphylaxis: Watch For Any One of The Following Signs of AnaphylaxisBrîndușa PetruțescuNo ratings yet
- Alternaria Alternata: Allergen ExposureDocument13 pagesAlternaria Alternata: Allergen ExposureBrîndușa PetruțescuNo ratings yet
- Patient Education: Preventing Diabetic Foot InfectionsDocument9 pagesPatient Education: Preventing Diabetic Foot InfectionsBrîndușa PetruțescuNo ratings yet
- Ains RecomandariDocument2 pagesAins RecomandariBrîndușa PetruțescuNo ratings yet
- 5-NOVELTIES IN THE MANAGEMENT OF ROSACEA en 370Document6 pages5-NOVELTIES IN THE MANAGEMENT OF ROSACEA en 370Brîndușa PetruțescuNo ratings yet
- Patient Education: Preventing Diabetic Foot InfectionsDocument9 pagesPatient Education: Preventing Diabetic Foot InfectionsBrîndușa PetruțescuNo ratings yet
- Drug Allergy Skin Test, Test Dose, Desensitization AAAAI 2014Document35 pagesDrug Allergy Skin Test, Test Dose, Desensitization AAAAI 2014Brîndușa PetruțescuNo ratings yet
- Atopy Patch Test: Indian Journal of Dermatology Venereology and Leprology May 2019Document5 pagesAtopy Patch Test: Indian Journal of Dermatology Venereology and Leprology May 2019Brîndușa PetruțescuNo ratings yet
- Budgerigar Droppings (Excremente de Perus) : Potential Cross-ReactivityDocument15 pagesBudgerigar Droppings (Excremente de Perus) : Potential Cross-ReactivityBrîndușa PetruțescuNo ratings yet
- Chronic Spontaneous 20200507Document1 pageChronic Spontaneous 20200507Brîndușa PetruțescuNo ratings yet
- Molecular Cloning and Characterization of Rubber Biosynthetic Genes From Taraxacum Koksaghyz - Schmidt 2010Document9 pagesMolecular Cloning and Characterization of Rubber Biosynthetic Genes From Taraxacum Koksaghyz - Schmidt 2010Brîndușa PetruțescuNo ratings yet
- Benralizumab Protocol For Severe Eosinophilic AsthmaDocument3 pagesBenralizumab Protocol For Severe Eosinophilic AsthmaBrîndușa PetruțescuNo ratings yet
- FasenraDocument12 pagesFasenraBrîndușa PetruțescuNo ratings yet
- Echinococcus Granulosus in Portugal TheDocument5 pagesEchinococcus Granulosus in Portugal TheBrîndușa PetruțescuNo ratings yet
- FASENRA - PFS To Pen Communication Downloadable PDFDocument2 pagesFASENRA - PFS To Pen Communication Downloadable PDFBrîndușa PetruțescuNo ratings yet
- Beta Lactam Allergy Jun 22 2017Document47 pagesBeta Lactam Allergy Jun 22 2017Brîndușa PetruțescuNo ratings yet
- 2Document13 pages2Brîndușa PetruțescuNo ratings yet
- n95 Mask DataDocument8 pagesn95 Mask DatatrebajumiknjigeNo ratings yet
- Abpa SeminarDocument38 pagesAbpa SeminarBrîndușa PetruțescuNo ratings yet
- A Positive Serum Basophil Histamine Release AssayDocument4 pagesA Positive Serum Basophil Histamine Release AssayBrîndușa PetruțescuNo ratings yet
- Chronic Spontaneous 20200507Document1 pageChronic Spontaneous 20200507Brîndușa PetruțescuNo ratings yet
- Penicillin Skin Testing Benzylpenicilloylpolylysine Pre Pen Frequently Asked Questions FinalDocument3 pagesPenicillin Skin Testing Benzylpenicilloylpolylysine Pre Pen Frequently Asked Questions FinalBrîndușa PetruțescuNo ratings yet
- Beta-Lactam Cross Reactivity PDFDocument5 pagesBeta-Lactam Cross Reactivity PDFBrîndușa PetruțescuNo ratings yet
- Beta-Lactam Cross Reactivity PDFDocument5 pagesBeta-Lactam Cross Reactivity PDFBrîndușa PetruțescuNo ratings yet
- Universitätsklinikum Des Saarlandes: Prof. Dr. Anh Tuan Dinh-Xuan and Prof. Dr. Vito BrusascoDocument2 pagesUniversitätsklinikum Des Saarlandes: Prof. Dr. Anh Tuan Dinh-Xuan and Prof. Dr. Vito BrusascoBrîndușa PetruțescuNo ratings yet
- Beta-Lactam Antibiotic Skin Testing and Oral Challenge: From The ACAAI 2015 Drug Allergy and Anaphylaxis CommitteeDocument13 pagesBeta-Lactam Antibiotic Skin Testing and Oral Challenge: From The ACAAI 2015 Drug Allergy and Anaphylaxis CommitteeBrîndușa PetruțescuNo ratings yet
- Laparoscopic Versus Open AppendectomyDocument25 pagesLaparoscopic Versus Open AppendectomyBrîndușa PetruțescuNo ratings yet
- Debate re diagnostic criteria for antibody deficiency disordersDocument18 pagesDebate re diagnostic criteria for antibody deficiency disordersBrîndușa PetruțescuNo ratings yet
- Name of Drug Mechanism of Action Indication Contraindication Side Effects Adverse Effects Nursing Consideration IndicationDocument2 pagesName of Drug Mechanism of Action Indication Contraindication Side Effects Adverse Effects Nursing Consideration IndicationBrian BaggayanNo ratings yet
- Doctor's OrderDocument2 pagesDoctor's OrderWiljohn de la CruzNo ratings yet
- Prostate cancer differential diagnosis and key considerationsDocument4 pagesProstate cancer differential diagnosis and key considerationsRobert StolnicuNo ratings yet
- Jurnal Implementasi NCP Pada DMDocument5 pagesJurnal Implementasi NCP Pada DMwidhy okayantiNo ratings yet
- Wheezing From PCODocument23 pagesWheezing From PCOShan KaiNo ratings yet
- Lecture 3-Epidemiological TriadDocument19 pagesLecture 3-Epidemiological Triadvikas takNo ratings yet
- Cucms Rheumatology Questions PDFDocument3 pagesCucms Rheumatology Questions PDFMaisara JhsNo ratings yet
- Risk For Aspiration Related To Esophageal Compromise Affecting The Lower Esophageal Sphincter As Evidenced by Heart Burn.Document2 pagesRisk For Aspiration Related To Esophageal Compromise Affecting The Lower Esophageal Sphincter As Evidenced by Heart Burn.eleinsamNo ratings yet
- Block M2 EYE Distribution by MMCDocument3 pagesBlock M2 EYE Distribution by MMCF ParikhNo ratings yet
- Dialog Diabetes B.inggris Kel 5-1Document4 pagesDialog Diabetes B.inggris Kel 5-1Desma LindaNo ratings yet
- NCP FinalDocument4 pagesNCP Finalmarkanthony3903No ratings yet
- Methods of Specimen Collection For Diagnosis of Superficial and Subcutaneous Fungal InfectionsDocument5 pagesMethods of Specimen Collection For Diagnosis of Superficial and Subcutaneous Fungal InfectionssaadmcsNo ratings yet
- ECG Report: An Overview of ElectrocardiographyDocument5 pagesECG Report: An Overview of Electrocardiographyالحارث فخري فياض احمدNo ratings yet
- Time Table Panitia - NewDocument3 pagesTime Table Panitia - NewcelinNo ratings yet
- Il Gem 4000 Operating and Maintenance ProcedureDocument15 pagesIl Gem 4000 Operating and Maintenance ProcedureHfsh OmerNo ratings yet
- Summary SecondANDl SetDocument57 pagesSummary SecondANDl SetPetros TemboNo ratings yet
- Supraglottic Airways in Difficult Airway Management: Successes, Failures, Use and MisuseDocument12 pagesSupraglottic Airways in Difficult Airway Management: Successes, Failures, Use and Misusejangkrik21No ratings yet
- Pathfit 1Document23 pagesPathfit 1Sep TemNo ratings yet
- Midwifery Pharmacology-7Document1 pageMidwifery Pharmacology-7georgeloto12No ratings yet
- Stool Exam Guide - Key Tests, Colors, Consistencies in 40 CharactersDocument8 pagesStool Exam Guide - Key Tests, Colors, Consistencies in 40 CharactersLester John HilarioNo ratings yet
- In-Press Article: Outcomes Following Severe Distal Tibial, Ankle, And/or Mid/Hindfoot TraumaDocument10 pagesIn-Press Article: Outcomes Following Severe Distal Tibial, Ankle, And/or Mid/Hindfoot TraumaDeng PanNo ratings yet
- SFP-Vol403 Unit2Document10 pagesSFP-Vol403 Unit2TnchNo ratings yet
- Current U.S. Military Fluid Replacement GuidelinesDocument6 pagesCurrent U.S. Military Fluid Replacement Guidelines"Rufus"No ratings yet
- Philippine College of Physicians Daily Census Ward Hospital de Los Santos-Sti Medical CenterDocument22 pagesPhilippine College of Physicians Daily Census Ward Hospital de Los Santos-Sti Medical Centercruz_johnraymondNo ratings yet