You might also like
- AbortionDocument3 pagesAbortionShaina MillanNo ratings yet
- Millan, Shaina Marie B. 12-04-2018 BSN-103 Ms. Riza MagsinoDocument3 pagesMillan, Shaina Marie B. 12-04-2018 BSN-103 Ms. Riza MagsinoShaina MillanNo ratings yet
- Anatomy & Physiology Laptop-4Ev9Il2O IP 192.168.43.96 MAC C8:FF:28l09:CD:49Document2 pagesAnatomy & Physiology Laptop-4Ev9Il2O IP 192.168.43.96 MAC C8:FF:28l09:CD:49Shaina MillanNo ratings yet
- 11 Functional Gordon Health Pattern QuestionsDocument5 pages11 Functional Gordon Health Pattern QuestionsShaina MillanNo ratings yet
- Tepid Sponge Bathplan and StrategiesDocument2 pagesTepid Sponge Bathplan and StrategiesShaina MillanNo ratings yet
- Olistic Ealth Odels: By: Cindy Abayan Aumie Ching Apple Dulig Shaina MillanDocument8 pagesOlistic Ealth Odels: By: Cindy Abayan Aumie Ching Apple Dulig Shaina MillanShaina MillanNo ratings yet
- Results Gram StainingDocument2 pagesResults Gram StainingShaina MillanNo ratings yet
- Nursing Diagnosis Cues Rank Justification According To ABC or Maslow'sDocument3 pagesNursing Diagnosis Cues Rank Justification According To ABC or Maslow'sShaina MillanNo ratings yet
- KWL DRRMDocument3 pagesKWL DRRMShaina MillanNo ratings yet
- Maternal Handouts Third Stage ComplicationsDocument7 pagesMaternal Handouts Third Stage ComplicationsShaina Millan100% (1)
- Lanuza Demo LabDocument57 pagesLanuza Demo LabShaina MillanNo ratings yet
- Maternal Handouts PowerDocument4 pagesMaternal Handouts PowerShaina MillanNo ratings yet
- AbortionDocument5 pagesAbortionShaina MillanNo ratings yet
- NCP GDMDocument5 pagesNCP GDMShaina MillanNo ratings yet
- Low Purine DietDocument2 pagesLow Purine DietShaina MillanNo ratings yet
- NCP GDMDocument5 pagesNCP GDMShaina Millan100% (1)
- AbortionDocument5 pagesAbortionShaina MillanNo ratings yet
- Low Purine DietDocument2 pagesLow Purine DietShaina MillanNo ratings yet
- Lanuza Demo LabDocument57 pagesLanuza Demo LabShaina MillanNo ratings yet
- Lunch With Rationale Low Purine DietDocument2 pagesLunch With Rationale Low Purine DietShaina MillanNo ratings yet
- The Fiction ExperienceDocument7 pagesThe Fiction ExperienceShaina MillanNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- OneShot - How Do Organisms ReproduceDocument84 pagesOneShot - How Do Organisms ReproduceMuskan GoyalNo ratings yet
- Factors Contributing To Low Uptake of Family Planning Services in Salaga (Recovered)Document70 pagesFactors Contributing To Low Uptake of Family Planning Services in Salaga (Recovered)Seyram RichardNo ratings yet
- NCP Cord Prolapse Frias Ea Lissandra CDocument2 pagesNCP Cord Prolapse Frias Ea Lissandra CFatima Medriza Duran0% (1)
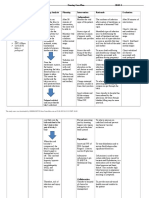
- Client Care Plan: Assessment/Nursing Dx. Outcome Identification/Planning Implementation EvaluationDocument2 pagesClient Care Plan: Assessment/Nursing Dx. Outcome Identification/Planning Implementation EvaluationTiese Lopez79% (14)
- Nursing Care Plan Gestational DiabetesDocument1 pageNursing Care Plan Gestational DiabetesDenise Garcia Molina100% (1)
- IGCSE Biology P42 May2020 QPDocument20 pagesIGCSE Biology P42 May2020 QPPakorn WinayanuwattikunNo ratings yet
- Chapter 6 - Nursing Care For The Family in Need of Reproductive Life PlanningDocument7 pagesChapter 6 - Nursing Care For The Family in Need of Reproductive Life PlanningBern NerquitNo ratings yet
- Pregnancy and LaborDocument9 pagesPregnancy and LaborkurapotaNo ratings yet
- Pi Is 0002937820314228Document2 pagesPi Is 0002937820314228el_dani_ellNo ratings yet
- MLec InterviewDocument3 pagesMLec InterviewAira Galinato CabrasNo ratings yet
- Case StudyDocument2 pagesCase StudyNene TapsNo ratings yet
- PartographDocument6 pagesPartographalyssa marie salcedo100% (1)
- Pregnancy Related ProblemDocument204 pagesPregnancy Related ProblemMannyNo ratings yet
- Gestational Diabetes MellitusDocument7 pagesGestational Diabetes Mellitusعلاوي البرشلونيNo ratings yet
- Reaction Paper On AdvocacyDocument5 pagesReaction Paper On Advocacyapi-32495846150% (6)
- Risk Factors of Hearing Defects and Their Relationship To The Outcome of Hearing Screening Among NeonatesDocument6 pagesRisk Factors of Hearing Defects and Their Relationship To The Outcome of Hearing Screening Among NeonatesRendra SyaniNo ratings yet
- HAP Question Bank Sem 2 B PharmDocument4 pagesHAP Question Bank Sem 2 B PharmJeswin AntoNo ratings yet
- The Natural Diet Solution For PCOS and InfertilityDocument490 pagesThe Natural Diet Solution For PCOS and InfertilityDanutZa Popa100% (1)
- Ovarian Tumours PresentationDocument49 pagesOvarian Tumours PresentationChoden JamyangNo ratings yet
- Klinefelter SyndromeDocument14 pagesKlinefelter SyndromeSisayNo ratings yet
- Meconium Aspiration Syndrome (Daran, Maria Ranela)Document8 pagesMeconium Aspiration Syndrome (Daran, Maria Ranela)Carlojay IniegoNo ratings yet
- Amh 417011Document9 pagesAmh 417011Haider AlmothaferNo ratings yet
- Knowledge About Pregnancy Danger Signs Among MotheDocument7 pagesKnowledge About Pregnancy Danger Signs Among MotheArin RanNo ratings yet
- The RH Factor: How It Can Affect Your PregnancyDocument3 pagesThe RH Factor: How It Can Affect Your PregnancyTedd CamilingNo ratings yet
- Instrument of NormalDocument17 pagesInstrument of NormalEdraline Lumawig100% (2)
- Malpresentation and Malposition Omer Ahmed MirghaniDocument78 pagesMalpresentation and Malposition Omer Ahmed Mirghaniاروى فتح الرحمن100% (1)
- (MCHNLEC) Case Analysis - Mrs. JamiecelDocument2 pages(MCHNLEC) Case Analysis - Mrs. JamiecelTom Cuenca100% (2)
- 1 - Anatomy (STRATOG 2015 SBAs)Document16 pages1 - Anatomy (STRATOG 2015 SBAs)w yNo ratings yet
- Fibriods: PrevalenceDocument5 pagesFibriods: PrevalenceEisha SattarNo ratings yet
- LRR Fmge ObgyDocument63 pagesLRR Fmge ObgyVishal KumarNo ratings yet