You might also like
- Lymphatic System ReviewerDocument49 pagesLymphatic System ReviewerJess Lejarde100% (1)
- Massachusetts immunization certificate guideDocument1 pageMassachusetts immunization certificate guidePrecilla Janet RosarioNo ratings yet
- (BCA 3) Respiratory Physiology (Dr. Mendoza)Document9 pages(BCA 3) Respiratory Physiology (Dr. Mendoza)Carla P100% (1)
- Lymphatic System GuideDocument9 pagesLymphatic System GuideKimberly Joy Gregorio100% (1)
- Histology Lab Samplex RationaleDocument13 pagesHistology Lab Samplex RationaleFrances Dei100% (1)
- Physiology LE3 Samplex 2017BDocument8 pagesPhysiology LE3 Samplex 2017BAxel Alvaran100% (1)
- Pharmacotherapy of Diabetes MellitusDocument8 pagesPharmacotherapy of Diabetes MellitusSheryl Layne Lao-SebrioNo ratings yet
- Nursing Care of The High Risk NewbornDocument8 pagesNursing Care of The High Risk NewbornFebie GonzagaNo ratings yet
- REV Micro HSB RemedsDocument16 pagesREV Micro HSB RemedsPatricia HariramaniNo ratings yet
- JRRMMC Biochem Exam Answer KeyDocument4 pagesJRRMMC Biochem Exam Answer KeyBom Tna100% (2)
- Pharmacology Finals ReviewDocument2 pagesPharmacology Finals ReviewVince CabahugNo ratings yet
- Portal Hypertension - A Case ReportDocument65 pagesPortal Hypertension - A Case ReportTEAM K 1920No ratings yet
- Obstetrics Midterms Rationale 2nd Sem 2018 2019Document21 pagesObstetrics Midterms Rationale 2nd Sem 2018 2019Gene Paulo UyNo ratings yet
- Chapter 24)Document10 pagesChapter 24)Hazel LopezNo ratings yet
- Anesth BarashDocument6 pagesAnesth BarashIAN GABRIELLE MERCADO CUYNONo ratings yet
- Disorders of Purine and Pyrimidine MetabolismDocument17 pagesDisorders of Purine and Pyrimidine Metabolismtanmay mehtaNo ratings yet
- Hypoxia and CyanosisDocument33 pagesHypoxia and CyanosisRamlah IbrahimNo ratings yet
- Phenylalanine and Tyrosine Metabolism (18 Oct)Document14 pagesPhenylalanine and Tyrosine Metabolism (18 Oct)api-19824406100% (6)
- Patho. Reviewer On Cellular InjuryDocument21 pagesPatho. Reviewer On Cellular InjurySeff CausapinNo ratings yet
- Migs (With Summary) +paoDocument6 pagesMigs (With Summary) +paoMigs MedinaNo ratings yet
- Integration of Metabolism Integration of MetabolismDocument10 pagesIntegration of Metabolism Integration of MetabolismEdison LucianoNo ratings yet
- Most Common Complication: Sabay SilaDocument6 pagesMost Common Complication: Sabay SilaSheryl Layne Lao-SebrioNo ratings yet
- Calcium, Magnesium, and Potassium Homeostasis: OutlineDocument10 pagesCalcium, Magnesium, and Potassium Homeostasis: OutlineMigs MedinaNo ratings yet
- Protein MetabolismDocument24 pagesProtein MetabolismSohail PattanNo ratings yet
- 1 Digestive System DevelopmentDocument3 pages1 Digestive System DevelopmentDianne IgnacioNo ratings yet
- Pediatric Fluid ReplacementDocument2 pagesPediatric Fluid ReplacementLori Arney100% (1)
- Biochem 1.5 Bioenergetics PDFDocument7 pagesBiochem 1.5 Bioenergetics PDFlovelots1234No ratings yet
- Consensus guidelines for treatment of pediatric nephrotic syndromeDocument14 pagesConsensus guidelines for treatment of pediatric nephrotic syndromeSara Ilyas KhanNo ratings yet
- 2023.LabDx - Trans02.Hemostasis and ThrombosisDocument4 pages2023.LabDx - Trans02.Hemostasis and ThrombosisstellaNo ratings yet
- CPG Childhood ImmunizationDocument25 pagesCPG Childhood ImmunizationLady Nur StarkNo ratings yet
- BioChemistry Syllabus and MQPs 08012018Document33 pagesBioChemistry Syllabus and MQPs 08012018rupaNo ratings yet
- Intrauterine Fetal Transfusion of Red Blood CellsDocument16 pagesIntrauterine Fetal Transfusion of Red Blood CellsHervi LaksariNo ratings yet
- Osce Cranial Nerves PDFDocument42 pagesOsce Cranial Nerves PDFriczen vilaNo ratings yet
- Biochemistry Notes For BoardsDocument35 pagesBiochemistry Notes For BoardsUjjwal PyakurelNo ratings yet
- 2 0CommDiseaseIMPTVisionDocument3 pages2 0CommDiseaseIMPTVisionAndrea Patricia DaquialNo ratings yet
- Glycogenolysis BreakdownDocument6 pagesGlycogenolysis BreakdownManila MedNo ratings yet
- NSAIDs, DMARDs & Antigout1Document69 pagesNSAIDs, DMARDs & Antigout1Melissa SalayogNo ratings yet
- Respiratory Notes and SlideDocument33 pagesRespiratory Notes and SlideChristina Gonez100% (1)
- Protein Energy MalnutritionDocument16 pagesProtein Energy MalnutritionAisha Abdullah ManzurNo ratings yet
- PCAP guidelines update (2016Document3 pagesPCAP guidelines update (2016Roy Anthony CenizaNo ratings yet
- Thalassemia: An Overview of the Genetic Blood DisorderDocument164 pagesThalassemia: An Overview of the Genetic Blood DisorderMohd Anas SheikhNo ratings yet
- Thalassemia TableDocument2 pagesThalassemia TableMeevie ToledoNo ratings yet
- Autonomic DrugsDocument4 pagesAutonomic DrugsSabrinaNo ratings yet
- S2-OB-Maternal Physio PDFDocument14 pagesS2-OB-Maternal Physio PDFSheena PasionNo ratings yet
- GluconeogenesisDocument11 pagesGluconeogenesisMithilesh RautNo ratings yet
- Pathophysiology of Short Stature (Specifically in Children)Document16 pagesPathophysiology of Short Stature (Specifically in Children)Dennis SukadanaNo ratings yet
- Amino Acids Building Blocks of ProteinsDocument12 pagesAmino Acids Building Blocks of ProteinsJearnie Lou Arroyo100% (1)
- Selected antibacterial antibiotics mechanisms and examplesDocument4 pagesSelected antibacterial antibiotics mechanisms and examplesTJNo ratings yet
- Reviewer For Pedia Osce: 10.5 KG 45.16 CM / 17.8 in 75 CM SixDocument10 pagesReviewer For Pedia Osce: 10.5 KG 45.16 CM / 17.8 in 75 CM SixJamora ManilynNo ratings yet
- PharmDrug List Complete SGU-USTDocument116 pagesPharmDrug List Complete SGU-USTMary Camille AzarconNo ratings yet
- Enhancement Course For Clerks Biochem Examination Part 2Document3 pagesEnhancement Course For Clerks Biochem Examination Part 2Kevin Alonzo100% (1)
- Case Presentation: NeurologyDocument19 pagesCase Presentation: NeurologySydrex SarmientoNo ratings yet
- MSPH Biostatistics FlyerDocument2 pagesMSPH Biostatistics FlyerJoyce MalitNo ratings yet
- Classification of The Epilepsies: Purpose: For Clinical DiagnosisDocument25 pagesClassification of The Epilepsies: Purpose: For Clinical Diagnosisayu rifqiNo ratings yet
- Path Concept MapsDocument113 pagesPath Concept MapsAndleeb ImranNo ratings yet
- 11 - Hemostasis & Blood CoagulationDocument66 pages11 - Hemostasis & Blood CoagulationISRAELNo ratings yet
- TOPNOTCH MEDICAL BOARD PREP BIOCHEMISTRY HANDOUTDocument46 pagesTOPNOTCH MEDICAL BOARD PREP BIOCHEMISTRY HANDOUTJohn RamosNo ratings yet
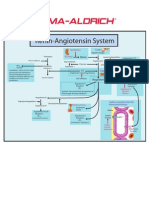
- Renin-Angiotensin SystemDocument1 pageRenin-Angiotensin SystemSigma-Aldrich100% (2)
- LECTURE 12 NITROGEN DEGRATIONDocument28 pagesLECTURE 12 NITROGEN DEGRATIONBiology BảoNo ratings yet
- Amino Acid Oxidation and The Production PDFDocument34 pagesAmino Acid Oxidation and The Production PDFNini BesiNo ratings yet
- University of The East Ramon Magsaysay Memorial Medical Center Department of Biochemistry QUIZ # 5 NAME: - SECTION A DATE: - Topic: FA SynthesisDocument3 pagesUniversity of The East Ramon Magsaysay Memorial Medical Center Department of Biochemistry QUIZ # 5 NAME: - SECTION A DATE: - Topic: FA SynthesisManila MedNo ratings yet
- A Blessed Merry Christmas and A Prosperous New Year To All!!!!Document13 pagesA Blessed Merry Christmas and A Prosperous New Year To All!!!!Manila MedNo ratings yet
- Dunfa Scientifc MethoDocument4 pagesDunfa Scientifc MethoManila MedNo ratings yet
- FA Synth3sDocument2 pagesFA Synth3sManila MedNo ratings yet
- Lipid metabolism and transport pathwaysDocument1 pageLipid metabolism and transport pathwaysManila MedNo ratings yet
- 2.01 Medieval Period and Renaissance: OutlineDocument5 pages2.01 Medieval Period and Renaissance: OutlineManila MedNo ratings yet
- Scientific Revolution and the Rise of Germ TheoryDocument3 pagesScientific Revolution and the Rise of Germ TheoryManila MedNo ratings yet
- Histry of MedcnDocument3 pagesHistry of MedcnManila MedNo ratings yet
- Glycogenolysis BreakdownDocument6 pagesGlycogenolysis BreakdownManila MedNo ratings yet
- Lipid Chemistry: BiochemistryDocument14 pagesLipid Chemistry: BiochemistryManila Med0% (1)
- Citrc Acd CycleDocument46 pagesCitrc Acd CycleManila MedNo ratings yet
- Gluconeogenesis: An Overview of Glucose Formation from Non-Carbohydrate SourcesDocument10 pagesGluconeogenesis: An Overview of Glucose Formation from Non-Carbohydrate SourcesManila Med100% (1)
- The Physician As A Rural Practitioner: History!And!Perspective !In!MedicineDocument2 pagesThe Physician As A Rural Practitioner: History!And!Perspective !In!MedicineManila MedNo ratings yet
- EarlyAncint CvlizationsDocument5 pagesEarlyAncint CvlizationsManila MedNo ratings yet
- Pyruvate Dehydrogenase Complex and the Tricarboxylic Acid CycleDocument9 pagesPyruvate Dehydrogenase Complex and the Tricarboxylic Acid CycleManila MedNo ratings yet
- 2 Long Exam Feedback: BiochemistryDocument7 pages2 Long Exam Feedback: BiochemistryManila MedNo ratings yet
- Juan Dela Cruz, MD - August 10, 2018: LE TransDocument2 pagesJuan Dela Cruz, MD - August 10, 2018: LE TransManila MedNo ratings yet
- Immunity Overview: Innate vs AdaptiveDocument13 pagesImmunity Overview: Innate vs AdaptiveManila MedNo ratings yet
- Hemostasis and Thrombosis: OutlineDocument11 pagesHemostasis and Thrombosis: OutlineManila MedNo ratings yet
- Carbohydrate Chemistry Digestion and TransportDocument14 pagesCarbohydrate Chemistry Digestion and TransportManila MedNo ratings yet
- Salivary Amylase Activity FactorsDocument5 pagesSalivary Amylase Activity FactorsManila MedNo ratings yet
- Platelts and CoaglatinDocument7 pagesPlatelts and CoaglatinManila MedNo ratings yet
- Uronc PathwayDocument11 pagesUronc PathwayManila MedNo ratings yet
- Chromatography Techniques for Separating Amino AcidsDocument4 pagesChromatography Techniques for Separating Amino AcidsManila MedNo ratings yet
- Red Blood Cell Metabolism: Outline A. Blood ChemistryDocument11 pagesRed Blood Cell Metabolism: Outline A. Blood ChemistryManila MedNo ratings yet
- HexhoseDocument12 pagesHexhoseManila MedNo ratings yet
- Intro To Metabo (IsmDocument8 pagesIntro To Metabo (IsmManila MedNo ratings yet
- Enzymes: OutlineDocument10 pagesEnzymes: OutlineManila MedNo ratings yet
- HtwoO and BufferDocument7 pagesHtwoO and BufferManila MedNo ratings yet
- Bioenergetics: OutlineDocument8 pagesBioenergetics: OutlineManila MedNo ratings yet
- Amino AcidDocument2 pagesAmino AcidMervinlloyd Allawan BayhonNo ratings yet
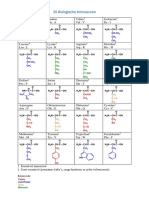
- 20 Biologische Aminozuren: Asparaginezuur Asp DDocument2 pages20 Biologische Aminozuren: Asparaginezuur Asp Detienne.jooken8734No ratings yet
- Appendix I: IA IUPAC Nucleotide Ambiguity CodesDocument2 pagesAppendix I: IA IUPAC Nucleotide Ambiguity Codespeeps007No ratings yet
- Amino Acids: The Building Blocks of ProteinsDocument133 pagesAmino Acids: The Building Blocks of ProteinsAfnankh698No ratings yet
- Periodic Chart of Amino AcidsDocument1 pagePeriodic Chart of Amino AcidsKatherin100% (1)
- HARPERS - VI Biosynthesis of Nutritionally Nonessential Amino AcidsDocument2 pagesHARPERS - VI Biosynthesis of Nutritionally Nonessential Amino AcidsdandiNo ratings yet
- Amino Acid Racemization DatingDocument39 pagesAmino Acid Racemization DatingSean Pitman, MD100% (1)
- BIOCHEM FR 2 Qualitative Color ReactionsDocument6 pagesBIOCHEM FR 2 Qualitative Color ReactionsJNo ratings yet
- Amino AcidDocument64 pagesAmino AcidGon FreecssNo ratings yet
- Brazilian Tables For Poultry and Swine: Feedstuff Composition and Nutritional RequirementsDocument482 pagesBrazilian Tables For Poultry and Swine: Feedstuff Composition and Nutritional RequirementsInzamamUlHaq100% (1)
- 720006487en PDFDocument10 pages720006487en PDF--No ratings yet
- Formula of The 20 Common Amino AcidsDocument11 pagesFormula of The 20 Common Amino AcidsAngelica AngelesNo ratings yet
- Biochem CH 24 Amino Acid BiosynthesisDocument6 pagesBiochem CH 24 Amino Acid BiosynthesisSchat ZiNo ratings yet
- Asparagina 2Document15 pagesAsparagina 2Daniela SepulvedaNo ratings yet
- Biochemistry Notes ProteinsDocument6 pagesBiochemistry Notes ProteinsRegine ChuaNo ratings yet
- DNA and DestinyDocument26 pagesDNA and DestinyGN100% (1)
- AA BiosynthesisDocument69 pagesAA BiosynthesisSajid NabiNo ratings yet
- 20 Common Amino Acids v2 PDFDocument1 page20 Common Amino Acids v2 PDFRenaldy NugrahaNo ratings yet
- Old Data BookletDocument12 pagesOld Data BookletMohamed MawasNo ratings yet
- Mind Map: Amino Acid MetabolismDocument1 pageMind Map: Amino Acid MetabolismAbbey Ayala100% (1)
- A Review of Current Methods For The Determination of Acrylamide in Food ProductsDocument11 pagesA Review of Current Methods For The Determination of Acrylamide in Food ProductsdiaznufioNo ratings yet
- Origins of Names of Protein Amino AcidsDocument1 pageOrigins of Names of Protein Amino AcidsadirmeedanNo ratings yet
- Pharmaceutical Biochemistry (PACOP RED) ANSWER SHEETDocument20 pagesPharmaceutical Biochemistry (PACOP RED) ANSWER SHEETBRYAN BALDOMERONo ratings yet
- Applications of Metabolomics To Study Cancer MetabolismDocument13 pagesApplications of Metabolomics To Study Cancer Metabolismyylf2016No ratings yet
- Table of Standard Amino Acid Abbreviations and Side Chain PropertiesDocument9 pagesTable of Standard Amino Acid Abbreviations and Side Chain PropertieschaitanyasakhNo ratings yet
- Chapter Three Amino Acids and Peptides: Mary K. Campbell Shawn O. FarrellDocument23 pagesChapter Three Amino Acids and Peptides: Mary K. Campbell Shawn O. FarrellsaddamixoNo ratings yet
- Veganissimo A To Z ExcerptDocument25 pagesVeganissimo A To Z ExcerptThe Experiment100% (1)
- Amino Acids, Proteins, and EnzymesDocument62 pagesAmino Acids, Proteins, and Enzymesendale gebregzabherNo ratings yet
- Nitrogen Containing Compounds: Amino AcidsDocument10 pagesNitrogen Containing Compounds: Amino AcidsakshodhiniNo ratings yet
- Amino Acid AnalysisDocument24 pagesAmino Acid AnalysisalaafathyNo ratings yet