You might also like
- My Mifespristone and Misoprostol Story: How I used mifepristone and misoprostol for a successful medical abortion and all you must know about these abortion pillsFrom EverandMy Mifespristone and Misoprostol Story: How I used mifepristone and misoprostol for a successful medical abortion and all you must know about these abortion pillsNo ratings yet
- Pharma Report Reproductive SystemDocument18 pagesPharma Report Reproductive SystemDolly Jane JavierNo ratings yet
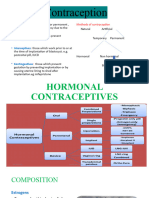
- HORMONAL CONTRACEPTION PresentationDocument25 pagesHORMONAL CONTRACEPTION Presentationjaish8904No ratings yet
- Misoprostol For Treatment of Early Pregnancy LossDocument2 pagesMisoprostol For Treatment of Early Pregnancy LossJuan KipronoNo ratings yet
- Drug Study Rasmien S. JimmyDocument6 pagesDrug Study Rasmien S. JimmyCHRISTINE JOY. MOLINANo ratings yet
- Instructions For Use: Step 1: Step 4Document11 pagesInstructions For Use: Step 1: Step 4Anesh KumarNo ratings yet
- Coc 1Document17 pagesCoc 1Ahmed AnwarNo ratings yet
- Emergency Contraception: "The Morning-After Pill"Document24 pagesEmergency Contraception: "The Morning-After Pill"Dr. Sujnanendra MishraNo ratings yet
- Hormonal ContraceptionDocument13 pagesHormonal ContraceptionAnuradha RoopchandNo ratings yet
- Family Planning: By: Khalid Jemal (MD, Assistant Prof. of Obstetrics & Gynecology)Document73 pagesFamily Planning: By: Khalid Jemal (MD, Assistant Prof. of Obstetrics & Gynecology)Degefaw BikoyNo ratings yet
- Contraception: Heidery - Class DR. Hanaa Al 5 GynaecologyDocument11 pagesContraception: Heidery - Class DR. Hanaa Al 5 Gynaecologyzianab aliNo ratings yet
- Oestrodose Gel Estradiol Hemihydrate SYARIKAT WELLCHEM SDN BHD 4may2017 ENGDocument2 pagesOestrodose Gel Estradiol Hemihydrate SYARIKAT WELLCHEM SDN BHD 4may2017 ENGTQINNo ratings yet
- Drug Acting On UterusDocument12 pagesDrug Acting On UteruskenmanikeseNo ratings yet
- EstradiolDocument5 pagesEstradiolkitsilcNo ratings yet
- Discharge Planning 2Document6 pagesDischarge Planning 2Jason MacatuggalNo ratings yet
- H Receptor AntagonistDocument3 pagesH Receptor AntagonistNicholas TagleNo ratings yet
- PARGAD - CON1A - Module 11 Assignment (Endocrine Drugs and Diabetes Mellitus Drugs)Document9 pagesPARGAD - CON1A - Module 11 Assignment (Endocrine Drugs and Diabetes Mellitus Drugs)Samantha PargadNo ratings yet
- Peptic Ulcer Disease DrugsDocument6 pagesPeptic Ulcer Disease DrugsApple MaeNo ratings yet
- Abnoba ViscumDocument44 pagesAbnoba ViscumAlexandre Funcia100% (1)
- Department of Pharmacy Practice Vels UniversityDocument29 pagesDepartment of Pharmacy Practice Vels UniversityUdtjeVanDerJeykNo ratings yet
- CMCA ASSIGNMENT #1b PDFDocument3 pagesCMCA ASSIGNMENT #1b PDFAyanami PascuaNo ratings yet
- Progestin-Only Injectables Fact Sheet Final - 102510Document2 pagesProgestin-Only Injectables Fact Sheet Final - 102510Chan Myae AungNo ratings yet
- Clomiphene Med CardDocument1 pageClomiphene Med CardLisa AnneNo ratings yet
- Dosing of Ivermectin & Other TherapeuticsDocument7 pagesDosing of Ivermectin & Other TherapeuticsTom100% (2)
- Animal Birth ControlDocument15 pagesAnimal Birth Controlvenku07484435No ratings yet
- Data Collection 1Document5 pagesData Collection 1api-382265951No ratings yet
- Oxytocin and Drugs Acting On The UterusDocument56 pagesOxytocin and Drugs Acting On The UterusKasturiRangan SrivatsaNo ratings yet
- ImplantsDocument11 pagesImplantsraheelNo ratings yet
- Family Planning1Document63 pagesFamily Planning1Deborah AmpongNo ratings yet
- 13 FPDocument32 pages13 FPDawit g/kidanNo ratings yet
- HRT Dosing GuideDocument5 pagesHRT Dosing GuideBAMNo ratings yet
- Emistat Oral InsDocument1 pageEmistat Oral InsnajmulkutubiNo ratings yet
- No SpaDocument6 pagesNo SpaIlyes FerenczNo ratings yet
- EstradiolDocument1 pageEstradiol3S - JOCSON, DENESE NICOLE LEE M.No ratings yet
- كونتر اسبتفDocument40 pagesكونتر اسبتفAlaa MahdiNo ratings yet
- ContraceptionDocument53 pagesContraceptionfiea241089100% (6)
- Pentasa LeafletDocument2 pagesPentasa LeafletreadalotbutnowisdomyetNo ratings yet
- Drugs Used in Pediatrics: Criteria For Dose CalculationDocument21 pagesDrugs Used in Pediatrics: Criteria For Dose CalculationSanthosh.S.U100% (4)
- Class PrescriptionsDocument12 pagesClass PrescriptionsShirsh JauriharNo ratings yet
- Contraception Part 1Document50 pagesContraception Part 1Aman ShaikhNo ratings yet
- PRK Post-Operative Instructions: Please NoteDocument2 pagesPRK Post-Operative Instructions: Please NoteHaris UmairNo ratings yet
- Presentation 1Document12 pagesPresentation 1shekharkhadka2057No ratings yet
- Drug Study: PART 1: To Be Completed Prior To Clinical ExperienceDocument5 pagesDrug Study: PART 1: To Be Completed Prior To Clinical ExperienceFrozanSNo ratings yet
- OxytocinDocument1 pageOxytocinIvanne Hisoler100% (7)
- PRK Postop InstructionsDocument2 pagesPRK Postop Instructionspchengs6phNo ratings yet
- Summary of Product CharacteristicsDocument11 pagesSummary of Product Characteristicsdea chammearcNo ratings yet
- Panunumpa NG PropesyonalDocument5 pagesPanunumpa NG PropesyonalJustin DiazNo ratings yet
- Methylergonovine MaleateDocument2 pagesMethylergonovine MaleateRitamariaNo ratings yet
- Oral Hormonal Contraceptive: BY Magdyabdelrahmanmohamed 2 0 1 5Document36 pagesOral Hormonal Contraceptive: BY Magdyabdelrahmanmohamed 2 0 1 5UdtjeVanDerJeykNo ratings yet
- Case AnalysisDocument2 pagesCase AnalysisYeng MangilitNo ratings yet
- Gynecology - ContraceptionDocument10 pagesGynecology - ContraceptionparaschoumariaNo ratings yet
- 4th Year - Unit 5 - Pharmacotherapeutics in Obstetrics 1Document13 pages4th Year - Unit 5 - Pharmacotherapeutics in Obstetrics 1Rupa Ghosh100% (1)
- Guidelines Ut I 2012Document1 pageGuidelines Ut I 2012Siti ZulaikhahNo ratings yet
- Drug Study For OxytocinDocument2 pagesDrug Study For OxytocinAngelica CorpuzNo ratings yet
- On Nursing Responsibilities of Drugs in ObstetricsDocument117 pagesOn Nursing Responsibilities of Drugs in ObstetricsSanjita Kumari PanditNo ratings yet
- Drug Study On Labor and DeliveryDocument4 pagesDrug Study On Labor and DeliveryJune Dumdumaya67% (3)
- Fynadine 20mgDocument2 pagesFynadine 20mgNgo Van TruongNo ratings yet
- Medication Exercise Treatment Hygiene Outpatient Diet: Generic Name: Methylergonovine Brand Name: MethergineDocument2 pagesMedication Exercise Treatment Hygiene Outpatient Diet: Generic Name: Methylergonovine Brand Name: MethergineZoe Dominique GudioNo ratings yet
- Norpill: Levonorgestrel 1.5 MGDocument1 pageNorpill: Levonorgestrel 1.5 MGShad RahmanNo ratings yet
- Clinical Practice Guideline For The Management ofDocument51 pagesClinical Practice Guideline For The Management ofneleatucicovshiiNo ratings yet
- Vanschalkwyk2015 VV PDFDocument9 pagesVanschalkwyk2015 VV PDFAulia RahmaNo ratings yet
- Combined HormonalDocument108 pagesCombined HormonalneleatucicovshiiNo ratings yet
- Metronidazole Vaginal Gel 075Document6 pagesMetronidazole Vaginal Gel 075neleatucicovshiiNo ratings yet
- Management of Infection Guidance For Primary Care For Consultation and Local Adaptation - July 2015Document66 pagesManagement of Infection Guidance For Primary Care For Consultation and Local Adaptation - July 2015neleatucicovshiiNo ratings yet
- Oxfordshire-Antimicrobial-ADULT-Guidelines-Primary-Care - 2014Document38 pagesOxfordshire-Antimicrobial-ADULT-Guidelines-Primary-Care - 2014neleatucicovshiiNo ratings yet
- Core Safety ProfileDocument13 pagesCore Safety ProfileneleatucicovshiiNo ratings yet
- FLC Versus AlteleDocument4 pagesFLC Versus AlteleneleatucicovshiiNo ratings yet
- Committee Opinion: Solutions For Surgical Preparation of The VaginaDocument3 pagesCommittee Opinion: Solutions For Surgical Preparation of The VaginaneleatucicovshiiNo ratings yet
- Estriol Ema 2004Document14 pagesEstriol Ema 2004neleatucicovshiiNo ratings yet
- Antimicrob. Agents Chemother.-2011-Carrillo-Muсoz-AAC.00219-11Document13 pagesAntimicrob. Agents Chemother.-2011-Carrillo-Muсoz-AAC.00219-11neleatucicovshiiNo ratings yet
- ContraceptiveDocument4 pagesContraceptiveneleatucicovshiiNo ratings yet
- 02 Antimicrobial AgentsDocument10 pages02 Antimicrobial AgentssandipladaniNo ratings yet
- Efficacy of Vaginal Probiotic Capsules For Recurrent PDFDocument6 pagesEfficacy of Vaginal Probiotic Capsules For Recurrent PDFneleatucicovshiiNo ratings yet
- Canesten Clotrimazole Vaginal Products: Rescheduling Application ForDocument38 pagesCanesten Clotrimazole Vaginal Products: Rescheduling Application ForneleatucicovshiiNo ratings yet
- JPM 05 00050Document17 pagesJPM 05 00050mstNo ratings yet
- Clinical Trial - Use of Oral Probiotics As An Adjunctive Therapy To Fluconazole in The Treatment of Yeast VaginitisDocument3 pagesClinical Trial - Use of Oral Probiotics As An Adjunctive Therapy To Fluconazole in The Treatment of Yeast VaginitisneleatucicovshiiNo ratings yet
- 1-Dragana Skokovic-Probio 2015 enDocument35 pages1-Dragana Skokovic-Probio 2015 enneleatucicovshiiNo ratings yet
- Finasteride 5 MG Tablets - Summary of Product Characteristics (SPC) - (eMC)Document6 pagesFinasteride 5 MG Tablets - Summary of Product Characteristics (SPC) - (eMC)neleatucicovshiiNo ratings yet
- 1309 Ovestin 1332242478Document9 pages1309 Ovestin 1332242478neleatucicovshiiNo ratings yet
- Efficacy of Vaginal Probiotic Capsules For RecurrentDocument6 pagesEfficacy of Vaginal Probiotic Capsules For RecurrentneleatucicovshiiNo ratings yet
- Clinical StudyDocument7 pagesClinical StudyneleatucicovshiiNo ratings yet
- Antibiotic Resistance of Lactic Acid Bacteria PDFDocument8 pagesAntibiotic Resistance of Lactic Acid Bacteria PDFneleatucicovshiiNo ratings yet
- Clinical StudyDocument7 pagesClinical StudyneleatucicovshiiNo ratings yet
- 2103 Efficacy of Vitamin C Vaginal Suppository in Treatment of Bacterial Vaginosis A Randomized Controlled TrialDocument6 pages2103 Efficacy of Vitamin C Vaginal Suppository in Treatment of Bacterial Vaginosis A Randomized Controlled TrialneleatucicovshiiNo ratings yet
- Efficacy of Oral Metronidazole With Vaginal Clindamycin or Vaginal Probiotic For Bacterial Vaginosis - Randomised Placebo-Controlled Double-Blind TrialDocument11 pagesEfficacy of Oral Metronidazole With Vaginal Clindamycin or Vaginal Probiotic For Bacterial Vaginosis - Randomised Placebo-Controlled Double-Blind TrialneleatucicovshiiNo ratings yet
- Canadian Contraception ConsensusDocument3 pagesCanadian Contraception ConsensusneleatucicovshiiNo ratings yet
- Best of The 2001 AUA Annual MeetingDocument14 pagesBest of The 2001 AUA Annual MeetingneleatucicovshiiNo ratings yet
- Efficacy of Oral Metronidazole With Vaginal Clindamycin or Vaginal Probiotic For Bacterial Vaginosis - Randomised Placebo-Controlled Double-Blind TrialDocument11 pagesEfficacy of Oral Metronidazole With Vaginal Clindamycin or Vaginal Probiotic For Bacterial Vaginosis - Randomised Placebo-Controlled Double-Blind TrialneleatucicovshiiNo ratings yet
- DAOC in Extremes of Weight, Renal and Hepatic ImpairmentDocument14 pagesDAOC in Extremes of Weight, Renal and Hepatic ImpairmentHemanthi JettiNo ratings yet
- DVT 2600 Manual de UsoDocument28 pagesDVT 2600 Manual de UsoJUAN REYESNo ratings yet
- Transgender Women - Evaluation and Management - UpToDateDocument29 pagesTransgender Women - Evaluation and Management - UpToDateRicardo Alessandro Teixeira Gonsaga0% (1)
- Emboli ParuDocument61 pagesEmboli ParuAndrew MakariosNo ratings yet
- Warfarin CoumadinDocument1 pageWarfarin CoumadinE100% (5)
- 2020 Medical GuidelinesDocument406 pages2020 Medical Guidelinesanitn2020No ratings yet
- Initial Assessment and Management of Acute StrokeDocument49 pagesInitial Assessment and Management of Acute StrokeIrina DuceacNo ratings yet
- Contraception in Women Over 40 Years ofDocument9 pagesContraception in Women Over 40 Years ofAndhika MaulinaNo ratings yet
- Oral Anticoagulation in The Elderly and Frail: Rupert M. Bauersachs Joerg HeroldDocument10 pagesOral Anticoagulation in The Elderly and Frail: Rupert M. Bauersachs Joerg Herold90STRATOVARIUS90No ratings yet
- First Aid '20: Osmosis VideosDocument55 pagesFirst Aid '20: Osmosis VideosJulien ClaireNo ratings yet
- DVTDocument13 pagesDVTapi-253732526No ratings yet
- CPG - Prevention Treatment VTE 2013 PDFDocument170 pagesCPG - Prevention Treatment VTE 2013 PDFUmmu SolahNo ratings yet
- PFO-AHA Guidelines 2020 PDFDocument11 pagesPFO-AHA Guidelines 2020 PDFsdfasdfasdfadfsNo ratings yet
- Pulmonary EmbolismDocument93 pagesPulmonary EmbolismRakesh PanchalNo ratings yet
- Antifosfolipidni SindromDocument12 pagesAntifosfolipidni SindromSlobodan ObradovicNo ratings yet
- 10.1007@s00266 019 01576 2Document10 pages10.1007@s00266 019 01576 2Antonio CardenasNo ratings yet
- High Definition Liposculpture 18 Year Evolution .12Document11 pagesHigh Definition Liposculpture 18 Year Evolution .12drhestrellaNo ratings yet
- Euab 065Document65 pagesEuab 065Mathew McCarthyNo ratings yet
- Module 3 ReviDocument35 pagesModule 3 ReviJohn Van Dave TaturoNo ratings yet
- Nursing Board Review: Cardiovascular SystemDocument237 pagesNursing Board Review: Cardiovascular SystemsenthilmnurseNo ratings yet
- STD Heparin Protocol MethodistDocument1 pageSTD Heparin Protocol Methodistd40sithuiNo ratings yet
- A Single Preoperative Dose of Tranexamic Acid Reduces Perioperative Blood LossDocument7 pagesA Single Preoperative Dose of Tranexamic Acid Reduces Perioperative Blood LossCarlosA.DíazNo ratings yet
- Medicine CPC ScriptDocument4 pagesMedicine CPC ScriptMarco Paulo Reyes NaoeNo ratings yet
- ccpc15 Supportive and Preventive WorkbookDocument30 pagesccpc15 Supportive and Preventive WorkbookJeremy HamptonNo ratings yet
- VT Guidelines PDFDocument74 pagesVT Guidelines PDFgabrimarteNo ratings yet
- Initial Assessment and Management of Acute Stroke - UpToDateDocument27 pagesInitial Assessment and Management of Acute Stroke - UpToDateDiego VillacisNo ratings yet
- Drug Study HeparinDocument2 pagesDrug Study HeparinArianne NicoleNo ratings yet
- Careplan 5 MedsurgDocument8 pagesCareplan 5 Medsurgapi-509642710No ratings yet
- Acpimks: HematologyDocument147 pagesAcpimks: HematologyPaulo VizcardoNo ratings yet
- Guias Europeas TEP 2019Document61 pagesGuias Europeas TEP 2019Sebastian PosadaNo ratings yet