You might also like
- A Simple Guide to Hand Tremors, Related Diseases and Use in Disease DiagnosisFrom EverandA Simple Guide to Hand Tremors, Related Diseases and Use in Disease DiagnosisRating: 3.5 out of 5 stars3.5/5 (3)
- Module 4: Neurologic Medications: TasksDocument5 pagesModule 4: Neurologic Medications: TasksSheril Marek0% (1)
- CNS Depressants - Anxiolytics & Sedative HypnoticsDocument4 pagesCNS Depressants - Anxiolytics & Sedative HypnoticsJustin HulinNo ratings yet
- Drugs FOR Psychiatric & Neurologic Disorders: Clonazepam (Klonopin, Rivotril) Midazolam (Versed, Dormicum)Document5 pagesDrugs FOR Psychiatric & Neurologic Disorders: Clonazepam (Klonopin, Rivotril) Midazolam (Versed, Dormicum)Noriko MatsumotoNo ratings yet
- 2010 (Chapter19 Final) Epilepsies 2Document20 pages2010 (Chapter19 Final) Epilepsies 2Candilicious10No ratings yet
- 14-Chapter 17-Drugs For EpilepsyDocument23 pages14-Chapter 17-Drugs For EpilepsyCandilicious10No ratings yet
- 02.01-04 CNS I - AntiepilepticsDocument10 pages02.01-04 CNS I - AntiepilepticsMiguel C. DolotNo ratings yet
- Pharmacology of Sedative-Hypnotics: DR - Datten Bangun, MSC, SPFK Dept - Farmakologi & Terapetik Fak - Kedokteran Uhn MedanDocument49 pagesPharmacology of Sedative-Hypnotics: DR - Datten Bangun, MSC, SPFK Dept - Farmakologi & Terapetik Fak - Kedokteran Uhn MedanGeorge AbrahamNo ratings yet
- Antiepileptic Medicines Shanbhag ShenoyDocument9 pagesAntiepileptic Medicines Shanbhag Shenoyshaziashaziashazia2001No ratings yet
- Pharma Topic 3 NotesDocument3 pagesPharma Topic 3 NotesAshley Franceska CansanayNo ratings yet
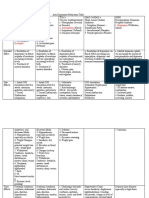
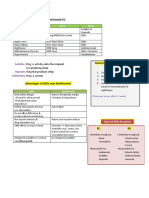
- Characteristics Indication Origin Market Name Absorption Peak Plasma Level Half-Life Excretion DoseDocument4 pagesCharacteristics Indication Origin Market Name Absorption Peak Plasma Level Half-Life Excretion DoseShafiqah AbdullahNo ratings yet
- PsychopharmacologyDocument5 pagesPsychopharmacologyADAL, KATE CARMELANo ratings yet
- Sedative - HypnoticsDocument62 pagesSedative - HypnoticsvijayNo ratings yet
- Lecture 8 Central Nervous System CnsDocument35 pagesLecture 8 Central Nervous System CnsakramuddaulaNo ratings yet
- CNS I Drug NotesDocument9 pagesCNS I Drug NotesErin YoungNo ratings yet
- Pharmacology (All Lectures)Document283 pagesPharmacology (All Lectures)Youssef ElzataryNo ratings yet
- Skeletal Muscle RelaxantsDocument21 pagesSkeletal Muscle RelaxantsKetan patilNo ratings yet
- Neurotransmitters AnxietyDocument7 pagesNeurotransmitters AnxietyMatthew SyNo ratings yet
- Lecture 11 Sedative-Hypnotic and Anti-Anxiety AgentsDocument32 pagesLecture 11 Sedative-Hypnotic and Anti-Anxiety AgentsHafsa ShakilNo ratings yet
- CC Rubie Ann G. Tillor: IM: (Schizophrenia)Document11 pagesCC Rubie Ann G. Tillor: IM: (Schizophrenia)Rubie Ann TillorNo ratings yet
- Barbiturates: of Action of GABA. Independent of GABADocument10 pagesBarbiturates: of Action of GABA. Independent of GABAAvi WerdesheimNo ratings yet
- DrUG STUDY PSYCHEDocument52 pagesDrUG STUDY PSYCHELiza MPNo ratings yet
- Depression PDFDocument10 pagesDepression PDFLyadelou FortuNo ratings yet
- Lecture 6 Autonomic Nervous SystemDocument17 pagesLecture 6 Autonomic Nervous SystemakramuddaulaNo ratings yet
- Drug Study HaloperidolDocument3 pagesDrug Study HaloperidolKrizzia FosterNo ratings yet
- Surgery Shelf Notes 2021 PDFDocument43 pagesSurgery Shelf Notes 2021 PDFBhandari SadikshyaNo ratings yet
- Antipsychotic Drugs-1Document5 pagesAntipsychotic Drugs-1Teddy linumbwaNo ratings yet
- PH - Karrar HaderDocument33 pagesPH - Karrar HaderAdnan YassinNo ratings yet
- Anxiolytics Sedatives Hypnotics Pharm 3Document38 pagesAnxiolytics Sedatives Hypnotics Pharm 3Peter Harris100% (1)
- NPLEX Combination Review Neurology - A: Paul S. Anderson, ND Medical Board Review ServicesDocument83 pagesNPLEX Combination Review Neurology - A: Paul S. Anderson, ND Medical Board Review ServicesValeria AcevedoNo ratings yet
- Antiepileptics IDocument33 pagesAntiepileptics Iلو ترىNo ratings yet
- Drugs Acting On Somatic Nervous SystemDocument25 pagesDrugs Acting On Somatic Nervous SystemcchatrumaNo ratings yet
- Sedative - HypnoticsDocument60 pagesSedative - HypnoticsNurul AinNo ratings yet
- Null 1Document60 pagesNull 1tbuyinza21apNo ratings yet
- Stereotypical Behavior: Rate Dependence EffectsDocument2 pagesStereotypical Behavior: Rate Dependence EffectsJustin HulinNo ratings yet
- Drug AnalysisDocument49 pagesDrug Analysisjomalaw6714No ratings yet
- PsychePharma 2pagesDocument2 pagesPsychePharma 2pagesBear GrylsNo ratings yet
- Penyalahgunaan ObatDocument26 pagesPenyalahgunaan Obatvinna iasyaNo ratings yet
- Drug Study FormatDocument7 pagesDrug Study FormatHAIDER JULAILINo ratings yet
- Er-Drug StudyDocument41 pagesEr-Drug Studyrc_lacampuinganyahooNo ratings yet
- All Other ClassificationsDocument6 pagesAll Other ClassificationsCorey100% (1)
- Prozac Venlafaxine Duloxetine Amitriptyline BupropionDocument3 pagesProzac Venlafaxine Duloxetine Amitriptyline BupropionMichael S. PetryNo ratings yet
- Sedative HynoticsDocument17 pagesSedative HynoticsAngel ShindeNo ratings yet
- Beers Criteria HandoutDocument3 pagesBeers Criteria Handoutapi-647779956No ratings yet
- Drugs For Psyciatric DisordersDocument19 pagesDrugs For Psyciatric Disordersapi-36993610% (1)
- Part Agents Act NG On The Central Ner Ous System: Liu JuntianDocument89 pagesPart Agents Act NG On The Central Ner Ous System: Liu Juntianapi-19916399No ratings yet
- Lec Discussion PcolDocument6 pagesLec Discussion PcolErnest Patrick MatiasNo ratings yet
- Anesthetics Fa 2022Document4 pagesAnesthetics Fa 2022Assanov AibekNo ratings yet
- 13 - Antiseizure AgentsDocument145 pages13 - Antiseizure AgentsALJHON OSORIONo ratings yet
- Sedative HypnoticsDocument39 pagesSedative HypnoticsFatima ShaukatNo ratings yet
- 1 - PharmacologyDocument18 pages1 - PharmacologyLuidgi MichelNo ratings yet
- Table of Sedative, Hypnotic, AntianxietyDocument4 pagesTable of Sedative, Hypnotic, AntianxietyirfanzukriNo ratings yet
- Anti DepressantDocument6 pagesAnti Depressantyahyaahmed152000No ratings yet
- Drug StudyDocument10 pagesDrug StudyRubie Ann TillorNo ratings yet
- Module 3: Pain Medications: TasksDocument9 pagesModule 3: Pain Medications: TasksSheril MarekNo ratings yet
- Basal GangliaDocument76 pagesBasal GangliaHussain ANo ratings yet
- Flumazenil Reverses The CNS Effects of BZDDocument3 pagesFlumazenil Reverses The CNS Effects of BZDLouradel AlfonsoNo ratings yet
- 7779087Document65 pages7779087MohamedNo ratings yet
- 911 Sedative-Hypnotics PDFDocument17 pages911 Sedative-Hypnotics PDFIkram HamacheNo ratings yet
- French LiteratureDocument65 pagesFrench Literatureverlaine88No ratings yet
- Umberto Eco - How To Write A Thesis EbookDocument8 pagesUmberto Eco - How To Write A Thesis Ebookfc51eh59100% (2)
- Newman's Apologia and The Drama of Faith and Reason - Draft5Document131 pagesNewman's Apologia and The Drama of Faith and Reason - Draft5Sancrucensis100% (6)
- Kontrak Jangka PanjangDocument26 pagesKontrak Jangka Panjanganon_800888083No ratings yet
- Gallstones Removal ReportDocument32 pagesGallstones Removal ReportRichard JacksonNo ratings yet
- Writers 39 Forum - 07 2018 PDFDocument68 pagesWriters 39 Forum - 07 2018 PDFGala Caesar AnugerahNo ratings yet
- The Work of Saturn According To DeeDocument13 pagesThe Work of Saturn According To DeeMrMantura100% (1)
- Skin Studio Powerpoint RevisedDocument8 pagesSkin Studio Powerpoint RevisedAngelo Jay MacaraegNo ratings yet
- Error 1797 PdfcreatorDocument2 pagesError 1797 PdfcreatorJulieNo ratings yet
- Intact (Polymeric/Blenderized) : Enteral Nutrition (Summary of Diet/Formula)Document2 pagesIntact (Polymeric/Blenderized) : Enteral Nutrition (Summary of Diet/Formula)Angela NeriNo ratings yet
- Active Shooter Incidents in The Us 2021 052322Document30 pagesActive Shooter Incidents in The Us 2021 052322ABC News PoliticsNo ratings yet
- Construction Productivity Norms ManpowerDocument1 pageConstruction Productivity Norms ManpowerSIVACHANDRAN50% (2)
- SAP Human Resources: Priya AroraDocument24 pagesSAP Human Resources: Priya AroraSARITANo ratings yet
- My Action Plan02023Document3 pagesMy Action Plan02023REYNALDO ESPARTERONo ratings yet
- BA316 International Business Trade Module 3 1Document12 pagesBA316 International Business Trade Module 3 1Pamela Rose CasenioNo ratings yet
- Pediatric Meds List1Document38 pagesPediatric Meds List1Arman Carl DulayNo ratings yet
- Price Elasticity of DemandDocument3 pagesPrice Elasticity of Demandssharma21No ratings yet
- Test Bank For Environmental Science 14th Edition William Cunningham Mary CunninghamDocument18 pagesTest Bank For Environmental Science 14th Edition William Cunningham Mary CunninghamAndi AnnaNo ratings yet
- Environmental Health and Sustainable Development in Ogoni DR Uzorka MainDocument31 pagesEnvironmental Health and Sustainable Development in Ogoni DR Uzorka MainBettyNo ratings yet
- ISO 9001 High Level Structure 1 NewDocument6 pagesISO 9001 High Level Structure 1 NewTony SinambelaNo ratings yet
- AOK Spec Only 2016-02Document17 pagesAOK Spec Only 2016-02Iulian MihaiNo ratings yet
- Arduino Electronics Blueprints - Sample ChapterDocument33 pagesArduino Electronics Blueprints - Sample ChapterPackt Publishing100% (1)
- Steel Nails From The United Arab Emirates: U.S. International Trade CommissionDocument68 pagesSteel Nails From The United Arab Emirates: U.S. International Trade CommissionAhmad AliNo ratings yet
- Front Office Reservation Department: Telephone EtiquetteDocument50 pagesFront Office Reservation Department: Telephone EtiquettePaola Quintos100% (1)
- "ACTIVITY 3: Let's Go Searching!" Proposed Research TitleDocument10 pages"ACTIVITY 3: Let's Go Searching!" Proposed Research TitleCeline Angela AbreaNo ratings yet
- 29-08-2017 38062 Meka Concrete Mixer Catalogue EngDocument16 pages29-08-2017 38062 Meka Concrete Mixer Catalogue EngSeif EddineNo ratings yet
- Blood Donor AppDocument5 pagesBlood Donor AppPriya DarshiniNo ratings yet
- Level 1 - Blackbeards Treasure PDFDocument28 pagesLevel 1 - Blackbeards Treasure PDFmrkanh67% (3)
- Financial Statement Analysis IIDocument21 pagesFinancial Statement Analysis IIJay-ar Castillo Watin Jr.No ratings yet
- Gcet Voice 2014 PDFDocument120 pagesGcet Voice 2014 PDFSmit SutharNo ratings yet