You might also like
- BSBDIV501 Student Assessment TasksDocument50 pagesBSBDIV501 Student Assessment TasksÇrox Rmg Punk100% (1)
- Handout 4 - JHA For Replacing Light BulbDocument2 pagesHandout 4 - JHA For Replacing Light Bulbdeby100% (1)
- Bypass Management Practice PDFDocument14 pagesBypass Management Practice PDFSyed Mustafa HussainNo ratings yet
- HowToReadCIStandards PDFDocument1 pageHowToReadCIStandards PDFdeivydejesusNo ratings yet
- NEBOSH IGC2 Past Exam Paper March 2013Document2 pagesNEBOSH IGC2 Past Exam Paper March 2013rexivy88% (8)
- Factors Influencing Compliance To The Jordan PDFDocument7 pagesFactors Influencing Compliance To The Jordan PDFRaed JaradatNo ratings yet
- Personal Protective Equipment Knowledge and Practices Among Nurses Working at Albaha King Fahad Hospital Saudi ArabiaDocument6 pagesPersonal Protective Equipment Knowledge and Practices Among Nurses Working at Albaha King Fahad Hospital Saudi ArabiaGerlan Madrid MingoNo ratings yet
- A Study To Assess The Knowledge and Practices of Hand Hygiene Among Nursing Staff in Different Department of The Hospitals in Uttar PradeshDocument24 pagesA Study To Assess The Knowledge and Practices of Hand Hygiene Among Nursing Staff in Different Department of The Hospitals in Uttar PradeshEditor IJTSRD100% (1)
- Researcharticle Open Access: Tigist EngdaDocument12 pagesResearcharticle Open Access: Tigist EngdasitiNo ratings yet
- Effects of Patient Safety Culture On Patient Satisfaction With Radiological Services in Nigerian Radiodiagnostic PracticeDocument5 pagesEffects of Patient Safety Culture On Patient Satisfaction With Radiological Services in Nigerian Radiodiagnostic PracticeNurul Pratiwi UsmanNo ratings yet
- Knowledge Attitude and Practices Regarding Respiratory SymptomsDocument8 pagesKnowledge Attitude and Practices Regarding Respiratory SymptomsK162404 Nauraiz SubhanNo ratings yet
- A Descriptive Study To Assess The Knowledge Related To Practices of Infection Control Standards Among Staff Nurses in Guru Gobind Singh Medical College and Hospital, Faridkot, PunjabDocument5 pagesA Descriptive Study To Assess The Knowledge Related To Practices of Infection Control Standards Among Staff Nurses in Guru Gobind Singh Medical College and Hospital, Faridkot, PunjabEditor IJTSRDNo ratings yet
- Analysing Hand Hygiene Knowledge and Attitude Among Medical Students and Nursing Staff: Identifying The GapsDocument6 pagesAnalysing Hand Hygiene Knowledge and Attitude Among Medical Students and Nursing Staff: Identifying The GapsIJAR JOURNALNo ratings yet
- Safety and Health at Work: Original ArticleDocument8 pagesSafety and Health at Work: Original ArticleOluwaseun Aderele GabrielNo ratings yet
- COPD 157403 Knowledge and Pharmaceutical Care Practice of Inhaled Therap - 030918Document10 pagesCOPD 157403 Knowledge and Pharmaceutical Care Practice of Inhaled Therap - 030918Rizky Fadhilah87No ratings yet
- F RMHP 265133 Pharmacists Rsquo Perspectives On Providing The Influenza V 62648Document9 pagesF RMHP 265133 Pharmacists Rsquo Perspectives On Providing The Influenza V 62648MB NusairNo ratings yet
- Evaluating The Effectiveness of The "Germ-Free Hands " Intervention For Improving The Hand Hygiene Practices of Public Health StudentsDocument9 pagesEvaluating The Effectiveness of The "Germ-Free Hands " Intervention For Improving The Hand Hygiene Practices of Public Health StudentsnoviaNo ratings yet
- Aplin Snider Et Al 2020 Development and Implementation of An Upper Respiratory Infection Treatment Protocol in ADocument6 pagesAplin Snider Et Al 2020 Development and Implementation of An Upper Respiratory Infection Treatment Protocol in ABBD BBDNo ratings yet
- Comparison Between Pre Post VAP Bundle - Kade Cintya PSDocument6 pagesComparison Between Pre Post VAP Bundle - Kade Cintya PSWidarma Atmaja, I KomangNo ratings yet
- Safety and Health at Work: Original ArticleDocument8 pagesSafety and Health at Work: Original ArticlePractice Medi-nursingNo ratings yet
- 3083 12086 2 PB 1Document10 pages3083 12086 2 PB 1adultnursingspecialtyNo ratings yet
- 15 Perceptions of Infection Control Among Nurses Regarding Barriers A QualitativeDocument6 pages15 Perceptions of Infection Control Among Nurses Regarding Barriers A QualitativemarisaNo ratings yet
- Knowledge of Hand Hygiene and Compliance Among Clinicians - at A Level Six Hospital in Kenya: A Cross Sectional StudyDocument20 pagesKnowledge of Hand Hygiene and Compliance Among Clinicians - at A Level Six Hospital in Kenya: A Cross Sectional StudyIJAR JOURNALNo ratings yet
- Infection Prevention in The Operating Room Anesthesia Work AreaDocument17 pagesInfection Prevention in The Operating Room Anesthesia Work AreaSally Mohy El-DinNo ratings yet
- ASurveyof Handwashing Knowledgeand Attitudesamongthe Healthcare Professionalsin Lahore PakistanDocument7 pagesASurveyof Handwashing Knowledgeand Attitudesamongthe Healthcare Professionalsin Lahore PakistankhadeejakhurshidNo ratings yet
- Do Medical Students Receive Training in Correct Use of Personal Protective EquipmentDocument6 pagesDo Medical Students Receive Training in Correct Use of Personal Protective EquipmentMuhammad zaid RaihanNo ratings yet
- 2901 13196 2 PBDocument8 pages2901 13196 2 PBAndi ZulkifliNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument8 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Mucoactive Agents in The Therapy of Upper Respiratory Airways Infections: Fair To Describe Them Just As Mucoactive?Document9 pagesMucoactive Agents in The Therapy of Upper Respiratory Airways Infections: Fair To Describe Them Just As Mucoactive?Korry Meliana PangaribuanNo ratings yet
- Padilla - The Lived Experience of Nurses Caring For Patients With COVID-19 in Iran: A Phenomenological StudyDocument8 pagesPadilla - The Lived Experience of Nurses Caring For Patients With COVID-19 in Iran: A Phenomenological StudyNicole PadillaNo ratings yet
- Dental Infection and Prevention Control GuidelineDocument7 pagesDental Infection and Prevention Control GuidelineMega ArfiyantiNo ratings yet
- Root Cause Analysis On Hospital Standards and Joint Commission International Standards: A Comparative StudyDocument7 pagesRoot Cause Analysis On Hospital Standards and Joint Commission International Standards: A Comparative StudymarinatariganNo ratings yet
- Fphar 14 1266095Document18 pagesFphar 14 1266095Renal YusufNo ratings yet
- R - Assessment of Knowledge of Staff Nurses Regarding Aseptic Techniques at Selected HospitalDocument6 pagesR - Assessment of Knowledge of Staff Nurses Regarding Aseptic Techniques at Selected HospitalErza GenatrikaNo ratings yet
- Knowledge, Attitude and Practice of Nursing Students Regarding Hand Hygiene in Western Region of NepalDocument6 pagesKnowledge, Attitude and Practice of Nursing Students Regarding Hand Hygiene in Western Region of NepalRochelle GagarinNo ratings yet
- Practice On Pulmonary Hygiene and Associated Factors Among Health Professionals Working in Two Government Hospitals at Amhara, EthiopiaDocument4 pagesPractice On Pulmonary Hygiene and Associated Factors Among Health Professionals Working in Two Government Hospitals at Amhara, EthiopiaayuNo ratings yet
- Awareness, Practices, and Contributing Factors.7Document8 pagesAwareness, Practices, and Contributing Factors.7Sonali SinghNo ratings yet
- Hand Hygiene Guidelines For Front Line Health Care WorkersDocument2 pagesHand Hygiene Guidelines For Front Line Health Care WorkersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- FarmacoviglanciaDocument12 pagesFarmacoviglanciafernandoNo ratings yet
- I-PASS CunaDocument8 pagesI-PASS CunaRafaela Ferreira dos SantosNo ratings yet
- Are Standard Precautions For Hospital Acquired InfectionDocument5 pagesAre Standard Precautions For Hospital Acquired Infectionاحمد العايديNo ratings yet
- 1 s2.0 S2049080121000595 Main1Document6 pages1 s2.0 S2049080121000595 Main1Devina ArrandhikasariNo ratings yet
- Translate PpiDocument8 pagesTranslate PpiHanung FirmanNo ratings yet
- Healthcare Workers' Knowledge, Attitude, and Practice Regarding Personal Protective Equipment For The Prevention of COVID-19Document10 pagesHealthcare Workers' Knowledge, Attitude, and Practice Regarding Personal Protective Equipment For The Prevention of COVID-19NoviNo ratings yet
- Assessment of Knowledge Attitude 603 Satish DeoDocument8 pagesAssessment of Knowledge Attitude 603 Satish Deodesalew bayeNo ratings yet
- 4.original SharifahDocument9 pages4.original Sharifahdebby claudiNo ratings yet
- The Association Between Motivation Prevention and Acceptance Vaccine Services For Prevention and Control of The COVID-19 On University Students in ThailandDocument5 pagesThe Association Between Motivation Prevention and Acceptance Vaccine Services For Prevention and Control of The COVID-19 On University Students in ThailandInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Hand HygieneDocument5 pagesHand Hygieneichoose1996No ratings yet
- Journal Homepage: - : Manuscript HistoryDocument10 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Observational Study of Safe Injection Practices in A Tertiary Care Teaching HospitalDocument5 pagesObservational Study of Safe Injection Practices in A Tertiary Care Teaching HospitalMuhammad HaezarNo ratings yet
- Predictors of Correct Technique in Patients UsingDocument11 pagesPredictors of Correct Technique in Patients UsingPetra ŠalamúnováNo ratings yet
- SSP ArticleDocument6 pagesSSP Articleapi-740259455No ratings yet
- Tate Avila DayDocument1 pageTate Avila DayHemantNo ratings yet
- Ppe-Worldwide ReviewDocument8 pagesPpe-Worldwide ReviewSAJIN ALEXANDERNo ratings yet
- 3133 12312 2 PBDocument7 pages3133 12312 2 PBWawan Febri RamdaniNo ratings yet
- Texto 1Document7 pagesTexto 1Omid Ernesto Chahuaris ChoqueNo ratings yet
- Nurses' Knowledge Regarding Hand Hygiene and Its Individual and Organizational PredictorsDocument9 pagesNurses' Knowledge Regarding Hand Hygiene and Its Individual and Organizational PredictorsMastifa HanasitaNo ratings yet
- Smartphone Text Message Service To Foster Hand Hygiene ComplianceDocument6 pagesSmartphone Text Message Service To Foster Hand Hygiene ComplianceEszter TóthNo ratings yet
- MotivasiDocument5 pagesMotivasiIrfan MadamangNo ratings yet
- Special Issue 1 3Document129 pagesSpecial Issue 1 3Amit PasiNo ratings yet
- Ihy 050Document15 pagesIhy 050Moch Ridwan Pujiar PamungkasNo ratings yet
- Antibiotics Inhalados en NavmDocument10 pagesAntibiotics Inhalados en NavmAnthony Huaman MedinaNo ratings yet
- International Journal of Trend in Scientific Research and Development (IJTSRD)Document4 pagesInternational Journal of Trend in Scientific Research and Development (IJTSRD)Editor IJTSRDNo ratings yet
- Hand Hygiene Compliance, Knowledge and Perception Among Healthcare Workers in A Tertiary Care Center in South IndiaDocument4 pagesHand Hygiene Compliance, Knowledge and Perception Among Healthcare Workers in A Tertiary Care Center in South IndiaIJAR JOURNALNo ratings yet
- J Cherd 2010 08 006Document7 pagesJ Cherd 2010 08 006Terrence Terry BhengoeNo ratings yet
- American Water Works Association Journal (American Water Works Association)Document14 pagesAmerican Water Works Association Journal (American Water Works Association)Terrence Terry BhengoeNo ratings yet
- Chlorine TestingDocument7 pagesChlorine TestingTerrence Terry BhengoeNo ratings yet
- Notice To MembersDocument1 pageNotice To MembersTerrence Terry BhengoeNo ratings yet
- (How To) Calculate The Required Blower Capacity For FBD - Pharma EngineeringDocument11 pages(How To) Calculate The Required Blower Capacity For FBD - Pharma EngineeringTerrence Terry BhengoeNo ratings yet
- FinalReportDraft2019 RahulSinghDocument37 pagesFinalReportDraft2019 RahulSinghTerrence Terry BhengoeNo ratings yet
- J Powtec 2019 03 039Document10 pagesJ Powtec 2019 03 039Terrence Terry BhengoeNo ratings yet
- Minimum and Full Fluidization Velocity For Alumina Used in The Aluminum SmelterDocument7 pagesMinimum and Full Fluidization Velocity For Alumina Used in The Aluminum SmelterTerrence Terry BhengoeNo ratings yet
- Critical Utility Qualification Part IIIDocument14 pagesCritical Utility Qualification Part IIITerrence Terry BhengoeNo ratings yet
- Good Practices in Quality ControlDocument13 pagesGood Practices in Quality ControlTerrence Terry BhengoeNo ratings yet
- Criticial Utility Qualification Part-1Document22 pagesCriticial Utility Qualification Part-1Terrence Terry BhengoeNo ratings yet
- Culture As The Fourth Pillar of Sustainable Development: Olga Helen AstaraDocument10 pagesCulture As The Fourth Pillar of Sustainable Development: Olga Helen AstaraTerrence Terry BhengoeNo ratings yet
- Culture: Fourth Pillar of Sustainable DevelopmentDocument8 pagesCulture: Fourth Pillar of Sustainable DevelopmentTerrence Terry BhengoeNo ratings yet
- Sustainable Development and Concrete Bridges: October 2018Document13 pagesSustainable Development and Concrete Bridges: October 2018Terrence Terry BhengoeNo ratings yet
- Model For Developing Five Key Pillars of Sustainable Tourism: A Literature ReviewDocument17 pagesModel For Developing Five Key Pillars of Sustainable Tourism: A Literature ReviewTerrence Terry BhengoeNo ratings yet
- Pharmaceutical Waste in The Environment: A Cultural PerspectiveDocument6 pagesPharmaceutical Waste in The Environment: A Cultural PerspectiveTerrence Terry BhengoeNo ratings yet
- Contact Derma TitusDocument5 pagesContact Derma TitusTiti PermatasariNo ratings yet
- Abdull DissertationDocument75 pagesAbdull DissertationKahura MundiaNo ratings yet
- Ejemplo de Aplicación 5SDocument19 pagesEjemplo de Aplicación 5Spedro luisNo ratings yet
- Mooring and UnmooringDocument7 pagesMooring and UnmooringDnv Bailey0% (1)
- 122 Health Safty Managment Procedure ManualDocument27 pages122 Health Safty Managment Procedure ManualShams KhattakNo ratings yet
- (EN) Argon, CompressedDocument9 pages(EN) Argon, Compressedmuhammad afiqNo ratings yet
- Detex.Document5 pagesDetex.Ardi ParismanNo ratings yet
- Mikrozid Universal Liquid ENDocument17 pagesMikrozid Universal Liquid ENadriansuvuoNo ratings yet
- Job Hazard Analysis (Jha) Worksheet: Mechanical CleaningDocument5 pagesJob Hazard Analysis (Jha) Worksheet: Mechanical CleaningCain DungauNo ratings yet
- Procedures Manual On Utpras Unified TVET Program Registration and Accreditation System Program Registration (Land-Based)Document60 pagesProcedures Manual On Utpras Unified TVET Program Registration and Accreditation System Program Registration (Land-Based)Valcy MadzNo ratings yet
- Working at Shuttering Yard JSA HSE ProfessionalsDocument2 pagesWorking at Shuttering Yard JSA HSE ProfessionalsViron BaxhiaNo ratings yet
- MSDS of All Listed Chemical in Local LanguageDocument9 pagesMSDS of All Listed Chemical in Local Languagekrishna royNo ratings yet
- Hazardous Substances - Safe Work ProcedureDocument4 pagesHazardous Substances - Safe Work ProcedureMbonise MbojaNo ratings yet
- Quarter 1 - Module 6: Bread and Pastry ProductionDocument20 pagesQuarter 1 - Module 6: Bread and Pastry ProductionHeriza AlcantaraNo ratings yet
- Health Safety and Environment Manual EDDocument167 pagesHealth Safety and Environment Manual EDPAUL ANTIANo ratings yet
- Safety ManualDocument17 pagesSafety ManualArpita Biswas100% (1)
- Cleaning ServiceDocument94 pagesCleaning ServiceYousaf RichuNo ratings yet
- LegislationDocument55 pagesLegislationGabriel FloresNo ratings yet
- Lufkin Risk AssessmentDocument7 pagesLufkin Risk AssessmentmohammedNo ratings yet
- How To Make A Employee Handbook Jess GardnerDocument39 pagesHow To Make A Employee Handbook Jess Gardnerdanyolee1No ratings yet
- Mobl 15W40 SDSDocument9 pagesMobl 15W40 SDSYasser MahmoudNo ratings yet
- OSHA Wallet CardsDocument2 pagesOSHA Wallet CardsbsiofncNo ratings yet
- The Chinese EPCDocument9 pagesThe Chinese EPCAlfredo AstaNo ratings yet
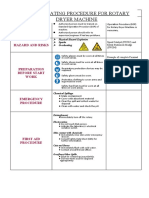
- Safe Operating Procedure For Rotary Dryer Machine: AuthorizationDocument10 pagesSafe Operating Procedure For Rotary Dryer Machine: Authorizationmaizatul ainNo ratings yet
- A Guide To Occupational Health and SafetyDocument12 pagesA Guide To Occupational Health and SafetyIrsyad XioksNo ratings yet