You might also like
- NclexDocument12 pagesNclexJosette Mae Atanacio100% (1)
- Ministry of Health Pharmaceutical VEN ListDocument25 pagesMinistry of Health Pharmaceutical VEN ListportosinNo ratings yet
- Rationale, Pre-Test Post-TestDocument9 pagesRationale, Pre-Test Post-TestNina OaipNo ratings yet
- Neurotransmitters AnxietyDocument7 pagesNeurotransmitters AnxietyMatthew SyNo ratings yet
- Table of Sedative, Hypnotic, AntianxietyDocument4 pagesTable of Sedative, Hypnotic, AntianxietyirfanzukriNo ratings yet
- Anesthesia PharmacologyDocument12 pagesAnesthesia PharmacologyMagy SnowNo ratings yet
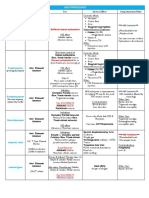
- Drugs FOR Psychiatric & Neurologic Disorders: Clonazepam (Klonopin, Rivotril) Midazolam (Versed, Dormicum)Document5 pagesDrugs FOR Psychiatric & Neurologic Disorders: Clonazepam (Klonopin, Rivotril) Midazolam (Versed, Dormicum)Noriko MatsumotoNo ratings yet
- 2018-2019 Cns DepressantsDocument5 pages2018-2019 Cns DepressantsMary AgorillaNo ratings yet
- Module 4: Neurologic Medications: TasksDocument5 pagesModule 4: Neurologic Medications: TasksSheril Marek0% (1)
- Pharmacology - Drugs For CNS DisordersDocument4 pagesPharmacology - Drugs For CNS DisordersJireh MejinoNo ratings yet
- Flumazenil Reverses The CNS Effects of BZDDocument3 pagesFlumazenil Reverses The CNS Effects of BZDLouradel AlfonsoNo ratings yet
- AnxiolyticsDocument8 pagesAnxiolyticsAlfie16No ratings yet
- Pharmacology IV L5Document4 pagesPharmacology IV L5سلطان القلحNo ratings yet
- 3.sedative and HypnoticsDocument24 pages3.sedative and HypnoticsGrishma ChokshiNo ratings yet
- Obat2 Yang Bekerja Pada Ganguan Kesadaran: Elly Usman Bagian Farmakologi Dan Terapi, Fakultas Kedokteran, UnandDocument29 pagesObat2 Yang Bekerja Pada Ganguan Kesadaran: Elly Usman Bagian Farmakologi Dan Terapi, Fakultas Kedokteran, UnandKhairani HakimNo ratings yet
- Barbiturates: of Action of GABA. Independent of GABADocument10 pagesBarbiturates: of Action of GABA. Independent of GABAAvi WerdesheimNo ratings yet
- Week 7 Course TaskDocument13 pagesWeek 7 Course TaskRachelle CambaNo ratings yet
- Psychopharmacological AgentsDocument44 pagesPsychopharmacological Agentsbazet49No ratings yet
- Stereotypical Behavior: Rate Dependence EffectsDocument2 pagesStereotypical Behavior: Rate Dependence EffectsJustin HulinNo ratings yet
- Modern Dravya GunaDocument21 pagesModern Dravya GunaAvinash Perfectt0% (2)
- Skeletal Muscle RelaxantsDocument2 pagesSkeletal Muscle RelaxantsRachel Ann FranchescaNo ratings yet
- Sedative HypnoticDocument60 pagesSedative HypnoticNeeraj KumarNo ratings yet
- Anxiolytics Sedatives Hypnotics Pharm 3Document38 pagesAnxiolytics Sedatives Hypnotics Pharm 3Peter Harris100% (1)
- Anxiolytics, Sedatives & Hypnotics: Mechanisms of Action & Clinical UsesDocument39 pagesAnxiolytics, Sedatives & Hypnotics: Mechanisms of Action & Clinical Usesgeng gengNo ratings yet
- Module IV: Central Nervous System MedicationsDocument4 pagesModule IV: Central Nervous System MedicationsVincent Paul SantosNo ratings yet
- Sedative HypnoticsDocument39 pagesSedative HypnoticsFatima ShaukatNo ratings yet
- Lecture 11 Sedative-Hypnotic and Anti-Anxiety AgentsDocument32 pagesLecture 11 Sedative-Hypnotic and Anti-Anxiety AgentsHafsa ShakilNo ratings yet
- Er-Drug StudyDocument41 pagesEr-Drug Studyrc_lacampuinganyahooNo ratings yet
- Sedative HynoticsDocument17 pagesSedative HynoticsAngel ShindeNo ratings yet
- Anxiolytics and HypnoticsDocument43 pagesAnxiolytics and HypnoticshamzabhayatNo ratings yet
- Anxiolytic, Sedative-Hypnotic DrugsDocument39 pagesAnxiolytic, Sedative-Hypnotic DrugsNina100% (1)
- AnxiolyticsDocument2 pagesAnxiolyticsChristel Mariz SantellaNo ratings yet
- General AnaesthesiaDocument21 pagesGeneral AnaesthesiahalayehiahNo ratings yet
- ? AnxiolyticsDocument2 pages? AnxiolyticsKarma iiiNo ratings yet
- Anti Anxiety DrugsDocument15 pagesAnti Anxiety DrugsMr. Psycho SamNo ratings yet
- Benzodiazepines + Local AnesthesiaDocument5 pagesBenzodiazepines + Local AnesthesiaALNAKINo ratings yet
- 7779087Document65 pages7779087MohamedNo ratings yet
- Pharmacology (All Lectures)Document283 pagesPharmacology (All Lectures)Youssef ElzataryNo ratings yet
- Central Nervous System: A Sedative Can Become A Hypnotic If It Is Given in Large Enough DosesDocument6 pagesCentral Nervous System: A Sedative Can Become A Hypnotic If It Is Given in Large Enough Doseschubbygunny_29776413No ratings yet
- Anxiolytic & Hypnotics Part 1Document28 pagesAnxiolytic & Hypnotics Part 1Sarah ArkanNo ratings yet
- Hypnotics and Sedatives PDFDocument35 pagesHypnotics and Sedatives PDFSayan Nag100% (1)
- Drug Study: West Visayas State University La Paz, Iloilo CityDocument3 pagesDrug Study: West Visayas State University La Paz, Iloilo CityBALOGO TRISHA MARIENo ratings yet
- DiazepamDocument3 pagesDiazepamGwyn RosalesNo ratings yet
- 7 Midazozalam Drug StudyDocument3 pages7 Midazozalam Drug Studyshadow gonzalezNo ratings yet
- Lecture Document (1st Mid)Document13 pagesLecture Document (1st Mid)Supti RahmanNo ratings yet
- Pharmacology of Sedative-HypnoticsDocument49 pagesPharmacology of Sedative-HypnoticsGeorge AbrahamNo ratings yet
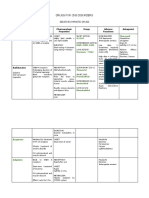
- I. Drug Study: Drug Mechanism of Action Indications Contraindication Side Effects Nursing ConsiderationsDocument3 pagesI. Drug Study: Drug Mechanism of Action Indications Contraindication Side Effects Nursing Considerationscyn yana0723No ratings yet
- 2016 Pharmacology of Sedative-HypnoticDocument46 pages2016 Pharmacology of Sedative-HypnoticFansisca SiallaganNo ratings yet
- CNS Depressants: Sedatives, Hypnotics, and Muscle RelaxantsDocument19 pagesCNS Depressants: Sedatives, Hypnotics, and Muscle RelaxantsAditya sagarNo ratings yet
- Sedative - HypnoticsDocument62 pagesSedative - HypnoticsvijayNo ratings yet
- Central Nervous System DepressantsDocument78 pagesCentral Nervous System DepressantsJan Dee ApuraNo ratings yet
- Sedation Reading TestDocument22 pagesSedation Reading TestJyothy AthulNo ratings yet
- Pharmacology of The Central Nervous System-1Document163 pagesPharmacology of The Central Nervous System-1Gølà Sèèñàà–baale irraaNo ratings yet
- Pcol 1 Prefinals Part 2 PDFDocument3 pagesPcol 1 Prefinals Part 2 PDFJillian Mae DacerNo ratings yet
- Sedative-Hypnotic Drugs - AMBOSSDocument8 pagesSedative-Hypnotic Drugs - AMBOSSRuva Oscass JimmyNo ratings yet
- Depression PDFDocument10 pagesDepression PDFLyadelou FortuNo ratings yet
- 2 Sedative-Hypnotics - Redi (Nema)Document58 pages2 Sedative-Hypnotics - Redi (Nema)Endre Shitaye KulkiNo ratings yet
- Drugs Used in Neuro PharmacologyDocument3 pagesDrugs Used in Neuro PharmacologyNabeel Kouka, MD, DO, MBA, MPH100% (1)
- 4 - Pharmacology of Anaesthesia (Updated)Document22 pages4 - Pharmacology of Anaesthesia (Updated)SivaNo ratings yet
- Use Cautiously in: History of suicide attempts or substance abuseDocument2 pagesUse Cautiously in: History of suicide attempts or substance abuseidullrufaidahNo ratings yet
- Characteristics Indication Origin Market Name Absorption Peak Plasma Level Half-Life Excretion DoseDocument4 pagesCharacteristics Indication Origin Market Name Absorption Peak Plasma Level Half-Life Excretion DoseShafiqah AbdullahNo ratings yet
- Indomethacin: Drugs MOA/Uses Side Effects OtherDocument2 pagesIndomethacin: Drugs MOA/Uses Side Effects OtherJustin HulinNo ratings yet
- Movement Disorder TreatmentsDocument3 pagesMovement Disorder TreatmentsJustin HulinNo ratings yet
- Stereotypical Behavior: Rate Dependence EffectsDocument2 pagesStereotypical Behavior: Rate Dependence EffectsJustin HulinNo ratings yet
- Medschool AnestheticsDocument4 pagesMedschool AnestheticsJustin HulinNo ratings yet
- Drug Abuse & DependenceDocument3 pagesDrug Abuse & DependenceJustin HulinNo ratings yet
- Psychoses: CNS Dopamine Levels Perception, Thought, Consciousness, Social, Affective DisordersDocument3 pagesPsychoses: CNS Dopamine Levels Perception, Thought, Consciousness, Social, Affective DisordersJustin Hulin100% (1)
- Antidepressants & Mood StabilizersDocument5 pagesAntidepressants & Mood StabilizersJustin HulinNo ratings yet
- Difficult Status Epilepticus: PhenytoinDocument6 pagesDifficult Status Epilepticus: PhenytoinJustin Hulin100% (1)
- Medical School AnalgesicsDocument3 pagesMedical School AnalgesicsJustin HulinNo ratings yet
- Med School AnticonvulsantsDocument6 pagesMed School AnticonvulsantsJustin HulinNo ratings yet
- Medical School AnalgesicsDocument3 pagesMedical School AnalgesicsJustin HulinNo ratings yet
- Medschool AnestheticsDocument4 pagesMedschool AnestheticsJustin HulinNo ratings yet
- Lista MedicamenteDocument4 pagesLista MedicamenteEstera-Beatrice ȘtefănuțiNo ratings yet
- How To Write A Good Abstract For A Scientific Paper or ConferenceDocument4 pagesHow To Write A Good Abstract For A Scientific Paper or Conference畏No ratings yet
- Comparison of BenzodiazepinesDocument8 pagesComparison of BenzodiazepinesDarryl BettsNo ratings yet
- Anticonvulsant Therapy in DogsDocument21 pagesAnticonvulsant Therapy in DogsConstanza Aedo SibilaNo ratings yet
- CNS Stimulants and Depressants PDFDocument5 pagesCNS Stimulants and Depressants PDFRizMarie100% (1)
- Nursing Process For Bipolar DisorderDocument37 pagesNursing Process For Bipolar DisorderDENVER CABADINNo ratings yet
- 4 6 11 950 PDFDocument8 pages4 6 11 950 PDFSurya WijayaNo ratings yet
- AnesDocument183 pagesAnesSholen SamaritaNo ratings yet
- Using in Children and Adolescents: BenzodiazepinesDocument4 pagesUsing in Children and Adolescents: BenzodiazepinesEunike KaramoyNo ratings yet
- Fneur 14 1175370Document10 pagesFneur 14 1175370WenSarmientoBNo ratings yet
- Understanding Sleep and Anxiety DisordersDocument8 pagesUnderstanding Sleep and Anxiety DisordersMae DoctoleroNo ratings yet
- Benzodiazepines 2022 Drug Fact Sheet - 1Document1 pageBenzodiazepines 2022 Drug Fact Sheet - 1Sharique KhanNo ratings yet
- Psychiatric Mental Health NursingDocument62 pagesPsychiatric Mental Health NursingHardeep KaurNo ratings yet
- Emergency Nursing QuestionsDocument60 pagesEmergency Nursing QuestionsVallesh ShettyNo ratings yet
- Icu PsychosisDocument23 pagesIcu PsychosisJisha JanardhanNo ratings yet
- Part XVIDocument17 pagesPart XVIphp_czarina04421No ratings yet
- NHS GuidelinesDocument339 pagesNHS GuidelinesAndri FerdianNo ratings yet
- Rapid Tranquilization Treatment FlowchartDocument1 pageRapid Tranquilization Treatment FlowchartKaren C. ManoodNo ratings yet
- Sedative & Hypnotics: Prof. Hanan Hagar Pharmacology Department Medical College King Saud UniversityDocument51 pagesSedative & Hypnotics: Prof. Hanan Hagar Pharmacology Department Medical College King Saud UniversityRose Ann Raquiza-PeranteNo ratings yet
- NCM105 13th PsychopharmacologyDocument17 pagesNCM105 13th PsychopharmacologyKamx MohammedNo ratings yet
- Psych Student NotesDocument23 pagesPsych Student NotesReymund Timog TalarocNo ratings yet
- Benzo ZdrugDocument12 pagesBenzo Zdruglnair_43No ratings yet
- Pediatric Status Epilepticus ManagementDocument7 pagesPediatric Status Epilepticus ManagementAndreaMenaWNo ratings yet
- Sedative Hypnotics: GABA Receptor Agonist (1:22)Document5 pagesSedative Hypnotics: GABA Receptor Agonist (1:22)Priyanka MonikaNo ratings yet
- CCSAP 2017book3 Sample ChapterDocument20 pagesCCSAP 2017book3 Sample ChapterMohanBabuNo ratings yet
- Topnotch Mnemonics - March 2019Document9 pagesTopnotch Mnemonics - March 2019euphrosyne92100% (1)
- Lorazepam Dosage, Uses, Side Effects and Nursing ResponsibilitiesDocument3 pagesLorazepam Dosage, Uses, Side Effects and Nursing ResponsibilitiesCHERISE CORDOVA100% (2)